

- Department of Neurosurgery, Medical College of Wisconsin, Milwaukee, Wisconsin, USA
- Department of Neurology, St. Vincent Mercy Hospital, Toledo, Ohio, USA
Correspondence Address:
Ha Son Nguyen
Department of Neurology, St. Vincent Mercy Hospital, Toledo, Ohio, USA
DOI:10.4103/2152-7806.187490
Copyright: © 2016 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Nguyen HS, Doan N, Shabani S, Gelsomino M, Zaidat O. Pure tentorial subdural hematoma from rupture of aneurysm along the transmastoid branches of the occipital artery. Surg Neurol Int 01-Aug-2016;7:
How to cite this URL: Nguyen HS, Doan N, Shabani S, Gelsomino M, Zaidat O. Pure tentorial subdural hematoma from rupture of aneurysm along the transmastoid branches of the occipital artery. Surg Neurol Int 01-Aug-2016;7:. Available from: http://surgicalneurologyint.com/surgicalint_articles/pure-tentorial-subdural-hematoma-rupture-aneurysm-along-transmastoid-branches-occipital-artery/
Abstract
Background:Pure subdural hematoma (without subarachnoid, intraventricular, or intraparenchymal hemorrhage) due to a ruptured intracranial aneurysm is rare. Most reported cases involve an aneurysm along the internal carotid artery, posterior communicating artery, or middle cerebral artery. No reports have described an aneurysm along the transmastoid branches of the occipital artery.
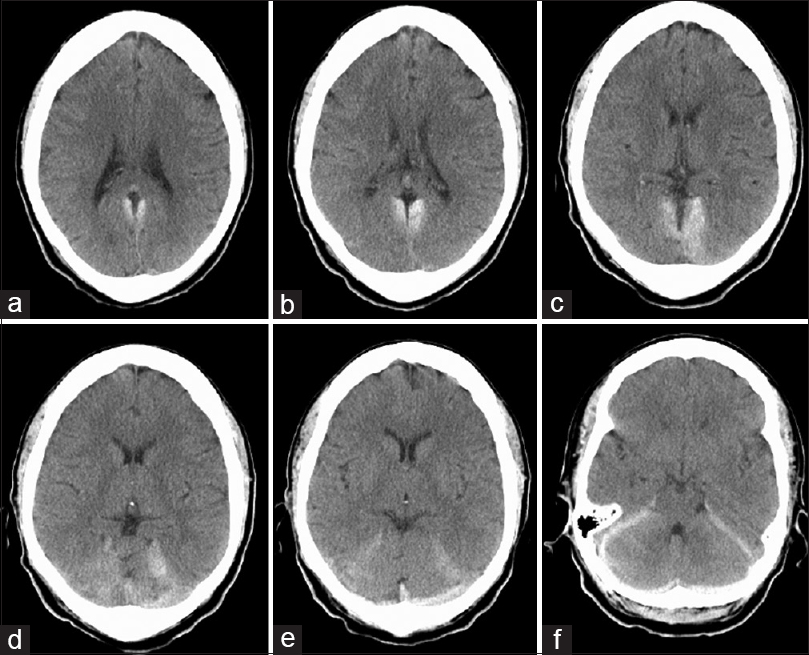
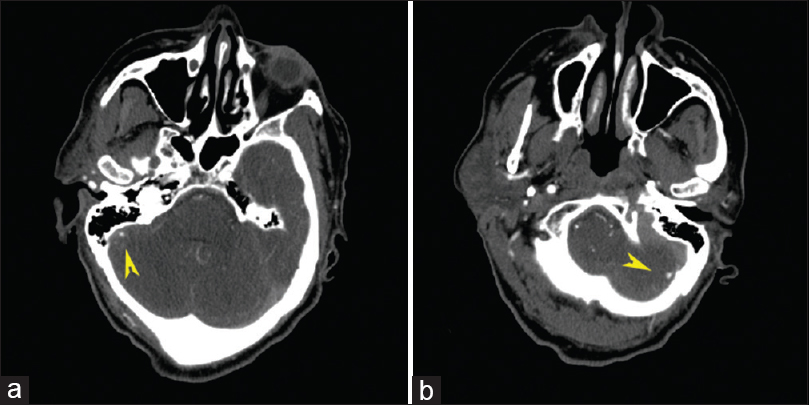
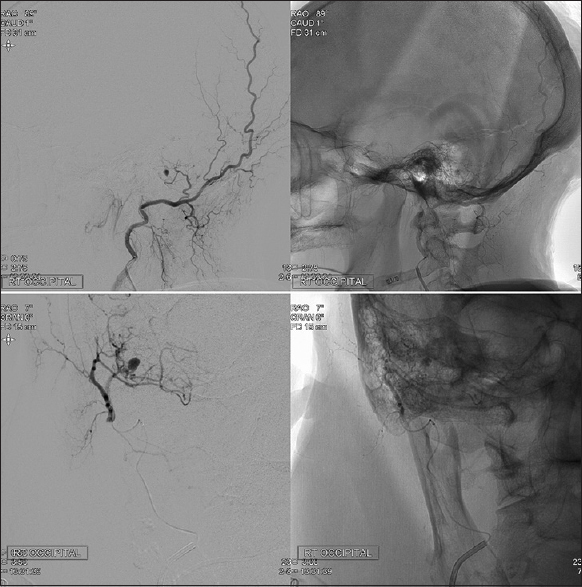
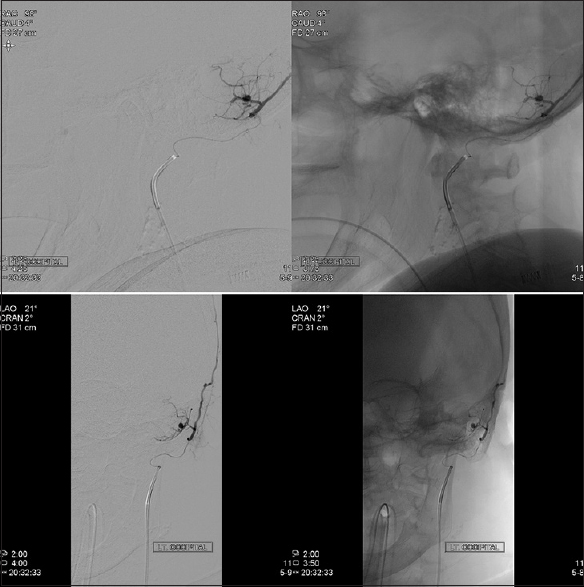
Case Description:A 70-year-old female presented with sudden-onset, excruciating headaches, associated with dizziness, nausea, and emesis. There was no history of trauma. Computed tomography (CT) head demonstrated a pure tentorial subdural hematoma. Vascular imaging revealed bilateral aneurysms along the transmastoid branches of the intracranial portion of both the occipital arteries. Consequently, these branches were embolized, with no residual filling of the aneurysms. After the procedure, the patient remained neurologically well. The patient was monitored appropriately for vasospasm, and was discharged home 10 days after presentation.
Conclusion:Rupture of aneurysms along intracranial branches of the occipital artery can lead to pure subdural hematoma along the tentorium.
Keywords: Aneurysmal rupture, occipital artery, subdural hematoma, transmastoid branches, transosseous branches
INTRODUCTION
Rupture of an intracranial aneurysm predominantly leads to subarachnoid hemorrhage (SAH), with frequent associations with intraparenchymal hematoma (IPH) or intraventricular hemorrhage (IVH).[
CASE PRESENTATION
A 70-year-old female, with a history of hypertension, congestive heart failure, renal artery stenosis, and gout, presented with sudden-onset, excruciating headaches, associated with dizziness, nausea, and emesis. There was no history of trauma. Neurological examination was unremarkable. Computed tomography (CT) of the head demonstrated a tentorial SDH [
DISCUSSION
The presence of an acute SDH in addition to SAH from an aneurysmal rupture is associated with a poor prognosis; in particular, acute SDH is an independent predictor for poor outcomes at discharge and at 3 months.[
Several mechanisms have been proposed to explain SDH development after aneurysmal rupture. For one, adhesions between the aneurysm and the arachnoid membrane could provide a pathway for direct hemorrhage into the subdural space.[
A significant proportion of the patients with pure SDH involving the tentorium exhibited internal carotid artery—posterior communicating artery aneurysms.[
CONCLUSION
The rupture of aneurysms along intracranial branches of the occipital artery can lead to pure subdural hematoma along the tentorium. For nontraumatic acute subdural hematoma, vigilance should be directed toward a vascular etiology.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Alvernia JE, Fraser K, Lanzino G. The occipital artery: A microanatomical study. Neurosurgery. 2006. 58: ONS114-22
2. Biesbroek JM, Rinkel GJ, Algra A, van der Sprenkel JW. Risk factors for acute subdural hematoma from intracranial aneurysm rupture. Neurosurgery. 2012. 71: 264-8
3. Biesbroek JM, van der Sprenkel JW, Algra A, Rinkel GJ. Prognosis of acute subdural haematoma from intracranial aneurysm rupture. J Neurol Neurosurg Psychiatry. 2013. 84: 254-7
4. Kocak A, Ates O, Durak A, Alkan A, Cayli S, Sarac K. Acute subdural hematomas caused by ruptured aneurysms: Experience from a single Turkish center. Turk Neurosurg. 2009. 19: 333-7
5. Kumar S, Sharma R, Goyal S, Husain S. Occipital artery occlusion to facilitate transmastoid posterior fossa tumor embolization. J Neurosci Rural Pract. 2011. 2: 178-9
6. Mansour O, Hassen T, Fathy S. Acute aneurismal bilateral subdural haematoma without subarachnoid haemorrhage: A case report and review of the literature. Case Rep Neurol Med 2014. 2014. p.
7. Marbacher S, Tomasi O, Fandino J. Management of patients presenting with acute subdural hematoma due to ruptured intracranial aneurysm. Int J Vasc Med 2012. 2012. p.
8. Nonaka Y, Kusumoto M, Mori K, Maeda M. Pure acute subdural haematoma without subarachnoid haemorrhage caused by rupture of internal carotid artery aneurysm. Acta Neurochir. 2000. 142: 941-4
9. Shepherd D, Kapurch J, Datar S, Lanzino G, Wijdicks EF. Sphenoid and subdural hemorrhage as a presenting sign of ruptured clinoid aneurysm. Neurocrit Care. 2014. 20: 489-93
10. Song TW, Kim SH, Jung SH, Kim TS, Joo SP. Rupture of distal anterior cerebral artery aneurysm presenting only subdural hemorrhage without subarachnoid hemorrhage: A case report. Springer Plus. 2016. 5: 73-

