

- Iran University of Medical Sciences, Rasool Akram Hospital, Tehran, Iran
- Iran University of Medical Sciences, Tehran, Iran
Correspondence Address:
Morteza Taheri
Iran University of Medical Sciences, Rasool Akram Hospital, Tehran, Iran
DOI:10.4103/sni.sni_20_17
Copyright: © 2017 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Alireza Tabibkhooei, Morteza Taheri, Arash Fattahi, Feyzollah Ebrahimniya, Mohsen Benam. Remote cerebellar hemorrhage: Report of two different cases. 26-Apr-2017;8:54
How to cite this URL: Alireza Tabibkhooei, Morteza Taheri, Arash Fattahi, Feyzollah Ebrahimniya, Mohsen Benam. Remote cerebellar hemorrhage: Report of two different cases. 26-Apr-2017;8:54. Available from: http://surgicalneurologyint.com/surgicalint-articles/remote-cerebellar-hemorrhage-report-of-two-different-cases/
Date of Submission
11-Jan-2017
Date of Acceptance
28-Jan-2017
Date of Web Publication
26-Apr-2017
Abstract
Background:Remote cerebellar hemorrhage (RCH) is a rare complication after supratentorial craniotomies, which usually presents as linear hemorrhages on the surface of the cerebellum; the exact mechanism of it is not established yet.
Case Description:In case one, a 57-year-old patient demonstrated hemorrhage in the cerebellar sulci in favor of RCH 2 days after craniotomy for sphenoidal wing meningioma resection. He was asymptomatic and showed good prognosis after conservative treatment. However, in the second case, a 21-year-old man presented with symptomatic RCH just after the surgery for resection of huge intraaxial parietooccipital lesion. He had a poor prognosis despite the treatment and died ultimately.
Conclusion:Although some studies reported the good prognosis for this type of hemorrhage, it can cause neurological and clinical deterioration and result to patient death.
Keywords: Postoperative complication, remote cerebellar hemorrhage, supratentorial craniotomy
BACKGROUND
Remote cerebellar hemorrhage (RCH) after supratentorial surgery is rare, ranging between 0.08% and 0.6% in the literature, with poorly-understood underlying mechanisms.[
CASE DESCRIPTION
Case 1
A 57-year-old male was presented with headaches, gait problem, and dizziness. Physical examination showed no significant deficits. The brain imaging demonstrated an enhancing extra-axial mass in the left frontal lobe adjacent to the left carotid artery bifurcation in favor of inner third sphenoidal wing meningioma [
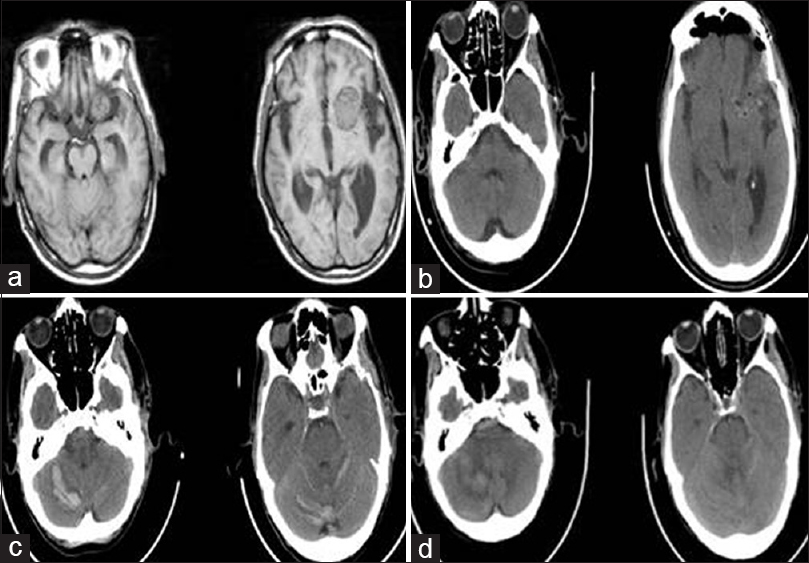
Figure 1
Case one: (a) axial T1weighted magnetic resonance imaging defines anatomic location of the left sphenoidal wing meningioma, (b) early postoperative axial brain CT scan lacks any sign in favor of RCH, (c) late postoperative scan unmask RCH and (d) the scan just before patient discharge depicted resolution of hematoma
Under general anesthesia and in supine position, the patient's head was positioned in a slight extension and rotation to the right while fixed on Mayfield head fixation. Adopting pterional and transsylvian approaches, the sphenoid wing meningioma was resected completely with no significant intraoperative complication. Postoperation, the patient, alert and oriented, was transferred to the neurosurgical intensive care unit (ICU), with no new neurological deficit. Postoperative brain computed tomography (CT) scan showed a moderate volume of pneumocephalus bifrontally, little epidural hematoma, small contusions, and hematoma in the surgical field [
The patient was stable neurologically and hemodynamically, with mean blood pressure between 90 and 110 mmHg. All lab tests, including prothrombin time (PT), partial thromboplastin time (PTT) and international normalized ratio (INR), were normal. Minimal blood was observed in vacuum drainage container. He was transferred to the ward on the second day of the surgery, with no more associated problems. On the third day after surgery, we noticed a large volume of bloody fluid (approximately 300 cc) in vacuum drainage container while the patient had no new complaint or neurologic deficit. Control CT scan showed cerebellar linear hemorrhage (zebra sign) and an intracerebellar hemorrhage of about 35 × 8 mm2 with no mass effect on the fourth ventricle [
The patient was taken back to the ICU for close observation, and coagulation profile (PT, PTT, and INR, bleeding and clotting times) showed no abnormality. The patient remained stable hemodynamically and intact neurologically. Follow-up CT scans showed no changes toward hydrocephalus, and the patient was treated conservatively. Brain magnetic resonance angiography (MRA) and magnetic resonance venography (MRV) showed no significant vascular findings. The hematoma resolved after approximately 10 days and the patient was discharged with satisfactory recovery [
Case 2
A 21-year-old man presented with hearing problem. Physical exam was normal; whereas the brain imaging demonstrated a huge intraaxial mass in the parietooccipital lobe originating from lateral ventricle associated with calcification [Figure
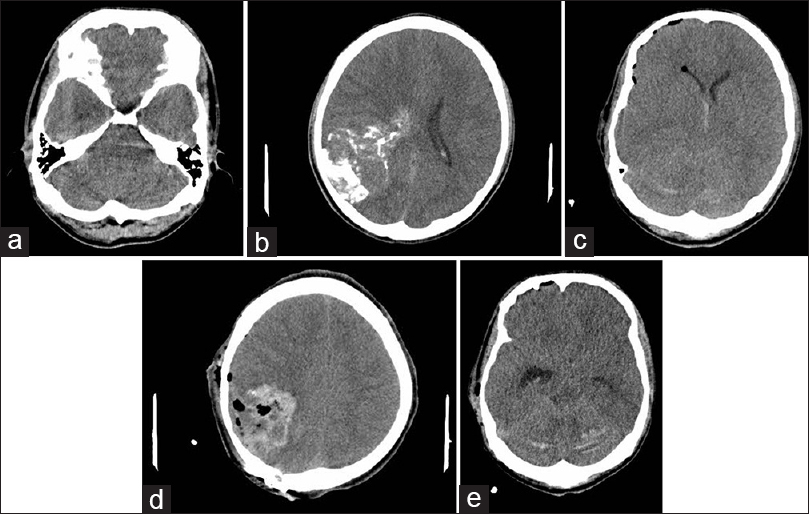
Figure 2
Case two: (a and b) preoperative CTscan demonstrated posterior fossa and supratentorial tumor, (c and d) the first scan postoperation showed linear hemorrhage in posterior fossa in favor of RCH and blood in surgical field and (e) the second scan postoperation demonstrated the exacerbated hemorrhage
The patient underwent craniotomy in the semilateral position. The head was fixed on Mayfield head fixation, and after craniotomy, total resection of tumor was done without any intraoperative complication. Postoperation, the patient was extubated and transmitted to the recovery room and then to neuro ICU. In ICU, generalized tonic–clonic seizure occurred suddenly and progressed to status epileticus. Despite administration antiepileptic agents, as seizure continued, the patient was intubated again after taking anesthesia. The postoperative CT scan showed the hemorrhage in the surgical field and in the cerebellar sulci in favor of RCH [Figure
DISCUSSION
RCH is a rare complication after supratentorial surgeries with an incidence rate between 0.08% and 0.6% in literature and poorly-understood underlying mechanisms,[
It has been reported that RCH is a benign entity with a good prognosis,[
Amini et al. suggested that the most common symptom of RCH is loss of consciousness. Therefore, the patient might show motor deficit, gait ataxia, and prolong anesthesia, or be asymptomatic.[
In our cases, a moderate amount of CSF was lost during the operation while opening the cisterns. Blood pressure, platelets count, and coagulation profiles were normal.
In the first patient, a large amount of CSF drainage from vacuum drain might have played an important role in the occurrence of RCH, while in the second patient, RCH occurred just after the surgery and the vacuum drain cannot be the reason. The first patient was asymptomatic and had a good prognosis, however, the second one was symptomatic and demonstrated deterioration and had a poor prognosis.
CONCLUSION
RCH after supratentorial craniotomy is a very rare complication and can be a life threatening and result to death. It is considered to avoid rapid loss of CSF intraoperative, avoiding excessive vacuum drainage, conservative treatment and serial CT scan.
Financial support and sponsorship
Nil.
Conflicts of interest
The authors declare that they have no conflict of interest, financial or otherwise with any organization.
References
1. Amini A, Osborn AG, McCall TD, Couldwell WT. Remote Cerebellar hemorrhage. AJNR Am J Neuroradiol. 2006. 27: 387-90
2. Brisman MH, Bederson JB, Sen CN, Germano IM, Moore F, Post KD. Intracerebral hemorrhage occurringre mote from the craniotomy site. Neurosurgery. 1996. 39: 1114-21
3. Brockmann MA, Nowak G, Reusche E, Russlies M, Petersen D. Zebra sign: Cerebellar bleeding pattern characteristic of cerebrospinal fluid loss. Case report. J Neurosurg. 2005. 102: 1159-62
4. Honegger J, Zentner J, Spreer J, Carmona H, Schulze-Bonhage A. Cerebellar hemorrhage arising postoperatively as a complication of supratentorial surgery: A retrospective study. J Neurosurg. 2002. 96: 248-54
5. Koller M, Ortler M, Langmayr J, Twerdy K. Posterior-fossa haemorrhage after supratentorial surgery- report of three cases and review of the literature. Acta Neurochir. 1999. 141: 587-92

