

- Department of Neurosurgery, Neurosurgery Teaching Hospital, Baghdad, Iraq,
- Department of Neurosurgery, University of Washington, Seattle, Washington, United States,
- Department of Medical Students, College of Medicine, University of Baghdad, Baghdad, Iraq.
Correspondence Address:
Zahraa F. Al-Sharshahi
Department of Medical Students, College of Medicine, University of Baghdad, Baghdad, Iraq.
DOI:10.25259/SNI_952_2020
Copyright: © 2021 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Samer S. Hoz1, Zaid Aljuboori2, Saja A. Albanaa3, Zahraa F. Al-Sharshahi1, Mohammed A. Alrawi1, Ali M. Neamah3, Aktham O. Al-Khafaji3. Ruptured giant aneurysm of a cortical middle cerebral artery: A case report. 08-Mar-2021;12:95
How to cite this URL: Samer S. Hoz1, Zaid Aljuboori2, Saja A. Albanaa3, Zahraa F. Al-Sharshahi1, Mohammed A. Alrawi1, Ali M. Neamah3, Aktham O. Al-Khafaji3. Ruptured giant aneurysm of a cortical middle cerebral artery: A case report. 08-Mar-2021;12:95. Available from: https://surgicalneurologyint.com/surgicalint-articles/ruptured-giant-aneurysm-of-a-cortical-middle-cerebral-artery-a-case-report/
Date of Submission
28-Dec-2020
Date of Acceptance
14-Feb-2021
Date of Web Publication
08-Mar-2021
Abstract
Background: Aneurysms of the cortical branches of the middle cerebral artery (MCA) are rare. They usually are secondary to traumatic or infectious etiologies and are rarely idiopathic. The specific characteristics of idiopathic aneurysms in such location are not well defined in the literature. The authors report a rare case of a ruptured giant idiopathic cortical MCA aneurysm with review of the available literature on this clinical entity.
Case Description: A 24-year-old female presented with headache, disturbed level of consciousness, and right-sided weakness. Imaging studies showed a left frontoparietal intracerebral hematoma and a giant saccular aneurysm in the posterior parietal cortical branch of the MCA. The patient had no history of head trauma or active infection; therefore, the aneurysm was considered idiopathic. A microsurgical clipping of the aneurysm with evacuation of the hematoma was performed. There were no surgical complications, and the patient achieved a good outcome modified Rankin Scale of 1 with no neurological deficits.
Conclusion: Idiopathic aneurysms of the cortical branches of the MCA are rare, and usually present with intraparenchymal hemorrhage due to rupture. There is no clear consensus regarding the optimal management strategy. This case shows that timely management can lead to good outcomes.
Keywords: Aneurysm, Cortical, Idiopathic, M4, Middle cerebral artery, Peripheral
INTRODUCTION
The middle cerebral artery (MCA) is the third most common site for aneurysm formation, accounting for up to 20% of all intracranial aneurysms.[
CASE DESCRIPTION
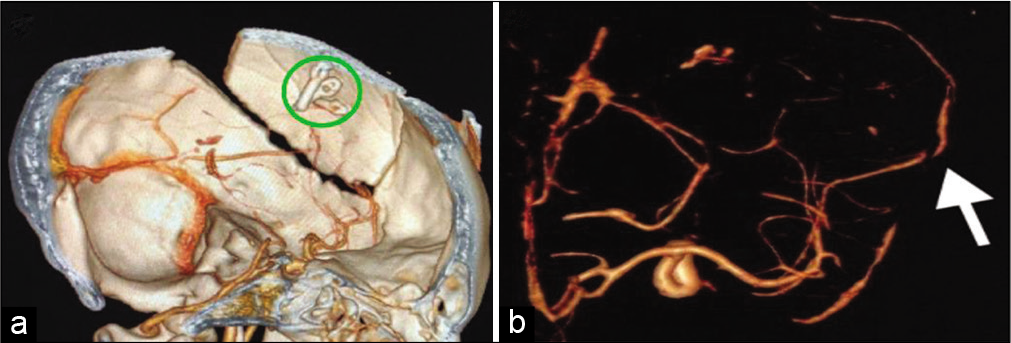
An otherwise healthy 24-year-old female presented with a sudden-onset, severe frontal headache associated with vomiting, disturbed level of consciousness (Glasgow Coma Scale 13), and right-sided weakness. The patient had no history of traumatic head injury, fever, heart disease, or intravenous drug use. A computed tomography (CT) scan of the brain revealed a left-sided frontoparietal intracerebral hematoma (ICH) (<5 mm from the surface) surrounded by edema with a midline shift of more than 5 mm. The CT-angiography (CTA) showed a 26 mm saccular MCA aneurysm of the left posterior parietal cortical branch. No diagnostic catheter angiography was offered as neurointerventional facilities are not available in our country. Echocardiography and routine blood tests ruled out infective endocarditis. A diagnosis of a ruptured idiopathic cortical MCA aneurysm was made. The patient underwent a left parietal craniotomy with microsurgical clipping of the aneurysm and evacuation of the hematoma to relieve the resultant mass effect [
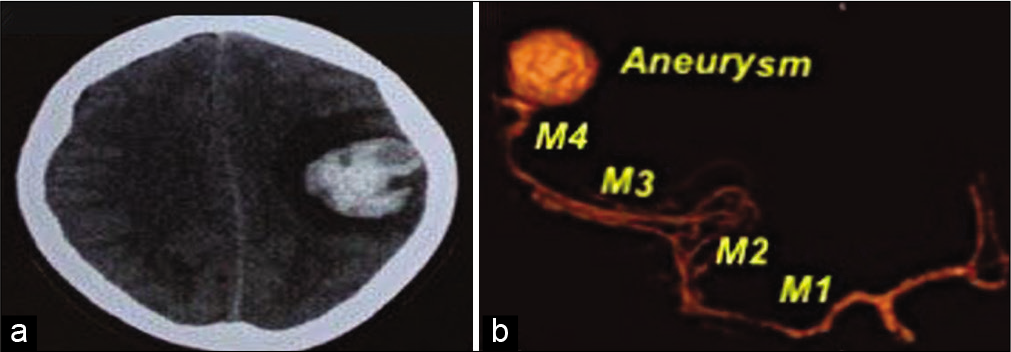
Figure 1:
(a) A non-contrast brain computed tomography (CT) scan (axial view) showing a left fronto-parietal intracerebral hematoma, (b) A preoperative CT-angiography (3D reconstruction) showing a giant cortical middle cerebral artery aneurysm of the posterior parietal cortical branch (M1-M4: Corresponds to the segments of middle cerebral artery).
DISCUSSION
The MCA is anatomically divided into four segments; sphenoidal or horizontal (M1), insular (M2), opercular (M3), and cortical (M4) segments. The cortical segment is further divided into 12 branches.[
Cortical MCA aneurysms can be mycotic, traumatic, inflammatory (vasculitis), or idiopathic.[
Morphologically, idiopathic MCA aneurysms tend to have a regular shape and small size, given the low-flow hemodynamics at the distal cortical segments, as opposed to the irregularly shaped mycotic aneurysms. This distinction is prognostically significant given the higher risk of rupture associated with mycotic aneurysms.[
Treatment strategies available for cortical MCA aneurysms involves both endovascular and microsurgical (clipping, trapping with or without bypass) options with no consensus on the optimal management plan. Important factors to consider include patient’s presentation, parent vessel characteristics and aneurysm size, etiology, morphology, and location.[
Idiopathic cortical MCA aneurysms are rare clinical entities and require a treatment approach that is unique to each patient. Similar to other ruptured aneurysms, they require urgent treatment and tend to have good clinical outcomes (functional independence).
CONCLUSION
Idiopathic cortical MCA aneurysms are rare and usually present without SAH. The sudden onset of the ictus in the absence of trauma should raise the suspicion for a potential cortical aneurysm. Given their cortical location, idiopathic saccular MCA aneurysms may favor surgical clipping with good outcomes.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Abruzzo TA, DiNapoli V, Rahme R, Patel B, O’Brien K, Jimenez L. Intracranial arterial aneurysms in children and young adults. J Pediatr Neuroradiol. 2013. 2: 203-35
2. Aeron G, Abruzzo TA, Jones BV. Clinical and imaging features of intracranial arterial aneurysms in the pediatric population. Radiographics. 2012. 32: 667-81
3. Awaji K, Inokuchi R, Ikeda R, Haisa T. Nontraumatic pure acute subdural hematoma caused by a ruptured cortical middle cerebral artery aneurysm: Case report and literature review. NMC Case Rep J. 2016. 3: 63-6
4. Boop WC, Chou SN, French LA. Ruptured intracranial aneurysm complicated by subdural hematoma. J Neurosurg. 1961. 18: 834-6
5. Cilliers K, Page BJ. Anatomy of the middle cerebral artery: Cortical branches, branching pattern and anomalies. Turk Neurosurg. 2017. 27: 671-81
6. Ducruet AF, Hickman ZL, Zacharia BE, Narula R, Grobelny BT, Gorski J. Intracranial infectious aneurysms: A comprehensive review. Neurosurg Rev. 2010. 33: 37
7. Elsharkawy A, Lehečka M, Niemelä M, Billon-Grand R, Lehto H, Kivisaari R. A new, more accurate classification of middle cerebral artery aneurysms: Computed tomography angiographic study of 1009 consecutive cases with 1309 middle cerebral artery aneurysms. Neurosurgery. 2013. 73: 94-102
8. Fatima N, Al Sulaiti G, Al Rumaihi G. Onyx embolization of distal middle cerebral artery aneurysm in a patient with nontraumatic subdural hematoma. Asian J Neurosurg. 2019. 14: 915
9. Gibo H, Carver CC, Rhoton AL, Lenkey C, Mitchell RJ. Microsurgical anatomy of the middle cerebral artery. J Neurosurg. 1981. 54: 151-69
10. Gong J, Sun H, Shi XY, Liu WX, Shen Z. Pure subdural hematoma caused by rupture of middle cerebral artery aneurysm: Case report and literature review. J Int Med Res. 2014. 42: 870-8
11. Hori E, Ogiichi T, Hayashi N, Kuwayama N, Endo S. Case report: Acute subdural hematoma due to angiographically unvisualized ruptured aneurysm. Surg Neurol. 2005. 64: 144-6
12. Kurabe S, Ozawa T, Fujiwara H, Watanabe T, Aiba T. Peripheral intracranial aneurysm causing subdural hematoma without subarachnoid hemorrhage. Neurology. 2010. 74: 268
13. Lee SM, Park HS, Choi JH, Huh JT. Ruptured mycotic aneurysm of the distal middle cerebral artery manifesting as subacute subdural hematoma. J Cerebrovasc Endovasc Neurosurg. 2013. 15: 235-40
14. Raza SM, Papadimitriou K, Gandhi D, Radvany M, Olivi A, Huang J. Intra-arterial intraoperative computed tomography angiography guided navigation: A new technique for localization of vascular pathology. Neurosurgery. 2012. 71: ons240-52
15. Rengachary SS, Szymanski DC. Subdural hematomas of arterial origin. Neurosurgery. 1981. 8: 166-72
16. Ricci A, Di Vitantonio H, De Paulis D, Del Maestro M, Raysi SD, Murrone D. Cortical aneurysms of the middle cerebral artery: A review of the literature. Surg Neurol Int. 2017. 8: 117
17. Saito H, Ogasawara K, Kubo Y, Saso M, Otawara Y, Ogawa A. Treatment of ruptured spontaneous saccular aneurysm in the central artery of the middle cerebral Artery using bypass surgery combined with trapping. Neurol Med Chir. 2007. 47: 471-4
18. Shekarchizadeh A, Masih S, Reza P, Seif B. Acute subdural hematoma and subarachnoid hemorrhage caused by ruptured cortical artery aneurysm: Case report and review of literature. Adv Biomed Res. 2017. 6: 46
19. Shim YS, Moon CT, Chun YI, Koh YC. Grading of intracerebral hemorrhage in ruptured middle cerebral artery aneurysms. J Korean Neurosurg Soc. 2012. 51: 268
20. Singla N, Tripathi M, Chhabra R. M5 segment aneurysm presenting as. “pure acute SDH”. J Neurosci Rural Pract. 2014. 5: 402-4
21. Sung SK, Kim SH, Son DW, Lee SW. Acute spontaneous subdural hematoma of arterial origin. J Korean Neurosurg Soc. 2012. 51: 91
22. Verhey LH, Wang W, Adel JG. True cortical saccular aneurysm presenting as an acute subdural hematoma. World Neurosurg. 2018. 113: 58-61

