

- Department of Neurosurgery, Loghman e Hakim Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran
Correspondence Address:
Mehrdad Hosseinzadeh Bakhtevari
Department of Neurosurgery, Loghman e Hakim Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran
DOI:10.4103/sni.sni_161_17
Copyright: © 2017 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Keveh Ebrahimzadeh, Mehrdad Hosseinzadeh Bakhtevari, Mohammad Hallajnejad, Omidvar Rezaei. Solitary aneurysm of the filum terminale artery: A case report and review of the literature. 09-Aug-2017;8:179
How to cite this URL: Keveh Ebrahimzadeh, Mehrdad Hosseinzadeh Bakhtevari, Mohammad Hallajnejad, Omidvar Rezaei. Solitary aneurysm of the filum terminale artery: A case report and review of the literature. 09-Aug-2017;8:179. Available from: http://surgicalneurologyint.com/surgicalint-articles/solitary-aneurysm-of-the-filum-terminale-artery-a-case-report-and-review-of-the-literature/
Date of Submission
27-Apr-2017
Date of Acceptance
05-Jun-2017
Date of Web Publication
09-Aug-2017
Abstract
Background:We report a rare case of aneurysmal dilatation of filum terminale artery after resection of filum terminal myxopapillary ependymoma.
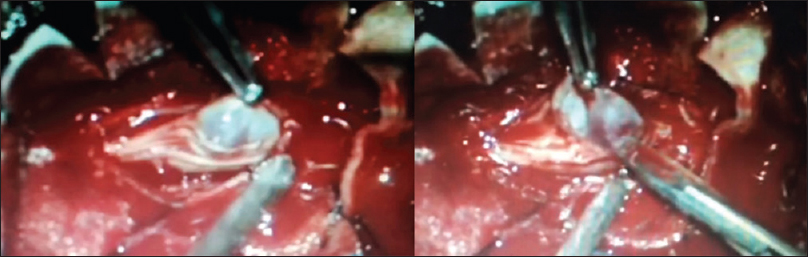
Case Description:The authors report a rare aneurysmal dilatation of the filum terminale artery following removal of a filum terminal myxopapillary ependymoma in a 10-year-old male. The patient presented with 6-month history of increasing back pain without a focal neurological deficit. Magnetic resonance (MR) showed an intradural filum terminale lesion that was completely excised. Three months later, the MR again revealed a lesion involving the filum terminale. During the second surgery, however, an aneurysmal dilation of the filum artery was found, which was coagulated and resected. Following the secondary surgery, the patient's symptoms gradually resolved, and he remains intact.
Conclusion:Although rare, a true aneurysm after spinal surgery should be considered among the differential diagnostic consideration in the region of the filum terminale.
Keywords: Aneurysm, filum terminale, myxopapillary ependymoma, spinal cord
INTRODUCTION
Aneurysms of spinal arteries arise from arteries inside the dural sac. They most typically involve the proximal intradural radiculomedullary or radiculopial arteries, and only rarely, the anterior or posterior spinal arteries. They are usually fusiform but may also be saccular in configuration. According to the literature review, aneurysm of the filum terminale artery is very rare, and this is the first report of an isolated filum terminale artery aneurysm after spinal myxopapillary ependymoma tumor.
CASE REPORT
A 10-year-old male, with a history of progressive low back pain for 6 months, underwent magnetic resonance imaging (MRI) of the lumbar spine showing an intradural mass filling the spinal canal from L2 to L5. The lesion was isointense on T1-weighted and hyperintense on T2-weighted images; it also markedly enhanced after gadolinium injection [

However, 3 months later, the follow-up MR revealed an intradural mass at the L3 level newly accompanied by a signal void [

DISCUSSION
Literature review
According to the literature review, aneurysm of the filum terminale artery is very rare, and this is the first report of an isolated filum terminale artery aneurysm after spinal myxopapillary ependymoma tumor [

This report focuses on the unique presentation of aneurysms involving the filum terminale artery following resection of a myxopapillary ependymoma.
The artery of the filum arises from the termination of the anterior spinal axis, either by trifurcation or from the proximal part of one of the two branches of the anastomotic ansa of the conus. At the level of the conus, the anterior spinal artery anastomoses with posterior spinal arteries. The artery travels in front of the filum and exhibits a rapidly diminishing caliber; rarely, it can be followed into the sacral canal.
Aneurysms are caused by a weakened blood vessel wall and can be an outcome of a hereditary condition or an acquired disease. Aneurysms can make a clot formation (thrombosis) and embolization.[
Spinal cord aneurysms usually have a dissecting etiology—the vessel is torn at the point where it traverses the dura, and the dissection propagates into the intradural (subarachnoid) segment of the vessel. Subarachnoid hemorrhage occurs when the dissection ruptures. However, if the dissection thrombosis, the outcome will depend on the availability of collateral support. When a dominant radiculomedullary artery (for example, Adamkiewicz) is occluded with no effective collaterals, symptoms of the anterior spinal cord infarct ensue (acute paraplegia, bowel, bladder, sexual dysfunction, pain and temperature sensory loss, sparing proprioception, and vibration). However, if effective radiculomedullary collaterals exist, the patient will likely do well.[
Another high yield etiology of these aneurysms are inherited connective tissue disorders and acquired vascular lesions (due to infections or inflammatory vasculopathies) which compromise the strength of the arterial wall, ultimately leading to aneurysm formation in the absence of a primary pathologic alteration of local hemodynamics.[
Spinal artery aneurysms are rare and uncommon lesions and they occur with spinal arteriovenous malformation in 20% of cases. Regarding spinal aneurysms, those patients who did bleed, approximately half had a recurrent episode, usually within 1 year.[
Anterior spinal artery aneurysms are rare and the result of hemodynamic anomalies; they are often associated with high flow vascular lesions. These may occur at all segments of the spinal artery, except at the bifurcation, and are often fusiform in morphology. Most are microaneurysms (smaller than 3 mm in diameter) and patients typically present with subarachnoid hemorrhage and/or signs of spinal cord compression.[
Spinal aneurysms differ from intracranial aneurysms in ways that affect their management. They seldom occur at branching points; rather, they develop along the course of an artery. The caliber of the spinal arteries is much smaller than that of intracranial arteries and they tend to be less affected by atherosclerosis.[
CONCLUSION
This case presents the rare finding of aneurysms of the filum terminale artery following resection of a myxopapillary ependymoma in a 10-year-old male. An aneurysm should be considered among the differential diagnostic considerations following tumor removal in this location. These lesions may spontaneously rupture definitive diagnosis and treatment (e.g., coagulation and resection) should be performed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Berenstein A, Lasjaunias PL, Brugge KG.editorsSurgical Neuroangiography. Springer; 2001. p.
2. Berlis A, Scheufler KM, Schmahl C, Rauer S, Götz F, Schumacher M. Solitary spinal artery aneurysms as a rare source of spinal subarachnoid hemorrhage: Potential etiology and treatment strategy. Am J Neuroradiol. 2005. 26: 405-10
3. Ceciliano A, Garbugino S, Sierre SD, Moguillansky S, Routabul C, Monges J. Endovascular Treatment with Platinum Microcoils of an Anterior Spinal Artery Aneurysm Associated with a Spinal Arteriovenous Malformation. ASNR Annual Meeting Abstracts. 2003. p.
4. Cronenwett JL, Murphy TF, Zelenock GB, Whitehouse WM, Lindenauer SM, Graham LM. Actuarial analysis of variables associated with rupture of small abdominal aortic aneurysms. Surgery. 1985. 98: 472-83
5. Greenberg M.editors. SAH and aneurysms. Handbook of neurosurgery. New York: Thieme Medical; 2000. p. 803-
6. Osman K, Orhan O, Yahya P, Yalcın K. Anterior spinal artery aneurysm presenting with spinal cord compression: MRI and MRI angiographic findings. J Neurol Neurosurg Psychiatry. 2010. 81: 771-2
7. Sakamoto M, Watanabe T, Okamoto H. A case of ruptured aneurysm associated with spinal arteriovenous malformation presenting with hematomyelia: Case report. Surg Neurol. 2002. 57: 438e42-
8. Spetzler RF, Detwiler PW, Riina HA, Porter RW. Modified classification of spinal cord vascular lesions. J Neurosurg. 2002. 96: S145-56

