

- Department of Pathology and Laboratory Medicine, American University of Beirut Medical Center, Beirut, Lebanon.
- Department of Hematology and Oncology, American University of Beirut Medical Center, Beirut, Lebanon.
- Department of Neurosurgery, American University of Beirut Medical Center, Beirut, Lebanon.
- Department of Radiology, American University of Beirut Medical Center, Beirut, Lebanon.
Correspondence Address:
Sara Sinno, Department of Pathology and Laboratory Medicine, American University of Beirut Medical Center, Beirut, Lebanon.
DOI:10.25259/SNI_902_2022
Copyright: © 2022 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Lama Farhat1, Mohammad Hassan Hodroj2, Sarah Kawtharani3, Charbel Moussalem3, Tamara El Annan4, Hazem Assi2, Houssein Darwish3, Sara Sinno1. Spinal intradural extramedullary granular cell tumor. 28-Oct-2022;13:496
How to cite this URL: Lama Farhat1, Mohammad Hassan Hodroj2, Sarah Kawtharani3, Charbel Moussalem3, Tamara El Annan4, Hazem Assi2, Houssein Darwish3, Sara Sinno1. Spinal intradural extramedullary granular cell tumor. 28-Oct-2022;13:496. Available from: https://surgicalneurologyint.com/surgicalint-articles/11958/
Date of Submission
29-Sep-2022
Date of Acceptance
09-Oct-2022
Date of Web Publication
28-Oct-2022
Abstract
Background: Granular cell tumors (GCTs) are uncommon peripheral nerve sheath tumors of Schwann cell origin that may occur throughout the body. However, they rarely occur in the spinal canal.
Case Description: A 49-year-old male presented with burning sensation in the left knee. The MRI of the lumbar spine showed an L3-L4 intradural extramedullary tumor. Complete surgical resection was successfully performed and the L3 root burning improved. Histopathologically, the lesion proved to be a benign GCT.
Conclusion: Spinal GCTs are rare benign tumors that may be found in an intradural extramedullary location in the spine. The preferred treatment is complete surgical resection as subtotal/partial resection may result in recurrence warranting radiation therapy.
Keywords: Granular cell tumor, Intradural extramedullary, Intramedullary, Nerve sheath tumor, Spinal canal
INTRODUCTION
Granular cell tumors (GCTs) are uncommon soft-tissue tumors that were initially described as granular cell myoblastoma by Abrinkossoff in 1926.[
CASE DESCRIPTION
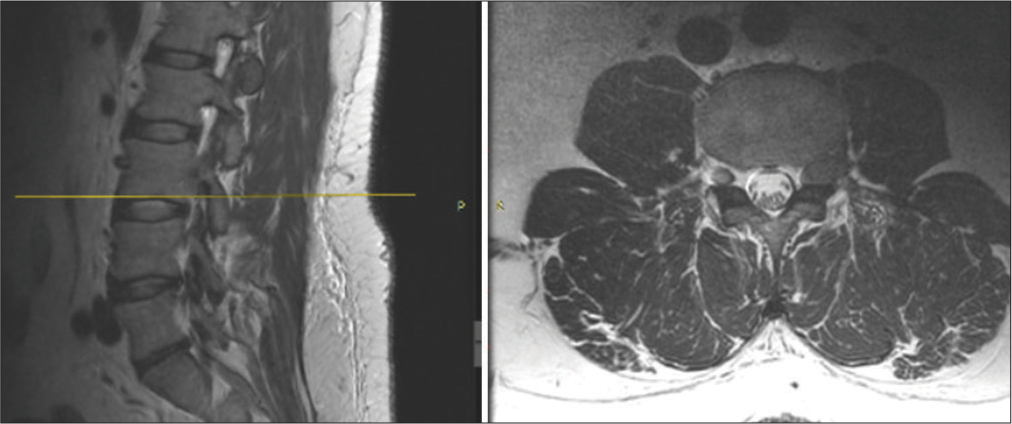
A 49-year-old male presented with burning sensation and pain in the left knee for 2 years’ duration. The pain was severe and refractory to pain medications. The lumbar MRI showed a well-circumscribed soft-tissue lesion in the left L3-L4 neural foramen along the course of the left L3 nerve root. It was isointense to hypointense on T1W, hypointense on T2W images [
Surgery
Under fluoroscopic guidance, a bilateral L3-L4 laminectomy was performed. The pedicles of L3 and L4 were exposed along with the transverse processes. The traversing L3 nerve root was identified and the tumor was completely dissected and resected off the root. Postoperatively, the patient sustained improvement in the burning sensation and exhibited no new motor deficit.
Histology
The histological examination was consistent with a benign GCT. It revealed polygonal tumor cells with abundant, eosinophilic, and granular cytoplasm arranged in sheets [

Figure 2:
Spinal granular cell tumor. (a) The tumor is composed of sheets of polygonal tumor cells with abundant eosinophilic granular cytoplasm (Hematoxylin and Eosin, original magnification ×20). (b-d) The tumor cells are diffusely positive for S-100, SOX-10, and inhibin (original magnification ×20).
DISCUSSION
GCTs are peripheral nerve sheath tumors that show neuroectodermal differentiation.[

The majority of the reported cases of spinal GCTs have an intradural extramedullary location. The differential diagnosis for tumors in this location includes neurofibroma, schwannoma, meningioma, paraganglioma, epidermoid cyst, intradural dissemination, and, in the cauda equina region, myxopapillary ependymoma. Those tumors can be difficult to distinguish from GCTs on MRI.[
Three spinal GCTs were described as being intramedullary.[
The vast majority of GCTs behave in a benign fashion; however, they may recur if incompletely excised.[
CONCLUSION
GCTs are peripheral nerve sheath tumors that rarely occur in the spinal canal where they are usually intradural/ extramedullary in location. The optimal treatment is gross total surgical excision, as subtotal/partial removal may result in recurrence and the need for adjuvant radiation therapy.
Declaration of patient consent
Patient’s consent not required as patient’s identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Al-Karawi SVassilyadi MMichaud J. Brain Pathology Case of the Month-June 2016. Available from: https://path.upmc.edu/divisions/neuropath/bpath/cases/case334.html.
2. Bhati AS, Tyagi A, Tyagi SK. Recurrent granular cell tumor: A case report and review of literature. J Spine Surg. 2017. 3: 484-8
3. Brown KG, Rao PJ, Oo TH, Fowler A. Granular cell tumors of the spinal canal: Intramedullary case report and a review of the literature. J Spine Surg. 2015. 1: 94-8
4. Burton BJ, Kumar VG, Bradford R. Granular cell tumour of the spinal cord in a patient with Rubenstein-taybi syndrome. Br J Neurosurg. 1997. 11: 257-9
5. Critchley GR, Wallis NT, Cowie RA. Granular cell tumour of the spinal cord: Case report. Br J Neurosurg. 1997. 11: 452-4
6. Lee CH, Hyun SJ, Lee JW, Rhim SC. Granular cell tumor of the intradural extramedullary spinal cord: Report of two cases with respect to radiological differential diagnosis. J Korean Neurosurg Soc. 2013. 53: 121-4
7. Li P, Yang Z, Wang Z, Zhou Q, Li S, Wang X. Granular cell tumors in the central nervous system: A report on eight cases and a literature review. Br J Neurosurg. 2016. 30: 611-8
8. Markesbery WR, Duffy PE, Cowen D. Granular cell tumors of the central nervous system. J Neuropathol Exp Neurol. 1973. 32: 92-109
9. Mundi I, Pathak A, Banerjee AK, Brar R. Granular cell tumor at an unusual site masquerading as a neurofibroma. Neurol India. 2017. 65: 1159-61
10. Qu J, Ma J, Luo L, Ai L, Li S, Dai J. Subdural granular cell tumor in thoracic vertebral canal. Neurol India. 2009. 57: 679-81
11. Shen J, Wang S, Shao X, Xu Z, Dai Y, Xu S. Intraspinal granular cell tumor: A case report and review of literature. Int J Clin Exp Pathol. 2016. 9: 4013-20
12. Soldozy S, Syed HR, Jha RT, O’Connell K, Ozdemirli M, Voyadzis JM. Giant granular cell tumor of the cervical spinal cord resected via anterior corpectomy with reconstruction: Technical note and review of literature. World Neurosurg. 2020. 139: 136-41
13. Soni A, Bansal N. Rare intradural extramedullary spinal granular cell tumor in a young female. MOJ Womens Health. 2018. 7: 104-7
14. Stromblad LG, Brun A, Cameron R, Cronquist S. Spinal granular cell tumor with subarachnoid hemorrhage: Case report. Neurosurgery. 1987. 21: 230-3
15. Takayama Y, Hasuo K, Takahashi N, Nishimiya M, Nonoshita T, Takita Y. Granular cell tumor presenting as an intradural extramedullary tumor. Clin Imaging. 2004. 28: 271-3
16. Vaghasiya VL, Nasit JG, Parikh PA, Trivedi PP. Intradural spinal granular cell tumor. Asian J Neurosurg. 2014. 9: 96-8
17. Weinstein BJ, Arora T, Thompson LD. Intradural, extramedullary spinal cord granular cell tumor: A case report and clinicopathologic review of the literature. Neuropathology. 2010. 30: 621-6
18. World Health Organizati, editors. WHO Classification of Tumours Editorial Board. Soft Tissue and Bone Tumours Lyon (France): International Agency for Research on Cancer. WHO Classification of Tumours Series. Geneva: World Health Organization; 2021. 3: Available from: https://tumourclassification.iarc.who.int/chapters/33 [Last accessed on 2022 Sep 29]
19. Xue J, Chen H, Yang Y, Hu J, Yang G. Granular cell tumors in the human spinal canal: A case report and literature review. Int J Clin Exp Med. 2019. 12: 4409-13

