

- Department of Neurosurgery, 7tir Hospital, Iran University of Medical Sciences, Tehran, Iran
- Department of Neurosurgery, Rasool-e-Akram Hospital, Iran University of Medical Sciences, Tehran, Iran
Correspondence Address:
Arash Fattahi
Department of Neurosurgery, Rasool-e-Akram Hospital, Iran University of Medical Sciences, Tehran, Iran
DOI:10.4103/sni.sni_223_17
Copyright: © 2017 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Arash Fattahi, Morteza Taheri. Spontaneous resolved cervical spine epidural hematoma: A case report. 10-Aug-2017;8:183
How to cite this URL: Arash Fattahi, Morteza Taheri. Spontaneous resolved cervical spine epidural hematoma: A case report. 10-Aug-2017;8:183. Available from: http://surgicalneurologyint.com/surgicalint-articles/spontaneous-resolved-cervical-spine-epidural-hematoma-a-case-report/
Date of Submission
20-Jun-2017
Date of Acceptance
29-Jun-2017
Date of Web Publication
10-Aug-2017
Abstract
Background:Cervical spine epidural hematomas (CSEH) are rare, and surgical intervention is typically required. Here, we present the rare case of a CSEH resulting from chiropractic manipulation successfully treated conservatively.
Case Description:A 44-year-old female with cervical myelopathy presented with a mild quadriparesis following manipulation by a chiropractor. Although magnetic resonance (MR) documented a CSEH, the lesion was treated nonsurgically as the patient refused operative intervention. Four days later, the patient demonstrated spontaneous improvement. Furthermore, the 1-month post manipulation cervical MR showed resolution of the CSEH mass effect, and her myelopathy fully resolved.
Conclusion:Few studies document the efficacy of conservative treatment of CSEH. In this case, a patient with cervical myelopathy presented with a mild quadriparesis following chiropractic manipulation. Although MR documented a CSEH, she refused surgery, but fortunately improved neurologically within the next 4 days and was intact within 1 postoperative month. We recommend performing more powerful studies with large sample size to better define criteria for conservative vs. surgical treatment of CSEH.
Keywords: Cervical cord, paresis, spinal epidural hematoma, spinal manipulation
INTRODUCTION
Cervical spine epidural hematomas (CSEH) are rare and have an unknown etiology in most cases.[
CASE DESCRIPTION
We present the case of a 44-year-old female who presented with severe neck pain and mild quadriparesis following a coarse neck massage by an untrained person. On admission, she exhibited low-grade fever (oral 37.5°C) and severe cervical paraspinal muscle spasm accompanied by 4/5 quadriparesis (based on muscle strength grading 0–5), left upper limb hyperreflexia, and a left positive Hoffmann's sign.
Diagnostic studies
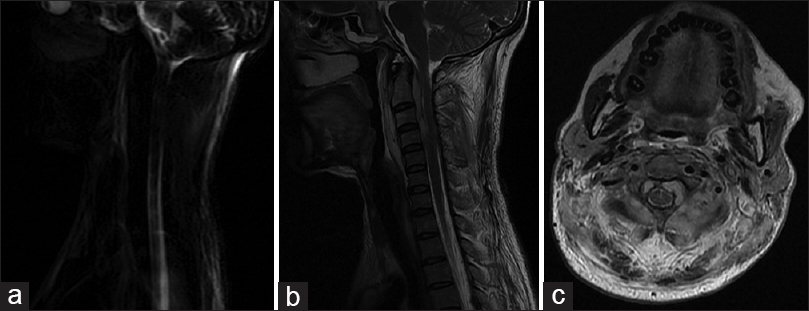
X-ray of the spine showed prevertebral soft tissue swelling that was confirmed on the cervical spine (C/S) MR imaging [

Refusal of surgical management
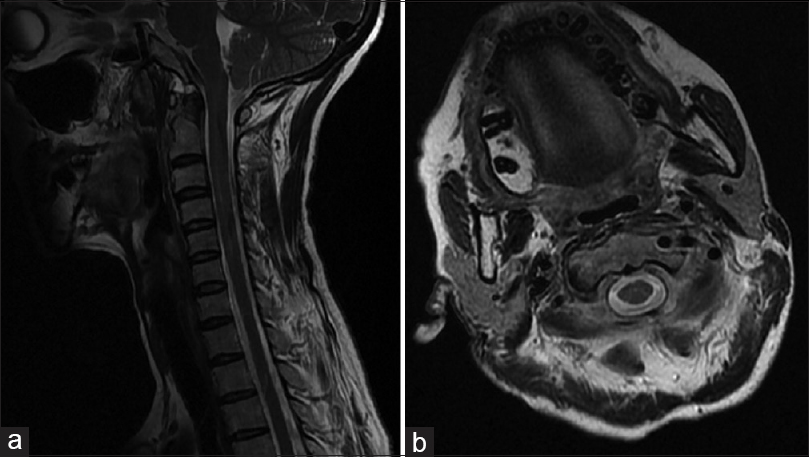
Based on the MR imaging, surgical removal of the CSEH was recommended. She opted for conservative treatment that included the care of an infectious disease specialist looking for the etiology of a fever with unknown origin (FUO). Four days later, her neurological examination improved, she was able to walk, but her “illness” continued. The follow-up C/S MRI confirmed significant relief of the CSEH lesion's mass effect [
DISCUSSION
CSEH are rare and typically warrant surgical intervention. They may be attributed to trauma, congenital spinal vascular anomaly, and/or bleeding disorders. In rare cases, neck manipulation including chiropractic treatment can lead to acute CSEH.[
Location and etiology of spinal epidural hematomas
Most spinal epidural hematomas are found in the cervicothoracic or thoracolumbar regions; they rarely involve the cervical spine.[
Surgical vs. nonsurgical treatment of CSEH
Most surgeons would perform a laminectomy to treat a CSEH. Almost all studies recommend immediate decompressive surgery and some even advocate surgery (laminectomy or laminoplasty) during the first 48 hours for patients with an incomplete cord injury.[
The use of conservative treatment for CSEH is controversial. In some patients with myelopathy and progressive deterioration, surgical management is often chosen as it is associated with less risk/better outcomes. Here, we highlighted lack of adequate criteria for choosing nonsurgical management of CSEH with accompanying myelopathic deficits, especially if acute in onset.
CONCLUSION
We present a patient who developed acute myelopathy and a mild quadriparesis after chiropractic cervical manipulation. MR documented a CSEH that was successfully managed without surgery – this was largely due to the patient's refusal of acute operative intervention. There are few such cases in the literature as most would choose a surgical option to maximize recovery/outcome. We recommend performing more powerful studies with large sample sizes to better define criteria for selecting conservative vs. surgical treatment of CSEH.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Aoki Y, Yamagata M, Shimizu K, Ikeda Y, Nakajima F, Ohtori S. An unusually rapid spontaneous recovery in a patient with spinal epidural hematoma. J Emerg Med. 2012. 43: e75-9
2. Duffill J, Sparrow OC, Millar J, Barker CS. Can spontaneous spinal epidural haematoma be managed safely without operation? A report of four cases. J Neurol Neurosurg Psychiatry. 2000. 69: 816-9
3. Guzel A, Simsek O, Karasalihoglu S, Kucukugurluoglu Y, Acunas B, Tosun A. Spontaneous spinal epidural hematoma after seizure: A case report. Clin Pediatr (Phila). 2007. 46: 263-5
4. Huang M, Barber SM, Moisi M, Powell S, Rivera A, Zwillman M. Cervical Epidural Hematoma after Chiropractic Spinal Manipulation Therapy in a Patient with an Undiagnosed Cervical Spinal Arteriovenous Malformation. Cureus. 2015. 7: e307-
5. Jusue-Torres I, Ortega-Zufiria JM, Tamarit-Degenhardt M, Navarro Torres R, Lopez-Serrano R, Rique-Dormido J. Iatrogenic cervical epidural hematoma: Case report and review of the literature. Neurocirugia (Astur). 2011. 22: 332-6
6. Kreppel D, Antoniadis G, Seeling W. Spinal hematoma: A literature survey with meta-analysis of 613 patients. Neurosurg Rev. 2003. 26: 1-49
7. Lee DY, Lee SH. Cervicothoracic spinal epidural hematoma after anterior cervical spinal surgery. J Korean Neurosurg Soc. 2010. 48: 541-3
8. Marinella MA, Barsan WG. Spontaneously resolving cervical epidural hematoma presenting with hemiparesis. Ann Emerg Med. 1996. 27: 514-7

