

- Department of Neurosurgery, The Jikei University Katsushika Medical Center, Tokyo, Japan.
- Department of Neurosurgery, The Jikei University School of Medicine, Tokyo, Japan.
Correspondence Address:
Jun Takei, Department of Neurosurgery, The Jikei University Katsushika Medical Center, Tokyo, Japan.
DOI:10.25259/SNI_247_2023
Copyright: © 2023 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Ryoto Wachi1, Jun Takei1, Shusuke Fujita1, Ken Aoki1, Hiroyasu Nagashima1, Yuichi Murayama2. Spontaneous shrinkage of vestibular schwannoma with the recovery of impaired hearing: A case report and literature review. 26-May-2023;14:180
How to cite this URL: Ryoto Wachi1, Jun Takei1, Shusuke Fujita1, Ken Aoki1, Hiroyasu Nagashima1, Yuichi Murayama2. Spontaneous shrinkage of vestibular schwannoma with the recovery of impaired hearing: A case report and literature review. 26-May-2023;14:180. Available from: https://surgicalneurologyint.com/surgicalint-articles/12339/
Date of Submission
20-Mar-2023
Date of Acceptance
01-May-2023
Date of Web Publication
26-May-2023
Abstract
Background: Sporadically occurring vestibular schwannomas (VSs) are the most frequent tumors in the cerebellopontine cistern and internal meatus and are commonly associated with hearing loss. These tumors have demonstrated spontaneous shrinkage rates of 0–22%; however, the relationship between tumor shrinkage and changes in hearing remains unclear.
Case Description: We report a case of a 51-year-old woman with a diagnosis of a left-sided VS and accompanying moderate hearing loss. The patient was treated with a conservative approach for 3 years, and the tumor showed a regression along with an improvement in her hearing ability during the yearly follow-ups.
Conclusion: The spontaneous shrinkage of a VS along with an associated improvement in hearing is a rare phenomenon. Our case study may support that the “wait and scan” approach is an alternative option for patients with VS and moderate hearing loss. Further investigations are needed to understand spontaneous VS regression and hearing changes.
Keywords: Hearing improvement, Hearing loss, Intrameatal tumors, Spontaneous shrinkage, Vestibular schwannoma
INTRODUCTION
Sporadic vestibular schwannomas (VSs) are the most frequently found tumors in the cerebellopontine angle and internal meatus and are widely recognized to cause hearing loss along with their growth. Based on their location, these tumors can be classified into the following two types: Intra-meatus and extra-meatus VSs. According to a study by Reznitsky et al., a comparatively larger proportion of VSs is extrameatal VSs.[
Two meta-analysis studies estimated that VSs have a natural growth rate of 1.2–1.9 mm/year.[
CASE DESCRIPTION
A 51-year-old Asian woman who had a medical history of repeated dizziness presented with acute left facial palsy and left facial numbness. Brain magnetic resonance imaging (MRI) showed no evidence of brain stroke, and the patient underwent conservative treatment.
At 1 year after the onset of her previous symptoms, the patient was referred to our hospital for reported left-sided hearing impairment. Pure tone audiogram (PTA) showed moderate hearing impairment on the left side, with 50 dB in the low frequency 3 PTA. Re-evaluation of her brain MRI conducted in the previous year revealed a lesion in the left internal meatus with a maximum intracranial diameter (ICD) of 13.5 mm [
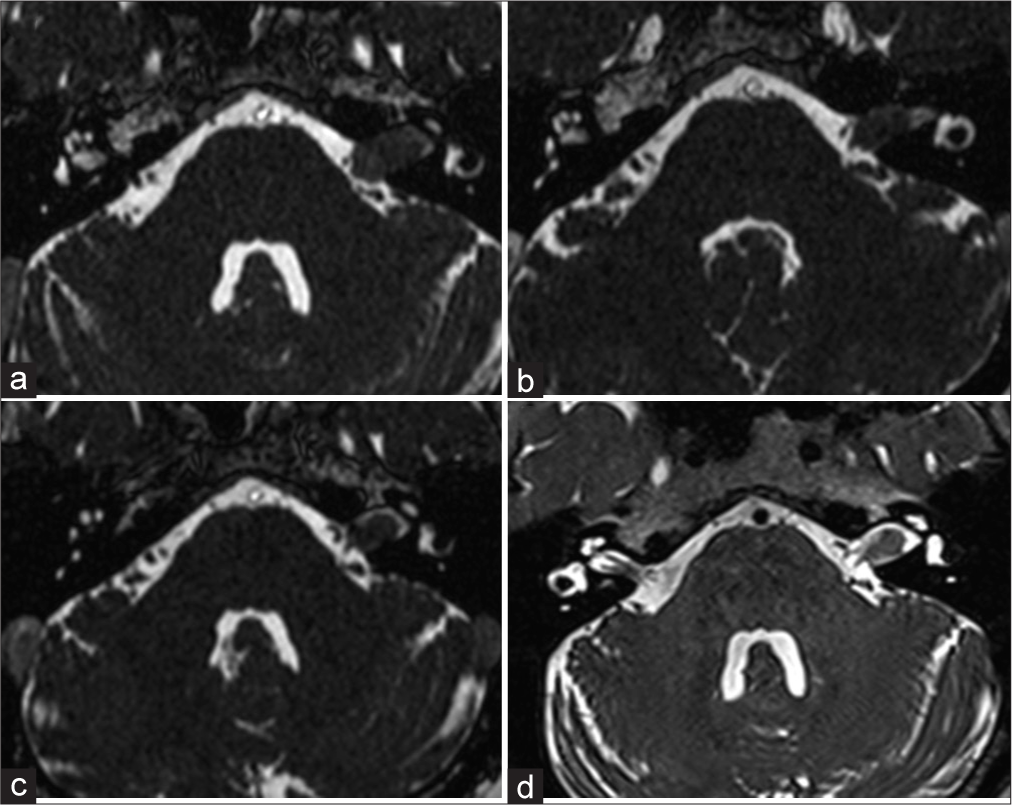
Figure 1:
T2-weighted images showing gradual tumor shrinkage. (a) The solid and nodular tumor on the left cerebellopontine angle cistern expanded the internal auditory canal. (b) Tumor shrinkage was seen at 1-year follow-up. (c) Peritumoral cerebrospinal fluid was observed at 2-year follow-up. (d) The solid tumor involuted at 3-year follow-up.
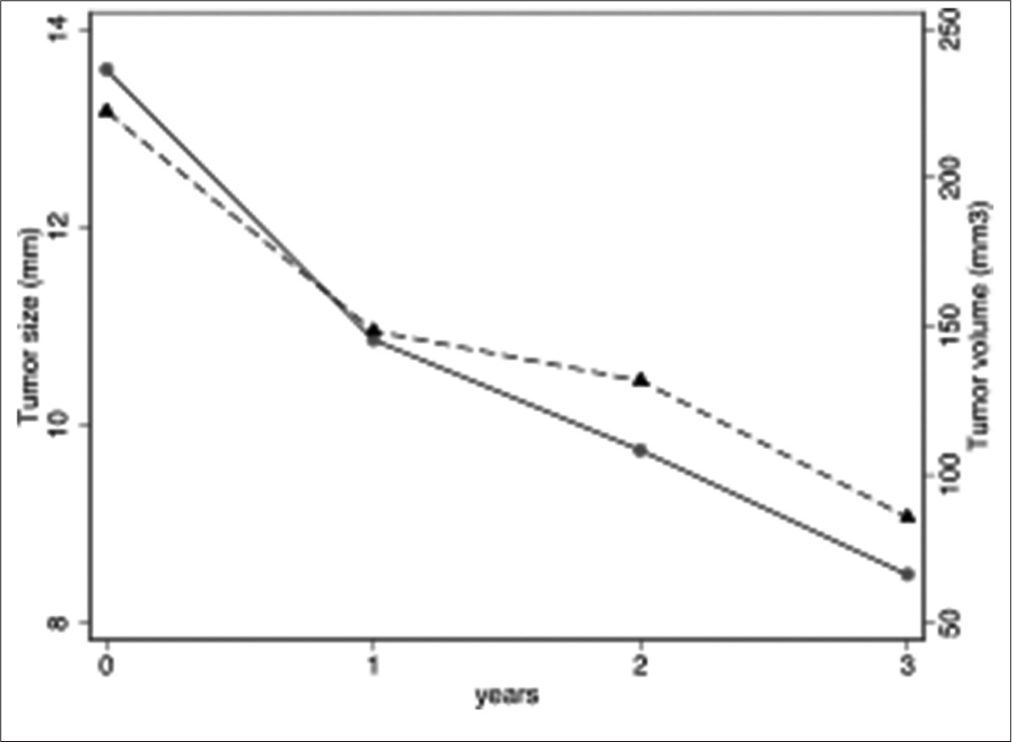
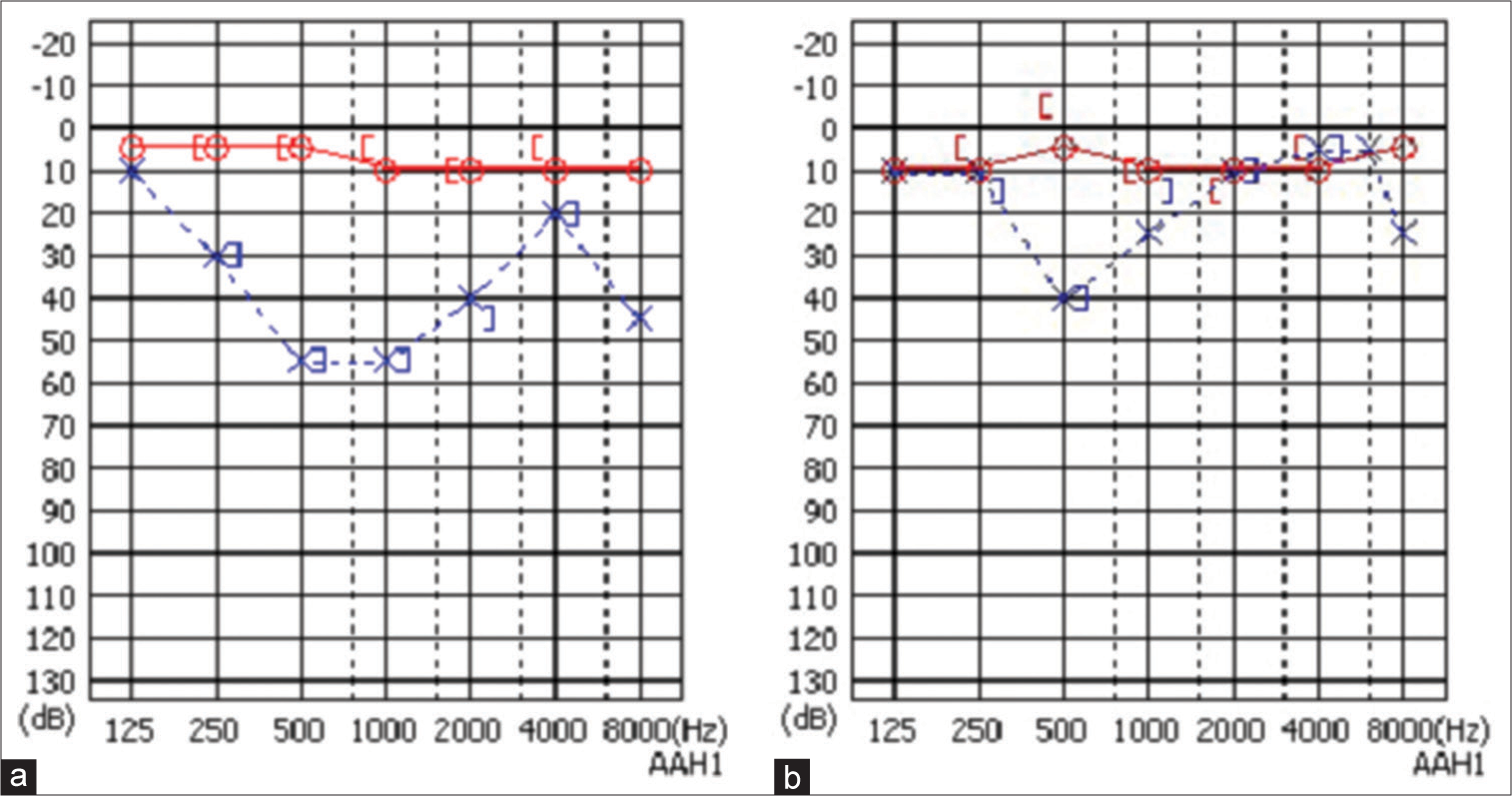
Figure 3:
Audiogram showing an improvement in hearing loss. (a) A pure tone audiogram showed moderate hearing loss on the left side. (b) The left-sided hearing impairment was improved at 2-year follow-up. The red line shows the result for the right ear and the blue line shows the result for the left ear.
DISCUSSION
The natural regression of VSs was first reported in a case series by Laasonen and Troupp. in 1986[
Here, we present a case of a patient with a spontaneously regressed VS with concomitant improvement in hearing. During the 3-year follow-up, the tumor demonstrated a maximum diameter reduction of 5 mm and volume reduction of 63%. PTA revealed an improvement from 50 dB to 25 dB. Based on our literature review, only two reported cases of naturally regressed VS with improvement in hearing have been published.[
Our case study may support the wait and scan strategy. The European Association for Neuro-Oncology guidelines for the treatment of VS recommends the wait and scan or stereotactic radiosurgery (SRS) approach for cases with moderate hearing loss.[
CONCLUSION
In this study, we present a case of a patient with a spontaneously regressed VS with concomitant improvement in hearing. Our study may indicate that the wait and scan approach is an alternative strategy for patients with VS accompanied with moderate hearing loss. Further investigations are required to understand spontaneous VS shrinkage and hearing changes.
Ethical statement
This study was conducted according to the principles of the Declaration of Helsinki. Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Journal or its management. The information contained in this article should not be considered to be medical advice; patients should consult their own physicians for advice as to their specific medical needs.
References
1. Battaglia A, Mastrodimos B, Cueva R. Comparison of growth patterns of acoustic neuromas with and without radiosurgery. Otol Neurotol. 2006. 27: 705-12
2. Ferri GG, Modugno GC, Pirodda A, Fioravanti A, Calbucci F, Ceroni AR. Conservative management of vestibular schwannomas: An effective strategy. Laryngoscope. 2008. 118: 951-7
3. Goldbrunner R, Weller M, Regis J, Lund-Johansen M, Stavrinou P, Reuss D. EANO guideline on the diagnosis and treatment of vestibular schwannoma. Neuro Oncol. 2020. 22: 31-45
4. Gurewitz J, Schnurman Z, Nakamura A, Navarro RE, Patel DN, McMenomey SO. Hearing loss and volumetric growth rate in untreated vestibular schwannoma. J Neurosurg. 2022. 136: 768-75
5. Hajioff D, Raut VV, Walsh RM, Bath AP, Bance ML, Guha A. Conservative management of vestibular schwannomas: Third review of a 10-year prospective study. Clin Otolaryngol. 2008. 33: 255-9
6. Huang X, Caye-Thomasen P, Stangerup SE. Distinct spontaneous shrinkage of a sporadic vestibular schwannoma. Auris Nasus Larynx. 2013. 40: 243-6
7. Laasonen EM, Troupp H. Volume growth rate of acoustic neurinomas. Neuroradiology. 1986. 28: 203-7
8. Lahlou G, Rodallec M, Nguyen Y, Sterkers O, Kalamarides M. How to radiologically identify a spontaneous regression of sporadic vestibular schwannoma?. PLoS One. 2019. 14: e0217752
9. Luetje CM, Whittaker CK, Davidson KC, Vergara GG. Spontaneous acoustic tumor involution: A case report. Otolaryngol Head Neck Surg. 1988. 98: 95-7
10. Marinelli JP, Killeen DE, Schnurman Z, Nassiri AM, Hunter JB, Lees KA. Spontaneous volumetric tumor regression during wait-and-scan management of 952 sporadic vestibular schwannomas. Otol Neurotol. 2022. 43: e1034-8
11. Oliveira Penido N, Tangerina RP, Kosugi EM, de Abreu CE, Vasco MB. Vestibular schwannoma: spontaneous tumor involution. Braz J Otorhinolaryngol. 2007. 73: 867-71
12. Patel EJ, Deep NL, Schecht M, Hagiwara M, Roland JT. Tracking spontaneous vestibular schwannoma regression with volumetric measurements. Laryngoscope. 2021. 131: E1647-52
13. Patnaik U, Prasad SC, Tutar H, Giannuzzi AL, Russo A, Sanna M. The long-term outcomes of wait-and-scan and the role of radiotherapy in the management of vestibular schwannomas. Otol Neurotol. 2015. 36: 638-46
14. Pennings RJ, Morris DP, Clarke L, Allen S, Walling S, Bance ML. Natural history of hearing deterioration in intracanalicular vestibular schwannoma. Neurosurgery. 2011. 68: 68-77
15. Reznitsky M, Petersen MM, West N, Stangerup SE, CayéThomasen P. The natural history of vestibular schwannoma growth-prospective 40-year data from an unselected national cohort. Neuro Oncol. 2021. 23: 827-36
16. Shin YJ, Fraysse B, Cognard C, Gafsi I, Charlet JP, Berges C. Effectiveness of conservative management of acoustic neuromas. Am J Otol. 2000. 21: 857-62
17. Smouha EE, Yoo M, Mohr K, Davis RP. Conservative management of acoustic neuroma: A meta-analysis and proposed treatment algorithm. Laryngoscope. 2005. 115: 450-4
18. Stipkovits EM, Graamans K, Van Dijk JE. Vestibular schwannoma: Negative growth and audiovestibular features. Eur Arch Otorhinolaryngol. 2001. 258: 467-71
19. Vellutini EA, Gomes MQ, Brock RS, Oliveira MF, Salomone R, de Souza Godoy LF. Radiologic features of spontaneous regression of vestibular schwannomas. World Neurosurg. 2020. 135: e488-93
20. Watanabe S, Yamamoto M, Kawabe T, Koiso T, Yamamoto T, Matsumura A. Stereotactic radiosurgery for vestibular schwannomas: Average 10-year follow-up results focusing on long-term hearing preservation. J Neurosurg. 2016. 125: 64-72
21. Whitehouse K, Foroughi M, Shone G, Hatfield R. Vestibular schwannomas-when should conservative management be reconsidered?. Br J Neurosurg. 2010. 24: 185-90
22. Yoshimoto Y. Systematic review of the natural history of vestibular schwannoma. J Neurosurg. 2005. 103: 59-63

