

- Department of Head and Neck Surgery, Neurosurgery Unit, Garibaldi Hospital, Catania, Italy
- Department of Experimental Biomedicine and Clinical Neurosciences, School of Medicine, Postgraduate Residency Program in Neurological Surgery, Neurosurgical Clinic, AOUP “Paolo Giaccone”, Palermo, Italy
- Department of Radiology, ARNAS Garibaldi, Catania, Italy
- Department of Neurosurgery, Cannizzaro Hospital, Catania, Italy.
Correspondence Address:
Gianluca Scalia, Department of Head and Neck Surgery, Neurosurgery Unit, Garibaldi Hospital, Catania, Italy.
DOI:10.25259/SNI_82_2023
Copyright: © 2023 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Gianluca Scalia1, Massimiliano Porzio2, Roberta Costanzo2, Domenico Gerardo Iacopino2, Gianluca Galvano3, Giovanni Federico Nicoletti1, Giuseppe Emmanuele Umana4. Spontaneous spinal epidural hematoma in a pediatric hemophiliac. 24-Feb-2023;14:69
How to cite this URL: Gianluca Scalia1, Massimiliano Porzio2, Roberta Costanzo2, Domenico Gerardo Iacopino2, Gianluca Galvano3, Giovanni Federico Nicoletti1, Giuseppe Emmanuele Umana4. Spontaneous spinal epidural hematoma in a pediatric hemophiliac. 24-Feb-2023;14:69. Available from: https://surgicalneurologyint.com/surgicalint-articles/12169/
Date of Submission
26-Jan-2023
Date of Acceptance
09-Feb-2023
Date of Web Publication
24-Feb-2023
Abstract
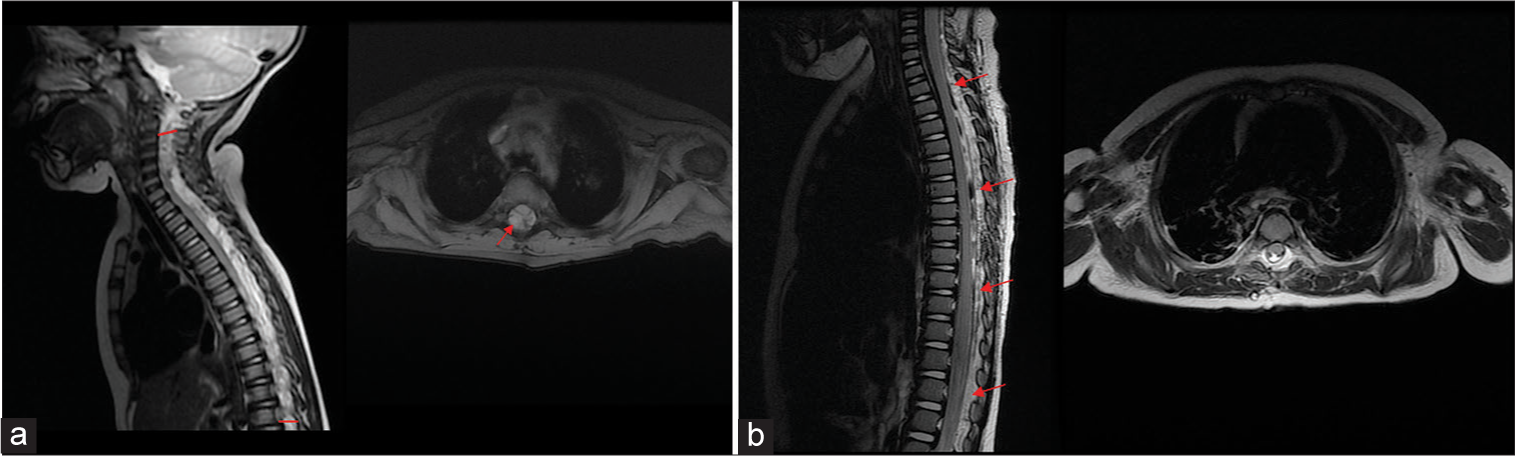
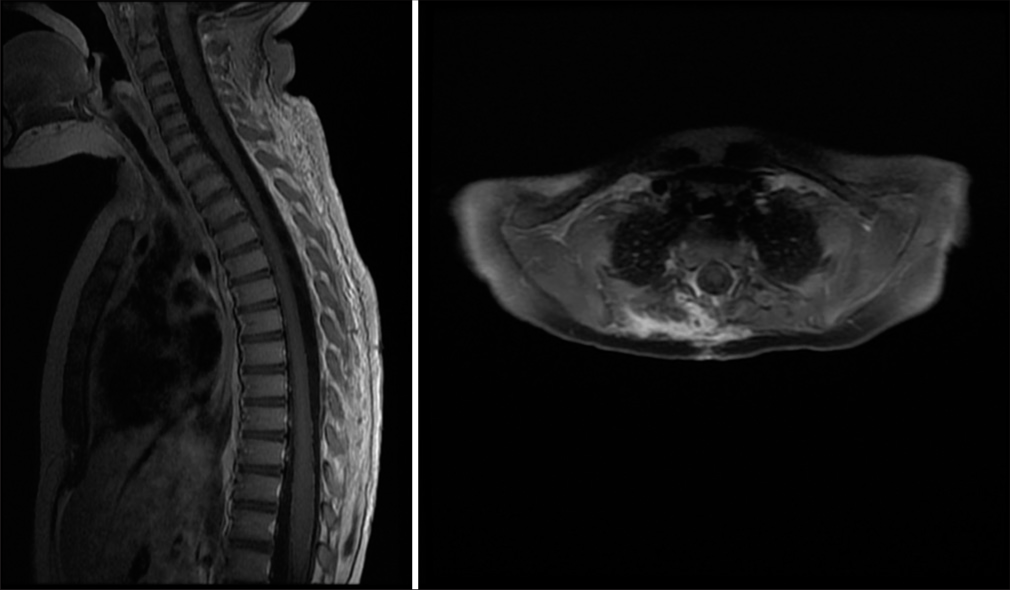
Background: Spontaneous spinal epidural hematomas (SSEH), unrelated to trauma, epidural anesthesia, or surgery, are rare in the pediatric population. Here, a 1-year-old male with hemophilia presented with a magnetic resonance (MR)-documented SSEH and was successfully treated with a C5-T10 right hemilaminectomy.
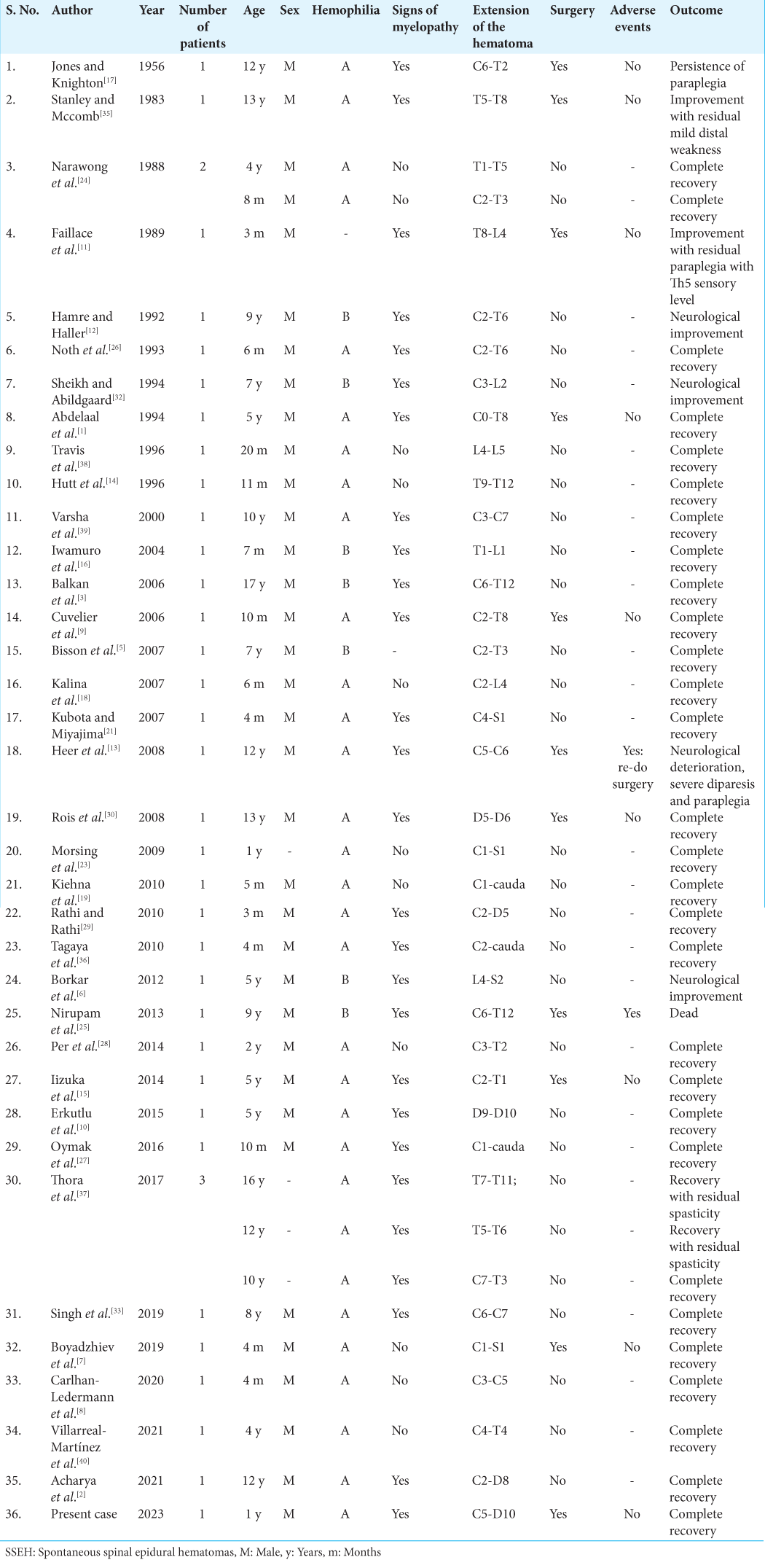
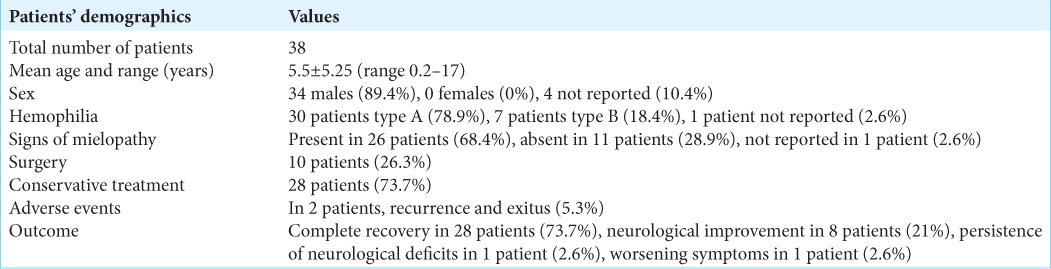
Case Description: A 1-year-old male with hemophilia presented with quadriparesis. The holo-spine magnetic resonance imaging with contrast showed a posterior cervicothoracic compressive epidural lesion extending from C3 to L1 consistent with an epidural hematoma. He underwent a C5 to T10 right-sided hemilaminectomy for clot removal, following which his motor deficits fully resolved. A literature review of SSEH attributed to hemophilia revealed that 28 of 38 cases were effectively treated conservatively, while only 10 cases warranted surgical decompression.
Conclusion: Select patients with SSEH attributed to hemophilia with severe MR-documented cord/cauda equina compromise and significant accompanying neurological deficits may require emergent surgical decompression.
Keywords: Epidural, Hematoma, Hemophilia, Pediatric, Spine
INTRODUCTION
Spontaneous spinal epidural hematomas (SSEH) that develop in the extradural space without accompanying histories of trauma, epidural anesthesia, or surgery represent <1% of all space-occupying spinal lesions. In adults, SSEH occurs with a frequency of 0.1 cases/100,000/year, and account for 0.6% of all spinal hemorrhages; in children, their incidence remains unclear.[
CASE DESCRIPTION
A 1-year-old male with hemophilia A (i.e., severe deficit of factor VIII) presented with the acute and spontaneous onset of severe quadriparesis. Laboratory tests revealed a low hemoglobin (8.5 g/dL), low hematocrit (25.6%), a mildly elevated international normalized ratio (1.34) and partial thromboplastin time (37 s), with reduced prothrombin activity (65 s). The holo-spine magnetic resonance (MR) with contrast showed a large cervicothoracic posterior epidural compressive lesion extending from C3 to L1 that was consistent with an epidural bleed; it was hypointense on T1, and hyperintense on T2-weighted images [
DISCUSSION
Hemophilia is one of the most common hereditary X-linked bleeding disorders attributed to a deficiency of factor VIII. Some patients with hemophilia acutely develop SSEH and present with the rapid onset of paralysis correlated with the levels of MR-documented spinal hemorrhages.[
Surgery
Most adults with SSEH will undergo decompressive laminectomies. However, children may occasionally be managed with less extensive partial laminectomies or single/multiple short-segment laminoplasties.[
CONCLUSION
A 1-year-old male with hemophilia presented with acute quadriparesis attributed to a MR-documented C5-T10 thoracic SSEH resulting in marked cord compression. Following a right-sided C5-T10 hemilaminectomy, the patient was neurologically intact and remained intact for 5 subsequent years during which he developed no spinal deformity.
Ethics approval
There is no ethical issue in this paper.
Declaration of patient consent
Patient’s consent not required as patient’s identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Journal or its management. The information contained in this article should not be considered to be medical advice; patients should consult their own physicians for advice as to their specific medical needs.
References
1. Abdelaal MA, Mcguinness FE, Sagar G. Case report: Spinal extradural haematoma in haemophilia-a-a diagnosis not to be missed. Clin Radiol. 1994. 49: 573-5
2. Acharya A, Bind R, Grewal S, John P. Spontaneous spinal epidural hematoma in a known case of hemophilia a managed conservatively: A rare case report. J Appl Hematol. 2021. 12: 112-4
3. Balkan C, Kavakli K, Karapinar D. Spinal epidural haematoma in a patient with Haemophilia B. Haemophilia. 2006. 12: 437-40
4. Barwar N, Kumar N, Sharma A, Bharti A, Kumar R. A rare presentation of spontaneous spinal epidural hematoma as spinal cord compression and complete paraplegia: A case report and review of the literature. Cureus. 2022. 14: e22199
5. Bisson EF, Dumont T, Tranmer B. Spontaneous spinal epidural hematoma in a child with Hemophilia B. Can J Neurol Sci. 2007. 34: 488-90
6. Borkar SA, Prasad GL, Satyarthee GD, Mahapatra AK. Spontaneous spinal extradural hematoma in a child with Hemophilia B, surgery or medical management-a dilemma?. J Pediatr Neurosci. 2011. 6: 131-3
7. Boyadzhiev D, Dumitriu D. A rare case of back pain in a 4 month-old baby with Type A haemophilia. J Belg Soc Radiol. 2019. 103: 46
8. Carlhan-Ledermann A, Laubscher B, Steinlin M, Ulrich CT, Verma RK, Rizzi M. Spinal epidural hematoma without significant trauma in children: Two case reports and review of the literature. BMC Pediatr. 2020. 20: 77
9. Cuvelier GD, Davis JH, Purves EC, Wu JK. Torticollis as a sign of cervico-thoracic epidural haematoma in an infant with severe Haemophilia A. Haemophilia. 2006. 12: 683-6
10. Erkutlu I, Bay A, Aktekin E. Conservative management of an acute spinal epidural hemorrhage in a child with Hemophilia A with inhibitor. Blood Coagul Fibrinolysis. 2016. 27: 930-2
11. Faillace WJ, Warrier I, Canady AI. In an infant with previously undiagnosed Hemophilia A: Treatment and peri-operative considerations. Clin Pediatr (Phila). 1989. 28: 136-8
12. Hamre MR, Haller JS. Intraspinal hematomas in hemophilia. Am J Pediatr Hematol Oncol. 1992. 14: 166-9
13. Heer JS, Enriquez EG, Carter AJ. Spinal epidural hematoma as first presentation of Hemophilia A. J Emerg Med. 2008. 34: 159-62
14. Hutt J, Herold E, Gilchrist G. Spinal extradural hematoma in an infant with Hemophilia A: An unusual presentation of a rare complication. J Pediatr. 1996. 128: 704-6
15. Iizuka Y, Iizuka H, Nagano K, Tsutsumi S, Nakajima T, Takagishi K. Laminoplasty preserving the deep extensor musculature for a pediatric cervicothoracic epidural hematoma case of hemophilia A. J Pediatr Orthop B. 2014. 23: 584-8
16. Iwamuro H, Morita A, Kawaguchi H, Kirino T, Fernandez H. Resolution of spinal epidural haematoma without surgery in a haemophilic infant. Acta Neurochir (Wien). 2004. 146: 1263-5
17. Jones RK, Knighton RS. Surgery in hemophiliacs with special reference to the central nervous system. Ann Surg. 1956. 144: 1029-34
18. Kalina P, Morris J, Raffel C. Spinal epidural hematoma in an infant as the initial presentation of severe hemophilia. Emerg Radiol. 2008. 15: 281-4
19. Kiehna EN, Waldron PE, Jane JA. Conservative management of an acute spontaneous holocord epidural hemorrhage in a hemophiliac infant: Case report. J Neurosurg Pediatr. 2010. 6: 43-8
20. Kreppel D, Antoniadis G, Seeling W. Spinal hematoma: A literature survey with meta-analysis of 613 patients. Neurosurg Rev. 2003. 26: 1-49
21. Kubota T, Miyajima Y. Spinal extradural haematoma due to haemophilia A. Arch Dis Child. 2007. 92: 498
22. Lan T, Chen Y, Yang XJ, Hu SY, Guo WZ, Ren K. Spontaneous spinal epidural haematoma. J Orthop Translat. 2015. 3: 152-6
23. Morsing IE, Brons P, Draaisma JM, Lindert EJ, Erasmus CE. Hemophilia A and spinal epidural hematoma in children. Neuropediatrics. 2009. 40: 245-8
24. Narawong D, Gibbons VP, Mclaughlin JR, Bouhasin JD, Kotagal S. Conservative management of spinal epidural hematoma in hemophilia. Pediatr Neurol. 1988. 4: 169-71
25. Nirupam N, Pemde H, Chandra J. Spinal epidural hematoma in a patient with Hemophilia B presenting as acute abdomen. Indian J Hematol Blood Transfus. 2014. 30: 54-6
26. Noth I, Hutter J, Meltzer P, Damiano M, Carter L. Spinal epidural hematoma in a hemophilic infant. Am J Pediatr Hematol Oncol. 1993. 15: 131-4
27. Oymak Y, Muminoglu N, Ay Y, Karapinar TH, Köker SA, Töret E. Torticollis in a haemophilic infant with inhibitor: A case of spinal epidural haematoma. Blood Coagul Fibrinolysis. 2016. 27: 576-9
28. Per H, Canpolat M, Tümtürk A, Gumuş H, Gokoglu A, Yikilmaz A. Different etiologies of acquired torticollis in childhood. Childs Nerv Syst. 2014. 30: 431-40
29. Rathi N, Rathi A. Haemophilia a presenting as spontaneous spinal epidural haematoma in a 3-Month-old infant. BMJ Case Rep. 2010. 2010: bcr0520102997
30. Rois PV, López MR, de Vergara BC, de La Lama Zaragoza A, García JG, Uxo JM. Spinal epidural hematoma in hemophilic children: Controversies in management. Childs Nerv Syst. 2009. 25: 987-91
31. Scalia G, Umana GE, Marrone S, Graziano F, Giuffrida A, Ponzo G. Spontaneous anterior cervicothoracic spinal epidural hematoma extending to clivus in SARS-CoV-2 infection. Surg Neurol Int. 2021. 12: 181
32. Sheikh AA, Abildgaard CF. Medical management of extensive spinal epidural hematoma in a child with factor IX deficency. Pediatr Emerg Care. 1994. 10: 26-9
33. Singh S, Philip CC, George U, John MJ. Spinal epidural bleed in hemophilia: A rare site of bleeding with complete resolution with nonsurgical management. J Pediatr Hematol Oncol. 2018. 41: 215-7
34. Soltani S, Nogaro MC, Rougelot C, Newell N, Lim K, Kieser DC. Spontaneous spinal epidural haematomas in children. Eur Spine J. 2019. 28: 2229-36
35. Stanley P, Mccomb JG. Pediatric radiology chronic spinal epidural hematoma in Hemophilia A in a child. Pediatr Radiol. 1983. 13: 241-3
36. Tagaya A, Miyajima Y, Sakamoto M, Ito M, Nakamura L, Ohe H. Spontaneous spinal epidural hematoma in an infant with undiagnosed Hemophilia A. Pediatri Int. 2010. 52: 296-8
37. Thora A, Bhatnagar N, Tiwari A, Lingaiah P, Rustagi N. Nonoperative management of spontaneous epidural hematoma in Hemophilia A. Int J Res Orthop. 2017. 3: 202
38. Travis SF, Greenbaum BH, Mintz M, White RM, Stein S, Steckler RE. Epidural hematoma Pf the cauda equina in a child with Hemophilia A. J Pediatr Hematol Oncol. 1996. 18: 308-10
39. Varsha J, Prashant S, Manohar S, Sachin G. Spinal epidural hematoma in Hemophilia-A A case report. Neuroradiol J. 2000. 13: 635-8
40. Villarreal-Martínez L, Sepúlveda-Orozco MD, GarcíaViera DA, Robles-Sáenz DA, Bautista-Gómez AJ, Ortiz-Castillo . Spinal epidural hematoma in a child with Hemophilia A with high titer inhibitors and follow-up with prophylactic emicizumab: Case report and literature review. Blood Coagul Fibrinolysis. 2021. 32: 418-22

