

- Division of Neurosurgery, Centre Hospitalier de l’Université de Montréal (CHUM), Quebec, Canada.
- Department of Neurosurgery, McGill University, Quebec, Canada.
- Department of Neurosurgery, CHU de Quebec - Hopital l’Enfant-Jesus, Quebec, Canada.
- Department of Surgery, CIUSSS du Nore de L, Ile de Montréal - Hôpital du Sacré-Coeur de Montréa, Montreal, Quebec, Canada.
Correspondence Address:
Lior M. Elkaim, Department of Neurosurgery, McGill University, Montreal, Quebec, Canada.
DOI:10.25259/SNI_1114_2021
Copyright: © 2022 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Sami Obaid1, Lior M. Elkaim2, Charles Gariepy3, Harrison J. Westwick4, Sung-Joo Yuh1, Daniel Shedid1. Spontaneous spinal epidural hematoma related to amphetamine abuse: A case report. 04-Feb-2022;13:35
How to cite this URL: Sami Obaid1, Lior M. Elkaim2, Charles Gariepy3, Harrison J. Westwick4, Sung-Joo Yuh1, Daniel Shedid1. Spontaneous spinal epidural hematoma related to amphetamine abuse: A case report. 04-Feb-2022;13:35. Available from: https://surgicalneurologyint.com/surgicalint-articles/11376/
Date of Submission
07-Nov-2021
Date of Acceptance
08-Jan-2022
Date of Web Publication
04-Feb-2022
Abstract
Background: Spontaneous spinal epidural hematoma (SSEH) is a rare condition that is typically associated with hypertension, the use of antithrombotic or sympathomimetic drugs. Here, we report a case of SSEH attributed to the use of amphetamines.
Case Description: A 27-year-old amphetamine user presented with the sudden onset of paraplegia (Frankel A) following amphetamine use. An MRI revealed C7–T2 spinal cord compression due to an epidural hematoma. Following a negative angiogram, the SSEH was removed, and the patient markedly recovered. Notably, by exclusion, the etiology for the SSEH was attributed to the use of amphetamines.
Conclusion: Here, we demonstrate the case of a 27-year-old male who presented paraplegic due to an acute C7– T2 SSEH secondary to amphetamine abuse.
Keywords: Amphetamine, Epidural, Hematoma, Spine
INTRODUCTION
Spontaneous spinal epidural hematomas (SSEHs) are rare, occurring in approximately 1/1 million individuals/year. Magnetic resonance (MR) studies performed in suddenly myelopathic patients with SSEH will document the location and size of these hemorrhages. Emergent surgical decompression and drainage are typically warranted.[
CASE PRESENTATION
History
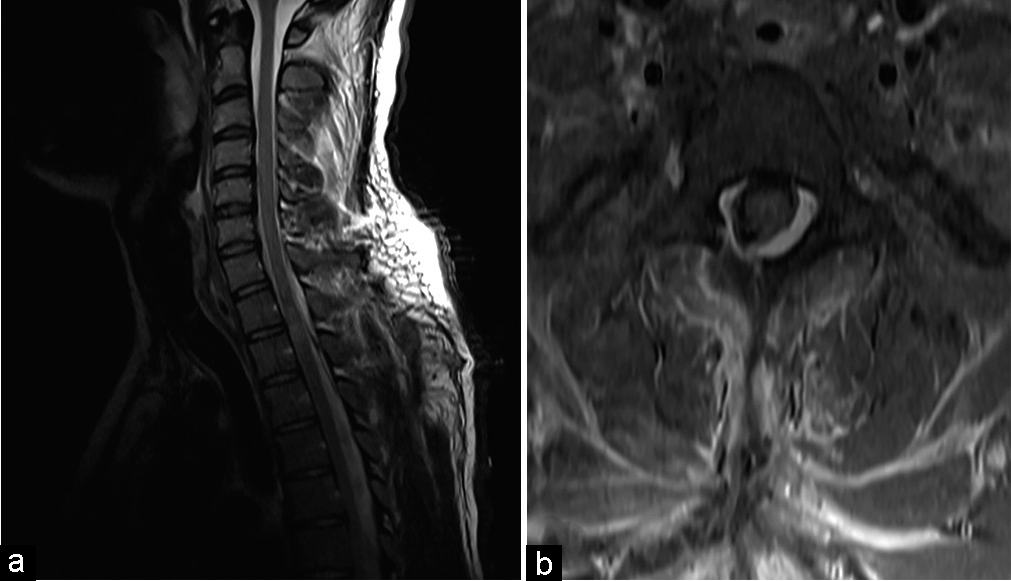
A 27-year-old chronic amphetamine abuser acutely presented with paraplegia just after taking amphetamines. Over a 4 h period, he developed total motor and sensory loss (i.e., Frankel Grade A). The only abnormal laboratory study was the urine toxicology screen that showed the presence of amphetamines. An emergent MRI showed a posterolateral right-sided C2–T6 acute SSEH that caused marked C7–T2 cord compression [

Figure 1:
Initial spinal MRI. Sagittal (a) and axial (b) T2-weighted sequences revealing a right-sided hyperintense posterolateral epidural collection extending from C2 to T6. A significant compression was observed between C7 and T2 (arrow). Signal changes were characteristic of an epidural hematoma.
Surgery
The patient underwent an emergent right-sided C7–T2 hemilaminectomy for hematoma drainage. Neither infection nor tumor was present. The histopathology was consistent with an acute hematoma.
Postoperative MR and clinical course
The day after surgery, an MRI documented near-total drainage of the hematoma [
DISCUSSION
SSEHs typically progress rapidly and often lead to paralysis. Predisposing factors usually include antithrombotic medication, hypertension, and cocaine abuse. We found only one other case of spinal hemorrhage related to amphetamine abuse in the literature. Contrasting the SSEH described in this paper, the case consisted of spinal subdural and subarachnoid hemorrhage after amphetamine use.[
Management of SSEH
SSEH requires early surgical spinal cord decompression and drainage to optimize the likelihood of neurological recovery. Further, patients whose SSEH is attributed to amphetamine use typically require strict blood pressure control (i.e., medical management). Those with myelopathy and significant neurological deficits usually require urgent MRI and prompt surgical intervention to achieve the best outcomes.[
Here, the patient presented with a 3-segment cervicothoracic SSEH that was decompressed within 6 h of its onset; the patient’s excellent postoperative neurological recovery was largely attributed to early recognition, diagnosis, and surgical decompression.
CONCLUSION
Here, we presented a 27-year-old male whose abuse of amphetamines resulted in the sudden onset of paraplegia due to an acute MR-documented C2–T6 acute SSEH.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Kreppel D, Antoniadis G, Seeling W. Spinal hematoma: A literature survey with meta-analysis of 613 patients. Neurosurg Rev. 2003. 26: 1-49
2. Lee HH, Park SC, Kim Y, Ha YS. Spontaneous spinal epidural hematoma on the ventral portion of whole spinal canal: A case report. Korean J Spine. 2015. 12: 173
3. Liu CL, Cheng CH, Cho DY. Rhabdomyolysis accompanied by spontaneous spinal subdural and subarachnoid hematoma related to amphetamine abuse. Spine. 1976. 35: 71-3
4. Ohba T, Ebata S, Haro H. Influence of postoperative hypertension on the development of spinal epidural hematoma. Orthop Surg. 2017. 9: 386-90
5. Riaz S, Jiang H, Fox R, Lavoie M, Mahood JK. Spontaneous spinal epidural hematoma causing Brown-Sequard syndrome: Case report and review of the literature. J Emerg Med. 2007. 33: 241-4
6. Spengos K, Sameli S, Tsivgoulis G, Vassilopoulou S, Vemmos K, Zakopoulos N. Spontaneous spinal epidural hematoma in an untreated hypertensive patient. Eur J Intern Med. 2005. 16: 451-3

