

- Department of Neurosurgery, Fuji Brain Institute and Hospital, Fujinomiya-shi, Shizuoka, Japan
Correspondence Address:
Tomohiro Inoue
Department of Neurosurgery, Fuji Brain Institute and Hospital, Fujinomiya-shi, Shizuoka, Japan
DOI:10.4103/2152-7806.200576
Copyright: © 2017 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Hiroki Hongo, Tomohiro Inoue, Akira Tamura, Isamu Saito. Surgical strategy to minimize ischemia during trapping/resection of giant extracranial carotid artery aneurysm stratified by collateral evaluation. 20-Feb-2017;8:28
How to cite this URL: Hiroki Hongo, Tomohiro Inoue, Akira Tamura, Isamu Saito. Surgical strategy to minimize ischemia during trapping/resection of giant extracranial carotid artery aneurysm stratified by collateral evaluation. 20-Feb-2017;8:28. Available from: http://surgicalneurologyint.com/?post_type=surgicalint_articles&p=8301
Date of Submission
09-Jun-2016
Date of Acceptance
30-Dec-2016
Date of Web Publication
20-Feb-2017
Abstract
Background:Extracranial carotid artery aneurysm (ECAA) is a rare clinical entity, and no standard treatment strategy has been established for this condition.
Methods:Data from three patients who underwent surgical treatment of enlarging giant ECAAs were retrospectively reviewed. Based on the collateral status, as evaluated by preoperative digital subtraction angiography (DSA), surgical strategy was stratified into (1) high flow bypass followed by cervical ICA (internal carotid artery) ligation, when the collateral status was judged as poor/fair or (2) direct cervical repair with patch application after aneurysmal wall resection when the collateral status was judged as robust. Postoperative results were evaluated by magnetic resonance imaging (MRI).
Results:Postoperative follow-up (day 0 to 1, as well as midterm at approximately 6 months) confirmed completely trapped aneurysm with successful robust bypass and robust anterograde flow of the reconstructed cervical carotid artery on magnetic resonance angiography with no additional ischemic lesions on diffusion weighted imaging and T2-weighted imaging when compared with preoperative imaging in all three patients. Postoperatively, there was no stroke event during the midterm follow-up at 6 months.
Conclusions:Clinical results of ECAAs treated by a surgical strategy stratified based on collateral status, as evaluated by preoperative DSA, were favorable, without postoperative ischemic event, and with satisfactory mid-term MRI results.
Keywords: Direct repair, extracranial carotid artery aneurysm, high flow bypass
INTRODUCTION
Extracranial carotid artery aneurysms (ECAA) is a rare entity and is involved in only 2% of all cervical carotid procedures.[
Few case series of patients with ECAAs who were treated with direct surgical repair noted a relatively high incidence of postoperative complications, most of which were related to cerebral ischemia during surgery.[
MATERIALS AND METHODS
We retrospectively reviewed three consecutive patients who underwent surgical treatment of enlarging giant cervical carotid aneurysm at the Fuji Brain Institute and Hospital between January 2007 and October 2015. During this time, 667 patients underwent surgical clipping for intracranial aneurysms and 429 patients underwent carotid endarterectomy for atherosclerotic cervical carotid lesions at our hospital. All study protocols were approved by the Institutional Review Board at the Fuji Brain Institute and Hospital, and all individuals provided informed consent before the surgery.
Preoperative evaluation
Presenting symptoms and medical comorbidities, such as hypertension, diabetes mellitus, dyslipidemia, and coronary disease, were recorded after medical chart review.
Preoperative magnetic resonance imaging (MRI) evaluation, including diffusion-weighted imaging (DWI), T2-weighted imaging (T2WI), and magnetic resonance angiography (MRA), as well as cervical MRI was performed in all patients. Cervical computed tomography (CT) scan was also performed to evaluate the geometry of the ECAA. Preoperative digital subtraction angiography (DSA) was performed to evaluate the collateral status in detail. Collateral through anterior communicating artery was evaluated by contralateral carotid injection during ipsilateral manual compression of CCA (Matas study). Collateral through posterior communicating artery was evaluated by vertebral injection during ipsilateral manual compression of CCA (Allcock study). When ipsilateral MCA area was opacified symmetrically/synchronously compared to contralateral MCA area during Matas study (and/or as compared to posterior cerebral artery during Allcock study), the collateral status was judged as robust. In contrast, when ipsilateral MCA opacification was delayed/faint compared to contralateral MCA/posterior cerebral artery during Matas/Allcock study, the collateral status was judged as fair. When we could not identify collateral circulation either by Matas nor Allcock study, the collateral status was judged as poor.
Surgical strategy was stratified into high-flow bypass followed by cervical ICA ligation, when (1) the collateral status was judged as poor/fair and (2) when the direct exposure of the normal distal end of the cervical ICA was anticipated to be quite difficult without aneurysmal decompression using a substantially long duration of cervical ICA occlusion. Direct cervical repair with patch application after aneurysmal wall resection was indicated when (1) the collateral status was judged as robust, (2) the geometry of the aneurysm was suitable for resection with a resultant only partial wall defect in the cervical CCA to ICA, and (3) insertion of the shunt was anticipated to be easy, therefore, requiring only minimal cervical ICA occlusion time.
Operative procedure
High-flow bypass followed by trapping of the cervical aneurysm
Under general anesthesia, with continued antiplatelet medication preoperatively, the giant ECAA, CCA, and external carotid artery (ECA) were exposed by cervical skin incision along the anterior edge of sternocleidomastoid muscle. It was difficult to expose the distal end of the ICA over the giant aneurysm at this stage. Then, a skin incision was made just over the superficial temporal artery (STA) parietal branch. Under microscopy, meticulous STA dissection was conducted. Then, the skin incision was extended toward the forehead and a skin flap was reflected. Simultaneously, a radial artery graft was harvested. After craniotomy, STA-middle cerebral artery (MCA) anastomosis was performed between the STA and the recipient M3 just distal to the site of the M2-radial artery (RA) graft anastomosis. Then, the M2-RA graft anastomosis was performed; during that time, the distal area of the occluded M2 was perfused by preceding STA-MCA bypass. The proximal end of the RA graft was passed under the subzygomatic tunnel and extracted through the space between the digastric muscle and the hypoglossal nerve. The proximal end of the RA graft was anastomosed to the ECA. Then, the cervical ICA proximal to the giant aneurysm was temporarily clamped, and successful high flow bypass was confirmed by microvascular Doppler evaluation. At this stage, by compressing the aneurysm, we could expose the normal distal end of the cervical ICA for the first time. After confirming that motor evoked potential (MEP) and somatosensory evoked potential (SSEP) remained stable over 20 min, both ends of the aneurysm were ligated. The aneurysm was opened and decompressed, however, we did not dissect the posterior wall of the aneurysm to avoid injury to the lower cranial nerves, which could have been stretched and adhered to the distended aneurysmal wall [
Resection of cervical aneurysmal wall and direct repair using synthetic patch graft
Under general anesthesia, the giant ECAA, CCA, ECA, as well as the distal end of ICA were exposed by cervical skin incision along the anterior edge of the sternocleidomastoid muscle. Shunting was performed with a commercially available shunt to encompass the proximal CCA and the distal end of the ICA. The aneurysmal wall was resected. With a synthetic commercially available patch graft [polytetrafluoroethylene graft (Gore-Tex)], the defect in the carotid arterial wall was repaired. SSEPs were recorded during carotid occlusion and during shunting time to assess for intraoperative ischemia [
Postoperative evaluation
Postoperative serial CT evaluations were performed in all cases. In all cases, postoperative MRI with DWI, T2WI, and MRA were performed on postoperative days 0 and 1. DSA for the assessment of bypass function and cervical carotid status was performed approximately 1 week postoperatively in all patients. A mid-term MRI follow-up study was performed at approximately 6 months after surgery.
RESULTS
All patients presented with enlarging cervical mass without focal neurological deficit. Two patients reported gradual idiopathic enlargement of the aneurysm over 1 year, and one patient reported rapid enlargement over several weeks after minor blunt cervical injury. Enhanced CT and MRI of the cervical portion revealed a 3–4.8 cm mass in maximum diameter originating from the cervical ICA/CCA in all the three patients. Two of the three patients showed extensive intraluminal thrombus. Preoperative collateral evaluation by DSA revealed poor-to-fair collaterals in two patients in conjunction with extensive fusiform dilatation of the cervical ICA portion and a quite high positioned normal distal ICA end, thereby rendering direct interposition graft repair quite difficult. In one patient, collateral flow was robust, the aneurysm neck was identified in the CCA just proximal to the bifurcation, and the morphology resembled that of a side-wall aneurysm rather than fusiform dilatation. Thus, the former two patients with inadequate collateral flow as well as fusiform aneurysm underwent high flow ECA-RA-M2 bypass before trapping of the aneurysm. The last patient underwent direct resection of the cervical aneurysmal wall and underwent repair with a synthetic patch with use of an indwelling shunt. The former two patients continued to have normal MEP and SSEP throughout surgery, and the last patient also showed normal SSEP during carotid clamping and shunting. None of the patients had new neurological deficits postoperatively. Immediate postoperative as well as postoperative day 1 DWI showed no ischemic lesion related to the surgical procedure in any of the patients. MRA demonstrated robust bypass flow and trapping of the cervical aneurysm in two patients and smooth anterograde flow signal in repaired cervical portion in one patient. Arterial spin labelling (ASL) demonstrated symmetrical cerebral blood flow (CBF) on postoperative day 0 to 1 in all patients, suggesting that there was no reperfusion injury or postoperative hyperperfusion due to intraoperative dense ischemic impact. DSA revealed complete trapping of the ICA and good patency of the EC-RA-M2 bypass in two patients and demonstrated smooth anterograde flow of the reconstructed cervical ICA in one patient. In midterm postoperative MRA evaluation at 6 months, no additional new ischemic lesion was identified in T2WI, and robust high flow bypass or widely patent cervical ICA was confirmed. Further, ASL demonstrated symmetrical CBF in all patients [
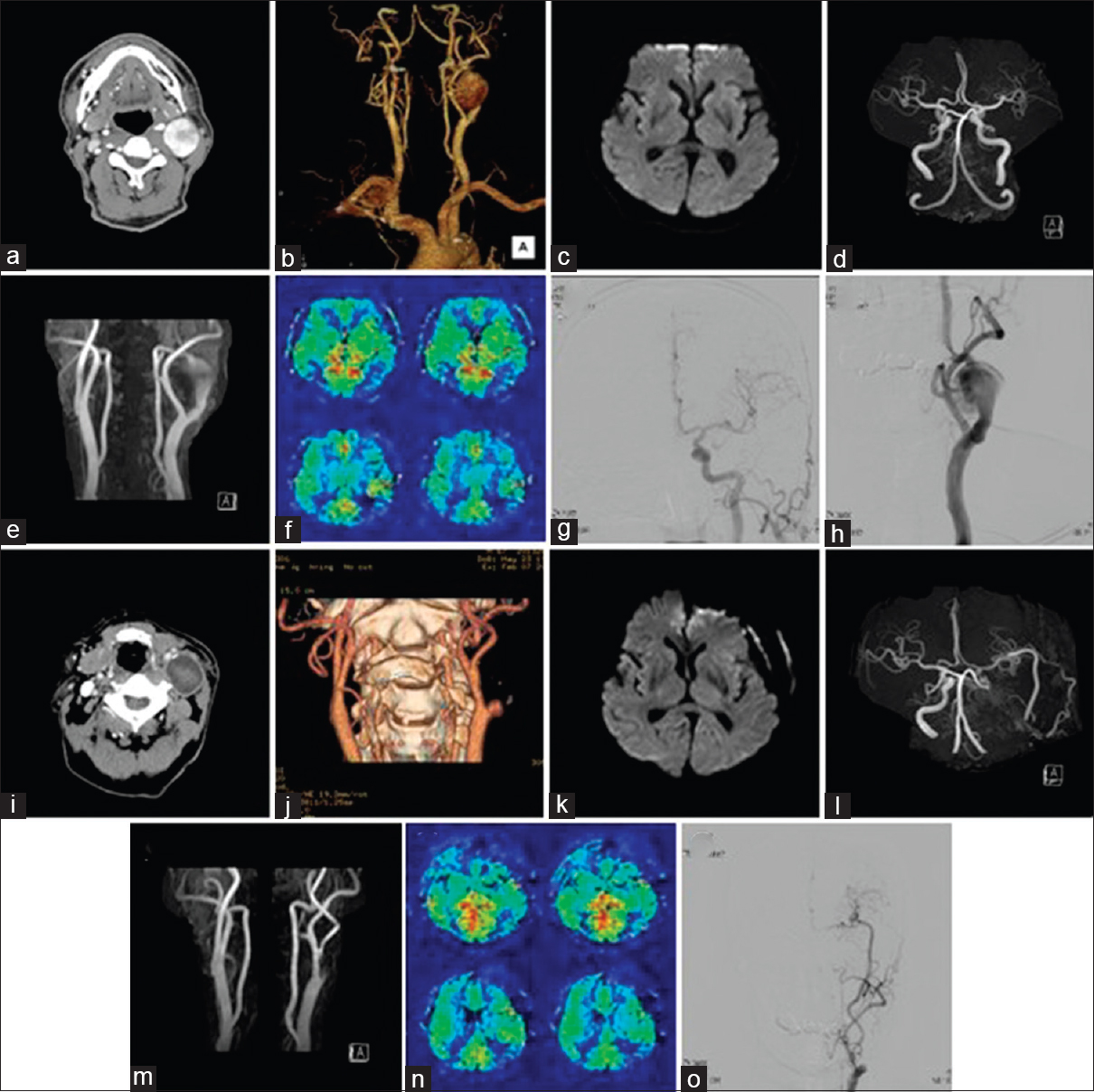
Figure 1
Case 1. A 67-year-old male who presented with enlarging left cervical mass over the past year. Enhanced CT reveals a 4-cm mass originating from the left cervical ICA (a, b). Preoperative DWI reveals no associated ischemic lesion (c). MRA (d, e) demonstrates a giant partially thrombosed left cervical ICA aneurysm. Preoperative ASL shows symmetrical CBF (f). Preoperative DSA (g, h) confirms a fusiform left cervical ICA aneurysm. Postoperative enhanced CT demonstrates no enhancement of the completely trapped cervical ICA aneurysm (i, j). Postoperative DWI (k) and MRA (l, m) demonstrate no ischemic lesion related to the surgical procedure and demonstrate robust bypass flow. Postoperative ASL (n) shows symmetrical CBF, suggesting that there is no reperfusion injury related to intraoperative dense ischemic stress. DSA confirms complete trapping of the ICA and good patency of the EC-RA-M2 bypass (o)
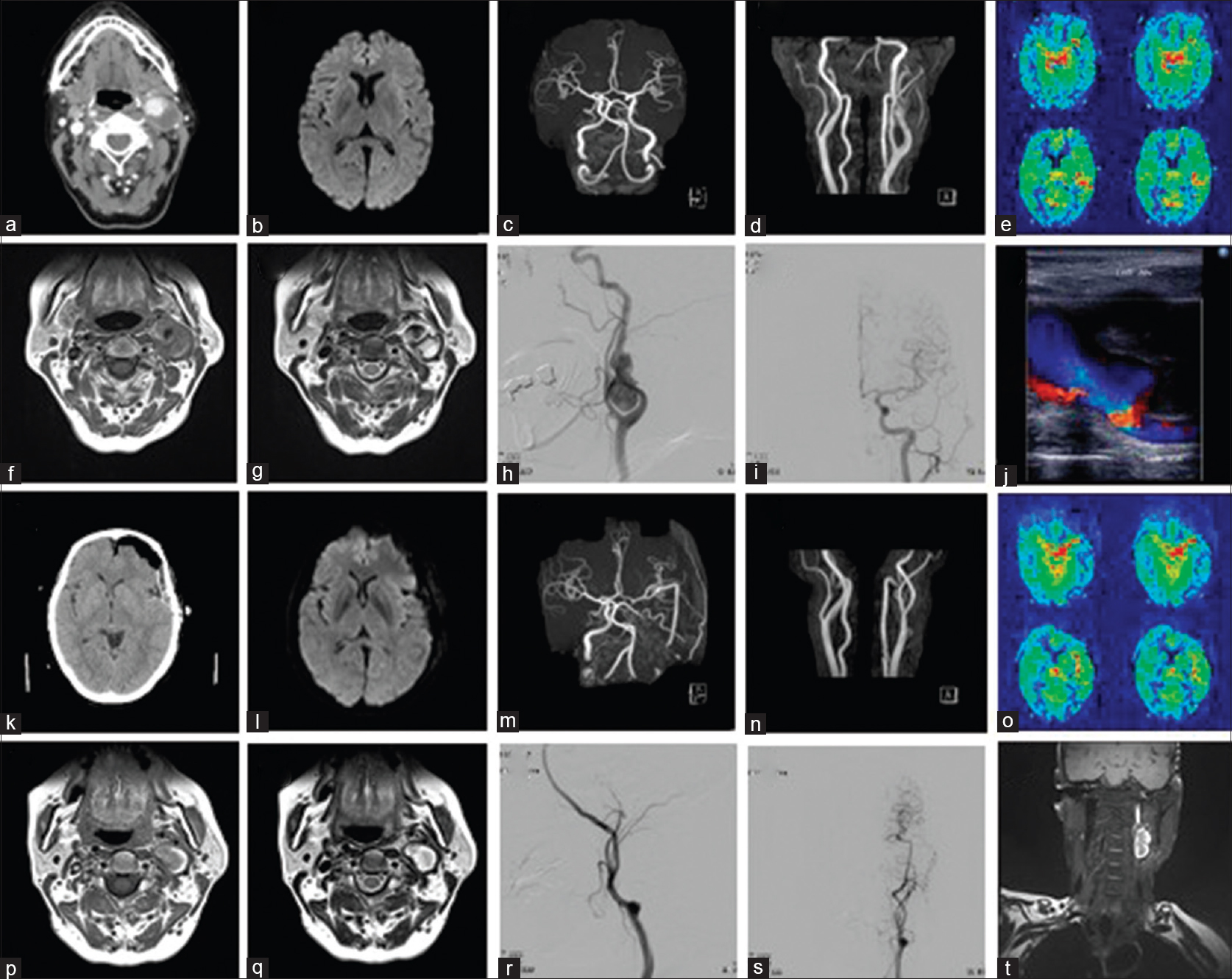
Figure 2
Case 2. A 66-year-old female who presented with enlarging left cervical mass over the past year. Enhanced CT (a) demonstrates a giant, partially thrombosed left cervical ICA aneurysm. Preoperative DWI demonstrates no ischemic lesion (b). MRA (c and d) demonstrates a giant, partially thrombosed left cervical ICA aneurysm. Preoperative ASL (e) demonstrates symmetrical perfusion. T2-weighted MRI (f and g), demonstrates a giant, partially thrombosed left cervical ICA aneurysm. DSA reveals it to be a fusiform cervical ICA aneurysm 4.8 cm in diameter with intramural thrombus (h and i). Cervical color Doppler sonography (j) shows a giant, partially thrombosed left cervical ICA aneurysm with some turbulent flow. Postoperative CT (k) and DWI (l) did not show a hemorrhagic lesion or ischemic lesion. Postoperative MRA (m and n) shows robust bypass and complete trapping of the cervical giant aneurysm. Postoperative ASL (o) shows symmetrical CBF, suggesting that there is no reperfusion injury related to intraoperative dense ischemic stress. Postoperative T1-weighted (p), T2-weighted (q) MRI reveals that the trapped cervical ICA aneurysm has completely thrombosed. DSA confirms complete trapping of the ICA and good patency of the EC-RA-M2 bypass (r and s). MPRAGE imaging reveals that trapped ICA aneurysm is completely thrombosed (t)
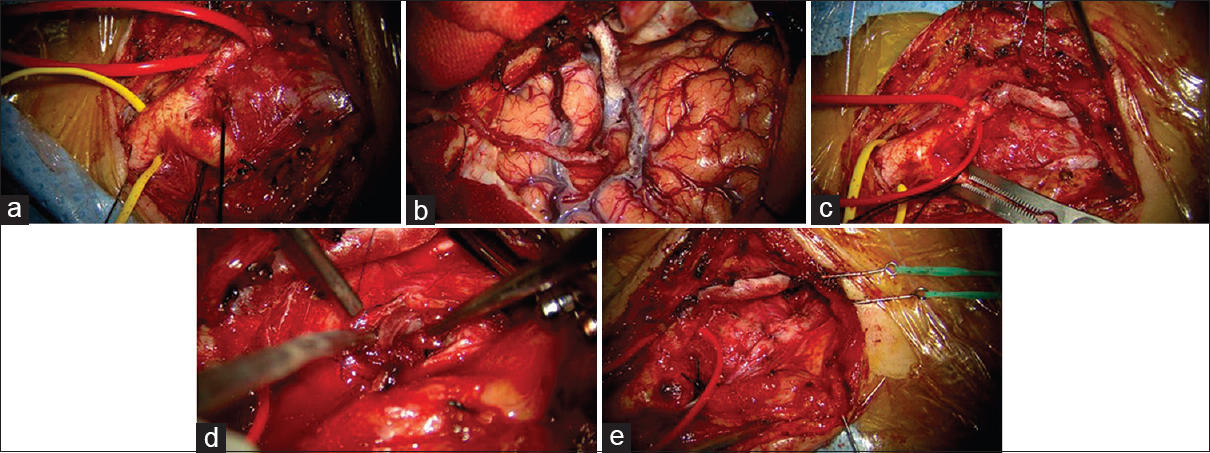
Figure 3
Intraoperative photo of Case 2. A 66-year-old female who presented with enlarging left cervical mass over the past year. Cervical giant aneurysm, the common carotid artery, the external carotid artery, and the distal end of internal carotid artery are exposed (a). M2-RA graft anastomosis is performed while STA-MCA bypass perfuses the distal area of the occluded M2 (b). Proximal end of the RA graft is anastomosed to the external carotid artery (c). The intraluminal thrombus is removed, and the aneurysmal wall is sutured (d and e)
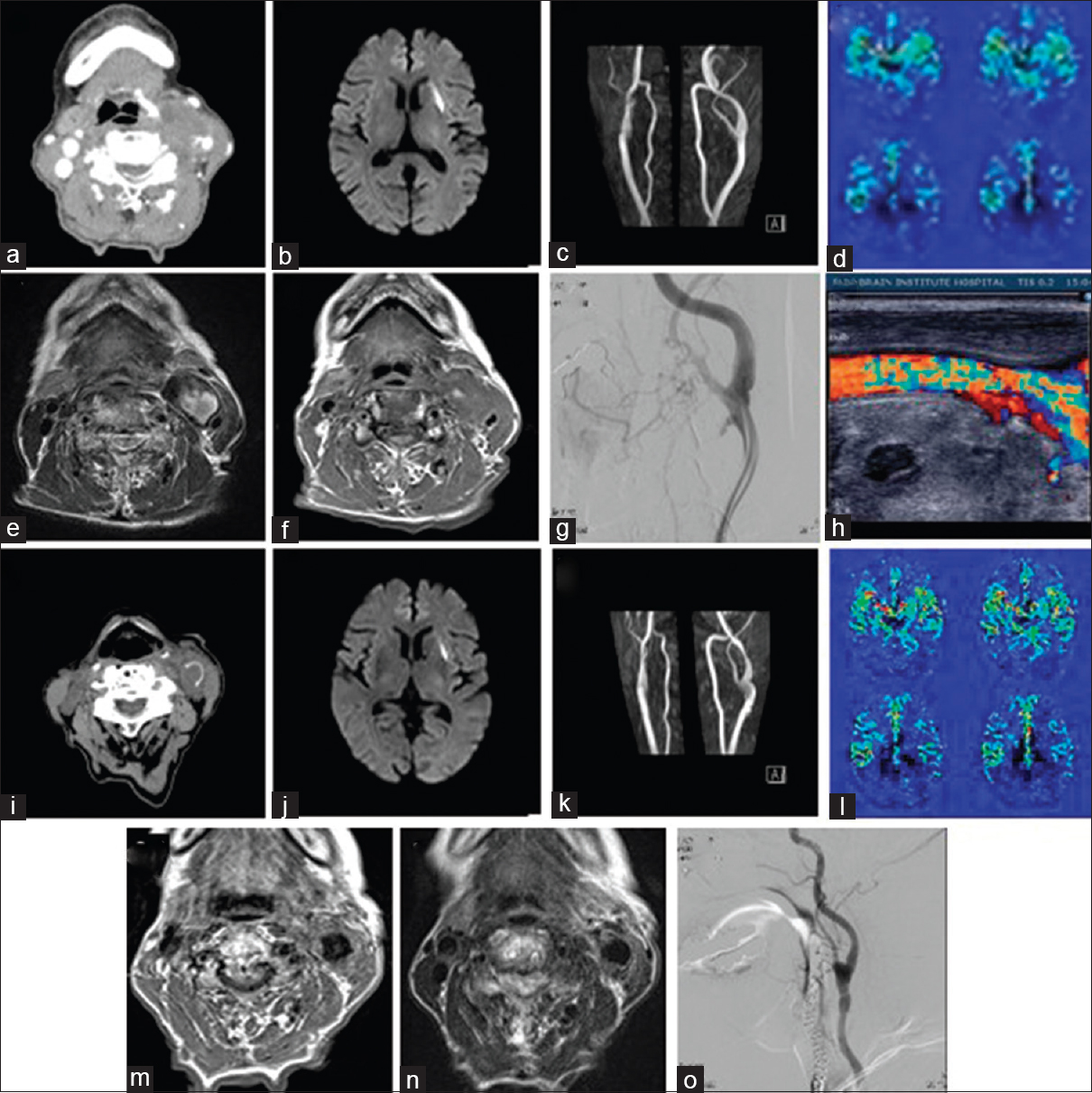
Figure 4
An 83-year-old female who presented with rapid enlargement of a left cervical mass during several weeks after a minor blunt cervical injury. Enhanced CT (a) shows a thrombosed left cervical mass. Preoperative DWI (b) shows a small ischemic lesion, suggesting embolic spray from the intra-aneurysmal thrombi. (c) preoperative cervical MRA shows almost normal left cervical CCA to ICA signal, (d) preoperative ASL shows symmetrical cerebral blood flow. T1-weighted (e) and T2-weighted (f) cervical MRI shows a thrombosed, well-bordered mass in the left neck, 3 cm in diameter, next to the left common carotid artery. DSA reveals extravasation of contrast material from a small pore on the anterior wall of the left common carotid artery (g). Cervical color Doppler sonography demonstrates the same finding (h). Nonenhanced CT (i) shows disappearance of the aneurysm. Postoperative DWI (j) shows no new ischemic lesion when compared with a preoperative study. Postoperative MRA (k) demonstrates good patency and smooth anterograde flow of the CCA. Postoperative ASL (l) shows symmetrical CBF, suggesting that there was no reperfusion injury related to intraoperative dense ischemic stress. T1-weighted (m) and T2-weighted (n) cervical MRI demonstrates disappearance of the aneurysm. DSA (o) demonstrates good patency and smooth anterograde flow of the CCA
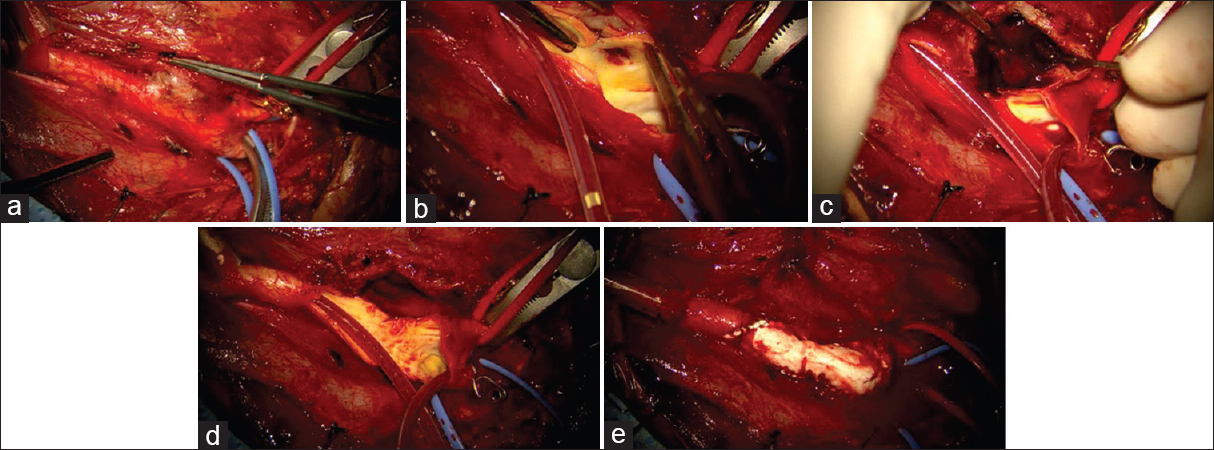
Figure 5
Intraoperative photo of Case 3. An 83-year-old female who presented with rapid enlargement of a left cervical mass over several weeks after minor blunt cervical injury. Cervical giant aneurysm, the common carotid artery, the external carotid artery, and the distal end of internal carotid artery are exposed (a). Shunting is performed to encompass the proximal common carotid artery and the distal end of the internal carotid artery (b). Intra-aneurysmal thrombi were removed, and the aneurysmal wall is resected (c and d). The carotid artery wall is repaired with a synthetic commercially available patch graft (e)
DISCUSSION
ECAAs are very rare, and intermediate-to-large single-institutional case series are seldom reported. According to previous reports, the most frequent etiology of ECAAs is atherosclerosis (in approximately 50% of the cases). Other etiologies have been reported, including traumatic, iatrogenic (post-carotid endarterectomy), infections, and systemic diseases, such as fibromuscular dysplasia or collagen diseases, including Marfan's syndrome.[
However, the treatment strategy of this difficult entity with respect to minimizing intraoperative ischemic injury, especially by meticulously evaluating the collateral flow in preoperative DSA, has not been discussed well to date. Accordingly, some case series reported a relatively high incidence of postoperative ischemic complications related to intraoperative ICA temporary occlusion.[
Meticulous collateral evaluation by balloon occlusion test, which would be a more predictive and reliable test, was not performed due to the unavailability of an endovascular team in our institution. Even with endovascular expertise, we would have avoided balloon occlusion test because of the embolic risk related to the balloon placement distal to the partially thrombosed enlarging aneurysm compared to the simple manual compression of common carotid artery far proximally to the cervical ICA bifurcation. In addition, we prefer the trapping/resection of the aneurysm in conjunction with reconstruction/restoration of flow whenever possible even in robust collateral cases because the long-term cerebral ischemic risk would not be predictable.
Some studies reported that the disadvantage of surgical treatment was a risk of injury to adjacent lower cranial nerves, occurring in as many as 40% of the cases.[
Endovascular stenting is an emerging alternative treatment to direct surgical treatment with promising results.[
CONCLUSION
Treatment of ECAAs is indicated mainly to prevent thromboembolic events caused by intra-aneurysmal thrombi. Although surgical treatment is preferred at present, the high risk of operative complications, such as intraoperative ischemia due to prolonged ICA occlusion as well as cervical cranial nerve damage, are concerns. We described three cases of ECAAs treated by a surgical strategy stratified based on collateral status as evaluated by preoperative DSA. None of these patients had postoperative ischemic events, and mid-term MRI results were also satisfactory.
Study limitations
First, this was a retrospective analysis with its associated inherent limitations. Second, this was a study involving a small number of patients, mainly because it was difficult to recruit a large number of consecutive patients who fulfilled the inclusion criteria from a single institution. The surgical treatment strategy of ECAA based on the preoperative collateral evaluation has not been previously investigated in a case series. Additional cases are required to definitively determine the safety and feasibility of this approach for preventing intraoperative ischemia during surgery of ECAA.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Choudhary AS, Evans RJ, Naik DK, Tripathi RK, Wickremesekera JK. Surgical management of extracranial carotid artery aneurysms. ANZ J Surg. 2009. 79: 281-7
2. El-Sabrout R, Cooley DA. Extracranial carotid artery aneurysms: Texas Heart Institute experience. J Vasc Surg. 2000. 31: 702-12
3. Fankhauser GT, Stone WM, Fowl RJ, O’Donnell ME, Bower TC, Meyer FB. Surgical and medical management of extracranial carotid artery aneurysms. J Vasc Surg. 2015. 61: 389-93
4. Gupta R, Thomas AJ, Masih A, Horowitz MB. Treatment of extracranial carotid artery pseudoaneurysm with stent grafts: Case series. J Neuroimaging. 2008. 18: 180-3
5. Li Z, Chang G, Yao C, Guo L, Lie Y, Wang M. Endovascular stenting of extracranial carotid artery aneurysm: A systematic review. Eur J Vasc Endovasc Surg. 2011. 42: 419-26
6. Rosset E, Albertini JN, Magnan PE, Ede B, Thomassin JM, Branchereau A. Surgical treatment of extracranial internal carotid artery aneurysms. J Vasc Surg. 2000. 31: 713-23
7. Schievink WI, Piepgras DG, McCaffrey TV, Mokri B. Surgical treatment of extracranial internal carotid artery dissecting aneurysms. Neurosurgery. 1994. 35: 809-16
8. Siablis D, Karnabatidis D, Katsanos K, Mastronikolis N, Zabakis P, Kraniotis P. Extracranial internal carotid artery aneurysms: Report of a ruptured case and review of the literature. Cardiovasc Intervent Radiol. 2004. 27: 397-401
9. Szopinski P, Ciostek P, Kielar M, Myrcha P, Pleban E, Noszczyk W. A series of 15 patients with extracranial carotid artery aneurysms: Surgical and endovascular treatment. Eur J Vasc Endovasc Surg. 2005. 29: 256-61
10. Welleweerd JC, den Ruijter HM, Nelissen BGL, Bots ML, Kappelle LJ, Rinkel GJE. Management of extracranial carotid aneurysm. Eur J Vasc Endovasc Surg. 2015. 50: 141-7
Commentary
Eric Nussbaum- St. Joseph's Hospital; Twin Cities, MN, USA E-mail:
lnussbaum@comcast.net
The authors should be congratulated for achieving technically excellent outcomes in a challenging group of patients with enlarging extracranial internal carotid artery aneurysms. In this setting, we have used local aneurysm resection with direct primary vascular repair in several cases. Nevertheless, with emerging endovascular options, it has been our practice to employ endovascular stenting with primary vessel preservation as the preferred treatment rather than relying on bypass with vascular sacrifice for this rare entity when we have not felt that the vessel could be primarily reconstructed. In particular, one could question the advisability of operating on an 83-year-old patient rather than first attempting an endovascular approach. In any case, we thank the authors for sharing their experience with this unusual entity.

