

- Program in Health Sciences-IAMSPE, Department of Neurosurgery, Sepaco Hospital, São Paulo, Brazil.
- Department of Neurosurgery, Sepaco Hospital, São Paulo, Brazil.
- Program in Health Sciences-IAMSPE, São Paulo, Brazil.
Correspondence Address:
Ítalo Teles de Oliveira Filho
Program in Health Sciences-IAMSPE, São Paulo, Brazil.
DOI:10.25259/SNI_380_2019
Copyright: © 2019 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Ítalo Teles de Oliveira Filho, Paulo Cesar Romero, Emílio Afonso França Fontoura, Saul Dalla de Oliveira, Ricardo Vieira Botelho. Symptomatic foramen of Magendie arachnoid cyst in an elderly patient: The second case report in the literature. 27-Sep-2019;10:189
How to cite this URL: Ítalo Teles de Oliveira Filho, Paulo Cesar Romero, Emílio Afonso França Fontoura, Saul Dalla de Oliveira, Ricardo Vieira Botelho. Symptomatic foramen of Magendie arachnoid cyst in an elderly patient: The second case report in the literature. 27-Sep-2019;10:189. Available from: http://surgicalneurologyint.com/surgicalint-articles/9674/
Date of Submission
25-Aug-2019
Date of Acceptance
04-Sep-2019
Date of Web Publication
27-Sep-2019
Abstract
Background: Arachnoid cysts are benign extra-axial lesions corresponding to 1% of intracranial expansive lesions. They are usually incidental findings in asymptomatic patients. Most cases are congenital, and when symptomatic are diagnosed in childhood or adolescence. Symptomatic arachnoids cyst in elderly patients is very rare. This report documents the second case in the literature of a symptomatic elderly patient with an arachnoid cyst located in the foramen of Magendie.
Case Description: A 68-year-old male had weakness in the lower limbs, imbalance, and gait disturbance for 3 years, associated with frequent falls. The patient complained of paresthesia in the upper right limb and right hemiface. An magnetic resonance imaging showed a massive cystic lesion in the posterior fossa in the foramen of Magendie. A median suboccipital craniectomy was performed, and the cyst was removed.
Conclusion: This case report adds to the literature the second case of a patient with a symptomatic arachnoid cyst in the posterior fossa successfully treated by surgery.
Keywords: Arachnoid cyst, Elderly, Foramen of Magendie, Midline, Posterior fossa
INTRODUCTION
Arachnoid cysts are benign extra-axial lesions corresponding to 1% of intracranial expansive lesions.[
The clinical manifestation varies according to the age, lesion size, and degree of compression in adjacent structures. Approximately 10%–30% of arachnoid cysts are located in the posterior fossa, with the most frequent sites being the cerebellar point angle, the supracollicular region, and the cerebellar vermis.[
Symptomatic arachnoid cysts in elderly patients are very rare.[
CASE REPORT
A 68-year-old male patient had weakness in the lower limbs, imbalance, and gait disturbance for 3 years, associated with frequent falls. The patient complained of paresthesia in the upper right limb and right hemiface for the prior 3 months.
Neurological examination revealed a weakness in the lower limbs (Grade 4/5), hyperreflexia in the lower limbs plus bilateral Achilles’ clonus, gait deviation to the right, and no findings in the cranial nerves or in the sensitivity test.
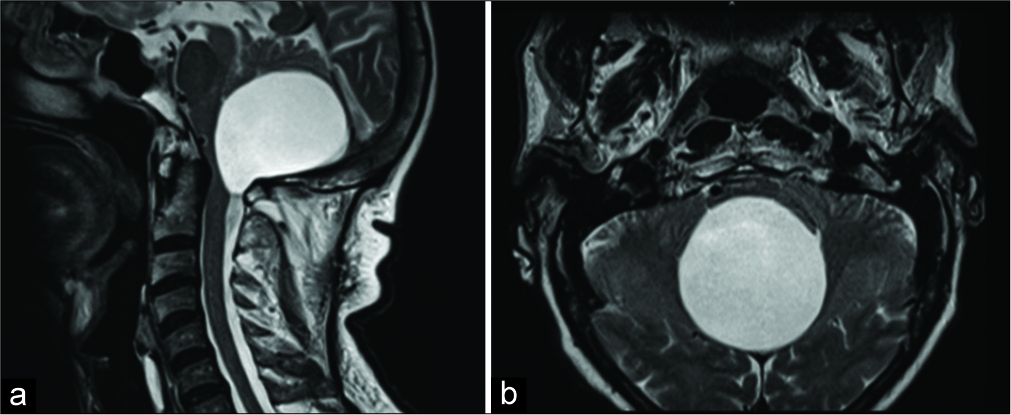
An magnetic resonance imaging (MRI) showed a massive cystic lesion measuring 6 cm×4.6 cm×5.2 cm (L×AP×T). The T1-weighted and T2-weighted signals were similar to the cerebrospinal fluid (CSF). The cyst was located in the foramen of Magendie. There was significant compression of the brainstem anteriorly, and the cerebellum was displaced superiorly [
Surgery
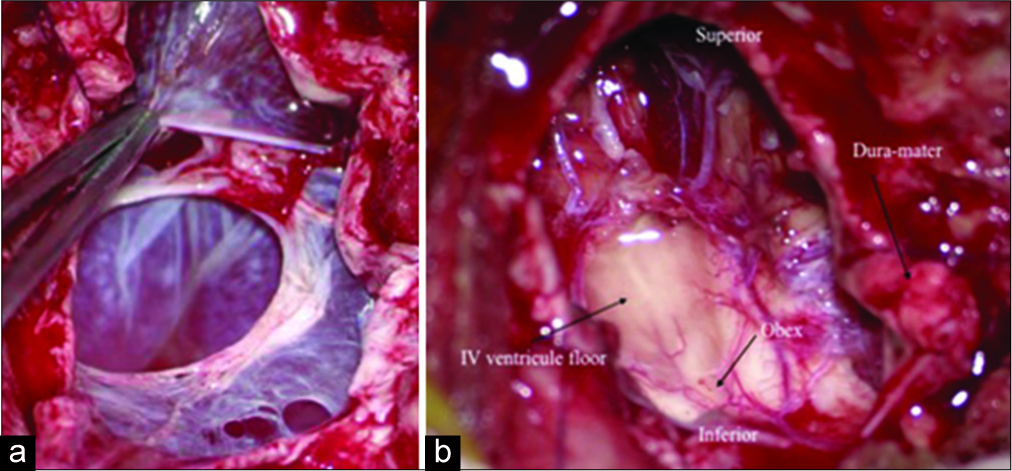
The patient was in the prone position after general anesthesia, midline incision, dissection of the muscle planes, exposure of the suboccipital bone, and posterior arch of C1. Suboccipital craniectomy, C1 laminectomy, and “Y” shaped durotomy were performed. The arachnoid cyst was exteriorizing through foramen of Magendie, displacing cerebellar hemisphere superiorly, cyst opening and removal of the cyst wall. The brainstem, obex, and spinal cord were observed at the end of the excision. The dura mater closure was done with autologous graft, then multiple layers closure [
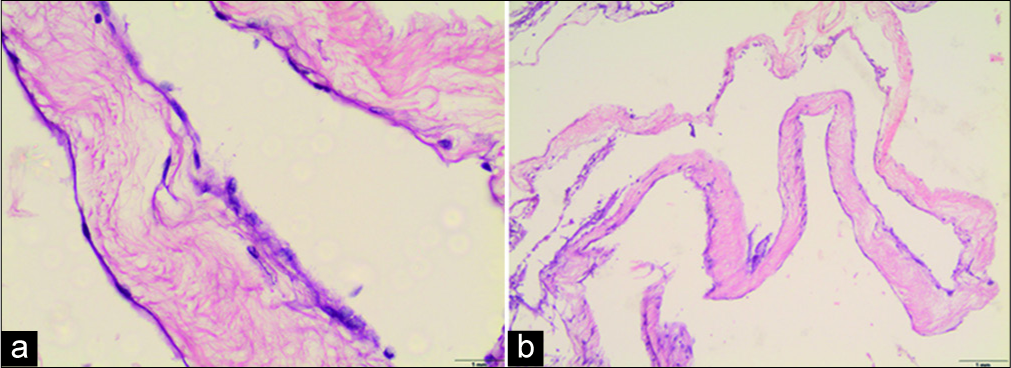
The anatomopathological examination with hematoxylin and eosin showed loose fibrous wall cyst lined by flattened meningothelial cells [
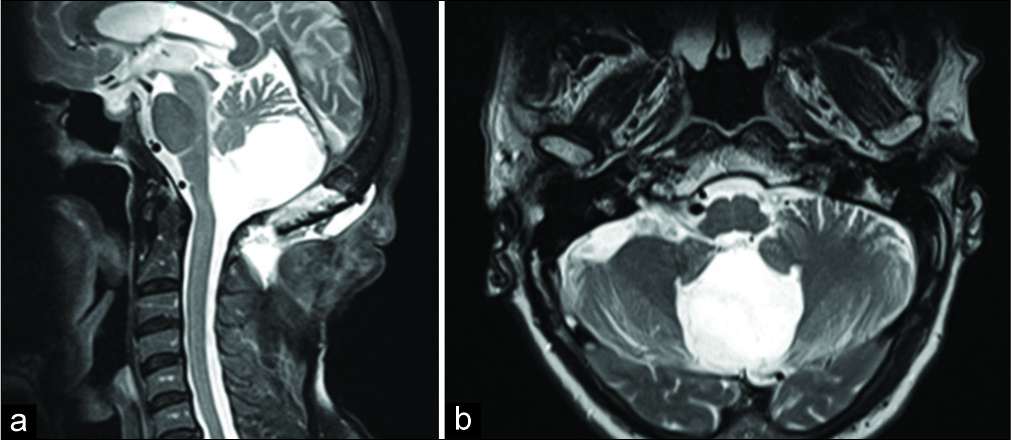
At the 6-month follow-up, the patient had recovered completely. Postoperative imaging showed a significant decrease in the compressive effect on the brainstem and cerebellum [
The patient signed a consent form authorizing the publication of this case report.
DISCUSSION
Cystic lesions of the posterior fossa include Dandy- Walker malformations, arachnoid cysts, Blake’s pouch cysts, mega cisterna magna, and epidermoid cysts. Epidermoid cysts and arachnoid cysts differ from the other malformations because they do not communicate with the ventricular system.[
Arachnoid cysts are benign leptomeningeal lesions that develop from the separation or duplication of the arachnoid membrane with subsequent CSF filling and are more common in males (3:1). Cysts may increase in size by valve mechanism, fluid secretion through the cyst wall, or by an osmotic gradient.[
In elderly patients with symptomatic arachnoid cysts, the clinical manifestations are similar to those with chronic subdural hematoma or normal pressure hydrocephalus, with the most common symptoms being headache, hemiparesis, gait alteration, and dementia. In general, the symptoms begin after minor trauma.[
Probably the mechanism of the arachnoid cyst became symptomatic in this case is due to traumatic event related by the patient, such as the frequent falls. Inflammatory and infectious conditions, which could also be an additional factor, were excluded with laboratory test and CSF with no abnormalities.
The treatment of choice for most cases is conservative. In cases of progressive neurological deficit or persistent symptoms, surgery is indicated. The objective is the collapse of the cyst and improvement of the clinical manifestations.[
In the first published case report of an arachnoid cyst in the foramen of Magendie in an elderly patient, the cerebellar symptoms were similar to those in our patient, including ataxia and gait disturbance, but in the present case, these symptoms caused the patient to fall repeatedly. In addition to the cerebellar symptoms, our patient presented with paresthesia in the right upper limb and right hemiface, which may have been caused by posterior brainstem compression. Although the cyst extension to spinal canal in our case, the MRI results were similar in both cases, in which there was no extension of the arachnoid cyst to the IV ventricle and the absence of hydrocephalus. As in our case, in the published case, the surgical approach was the same, and the outcome was excellent in both.[
CONCLUSION
This case report adds to the literature one more successful elderly patient treated by surgery for a symptomatic arachnoid cyst in the foramen of Magendie.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Clavel M, Taborga FG, Onzain I. Arachnoid cysts as a cause of dementia in the elderly. Acta Neurochir (Wien). 1985. 78: 28-32
2. Correa GG, Amaral LF, Vedolin LM. Neuroimaging of dandy-walker malformation: New concepts. Top Magn Reson Imaging. 2011. 22: 303-12
3. Cotes C, Bonfante E, Lazor J, Jadhav S, Caldas M, Swischuk L. Congenital basis of posterior fossa anomalies. Neuroradiol J. 2015. 28: 238-53
4. Filho SC, Marques JA, Albuquerque LA, Almeida JP, Santos FP. Cisto aracnoide intracraniano revisão de literatura. Arq Bras Neurocir. 2007. 26: 164-72
5. Hayashi Y, Kita D, Watanabe T, Yoshikawa A, Hamada J. Symptomatic foramen of magendie arachnoid cyst in an elderly patient. Surg Neurol Int. 2015. 6: 7-
6. Helland CA, Wester K. Arachnoid cysts in adults: Long-term follow-up of patients treated with internal shunts to the subdural compartment. Surg Neurol. 2006. 66: 56-61
7. Idris Z, Tan YC, Kandasamy R, Ghani RI, Abdullah JM. Transfrontal transaqueductal, transtrigonal, and suboccipital infratentorial supracerebellar endoscopic fenestration of posterior fossa arachnoid cysts: Three surgical cases. J Neurol Surg A Cent Eur Neurosurg. 2017. 78: 210-5
8. Lancon JA, Ellis AL. Giant posterior fossa arachnoid cyst. Pediatr Neurosurg. 2004. 40: 151-2
9. Panigrahi S, Mishra SS, Das S, Patra SK, Satpathy PC. Large intradural craniospinal arachnoid cyst: A case report and review of literature. J Craniovertebr Junction Spine. 2012. 3: 16-8
10. Pego-Reigosa R, Brañas-Fernández F, Martínez-Vázquez F, Cortés-Laiño JA. Craniospinal intradural arachnoid cyst. Arch Neurol. 2000. 57: 128-
11. Shekdar K. Posterior fossa malformations. Semin Ultrasound CT MR. 2011. 32: 228-41
12. Spansdahl T, Solheim O. Quality of life in adult patients with primary intracranial arachnoid cysts. Acta Neurochir (Wien). 2007. 149: 1025-32
13. Thinakara-Rajan T, Janjua A, Srinivasan V. Posterior fossa arachnoid cyst presenting with isolated sensorineural hearing loss. J Laryngol Otol. 2006. 120: 979-82
14. Wang Y, Wang F, Yu M, Wang W. Clinical and radiological outcomes of surgical treatment for symptomatic arachnoid cysts in adults. J Clin Neurosci. 2015. 22: 1456-61
15. Yamakawa H, Ohkuma A, Hattori T, Niikawa S, Kobayashi H. Primary intracranial arachnoid cyst in the elderly: A survey on 39 cases. Acta Neurochir (Wien). 1991. 113: 42-7

