

- Department of Neurosurgery, University of Cincinnati, Cincinnati, United States,
- Department of Neurosurgery, University of Baghdad, College of Medicine, Baghdad, Iraq,
- Department of Neurosurgery, University of Louisville, Kentucky, United States.
Correspondence Address:
Samer S. Hoz, Department of Neurosurgery, University of Cincinnati, Cincinnati, United States.
DOI:10.25259/SNI_784_2022
Copyright: © 2022 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Samer S. Hoz1, Paolo Palmisciano1, Hagar A. Algburi2, Mayur Sharma3, Mustafa Ismail2, Norberto Andaluz1. The crux of helix curvature: A potential surface landmark for the anterior border of the sigmoid sinus in minimally invasive presigmoid approaches. 23-Sep-2022;13:430
How to cite this URL: Samer S. Hoz1, Paolo Palmisciano1, Hagar A. Algburi2, Mayur Sharma3, Mustafa Ismail2, Norberto Andaluz1. The crux of helix curvature: A potential surface landmark for the anterior border of the sigmoid sinus in minimally invasive presigmoid approaches. 23-Sep-2022;13:430. Available from: https://surgicalneurologyint.com/surgicalint-articles/11888/
Date of Submission
27-Aug-2022
Date of Acceptance
02-Sep-2022
Date of Web Publication
23-Sep-2022
Abstract
Background: Surgical landmarks are widely used across all surgical specialties to assist surgeons in accurately estimating the deep anatomical structures. We describe the crus of helix curvature as a potential indicator for the anterior border of the sigmoid sinus (SS) in the setting of minimally invasive presigmoid approaches.
Methods: Anatomy investigations were performed on injected cadaveric heads to identify consistent surface surgical landmarks estimating the curse of the SS.
Results: Presigmoid mastoid was noted in the center of the skin incision in 100% of the specimens. The crus of helix curvature was superimposed on the anterior border of the SS on 6 sides (60%). On the other four sides, the curvature lays within 5 mm of the anterior SS border (40%).
Conclusion: For the minimally invasive presigmoid approaches, the “crus of helix curvature” can be used as a landmark for the anterior border of the SS, which can aid in the speed and safety of the procedure. The ease of use of this landmark makes it particularly convenient for physicians early in training.
Keywords: Crus helix, Ear anatomy, Presigmoid approach, Sigmoid sinus, Surgical landmarks
INTRODUCTION
The existence of landmarks can be dated back to the origin of surgical specialties. These landmarks have evolved to include surface, bony, and intraoperative markers that improve patient safety and outcome during surgical procedures. These surgical landmarks should estimate deep anatomical structures accurately considering interindividual anatomic variability.[
MATERIALS AND METHODS
This is a human cadaveric study performed at the Goodyear Lab-University of Cincinnati. Five injected cadaveric heads on both sides (a total of 10 slides) were used. The aim is to assess the crus of helix curvature as a consistent surface surgical landmark estimating the course of the anterior border of SS. The target anatomical structure was reached using minimally invasive presigmoid approaches.
RESULTS
The presigmoid mastoidectomy was observed in the exact center of the skin incision in 100% of the sample. The crus of helix curvature was superimposed on the anterior border of the SS on 6 sides (60%). On the other four sides, the curvature lays within 5 mm of the anterior SS border (40%).
DISCUSSION
Minimally invasive presigmoid approach
The posterolateral skull base approaches around the SS are routinely used for middle and posterior fossa pathologies. There is a profound disparity between the pre- and retro-sigmoid approaches regarding the available superficial anatomical landmarks. The localization of the posterior aspect of the SS and the transverse-sigmoid junction is extensively studied compared to the paucity of signs focusing on the presigmoid territory.[
The crus of the helix as a landmark
Based on our cadaveric investigations, we find a potential correlation between one of the internal folds of the pinna, namely, the crus of the helix and the anterior border of SS. For hearing-preserving presigmoid approaches, the “crus of helix curvature” can be used as a surface landmark to design the location of skin incision and then as an imaginary line on the mastoid bone to delineate the posterior boundary of the presigmoid approach [
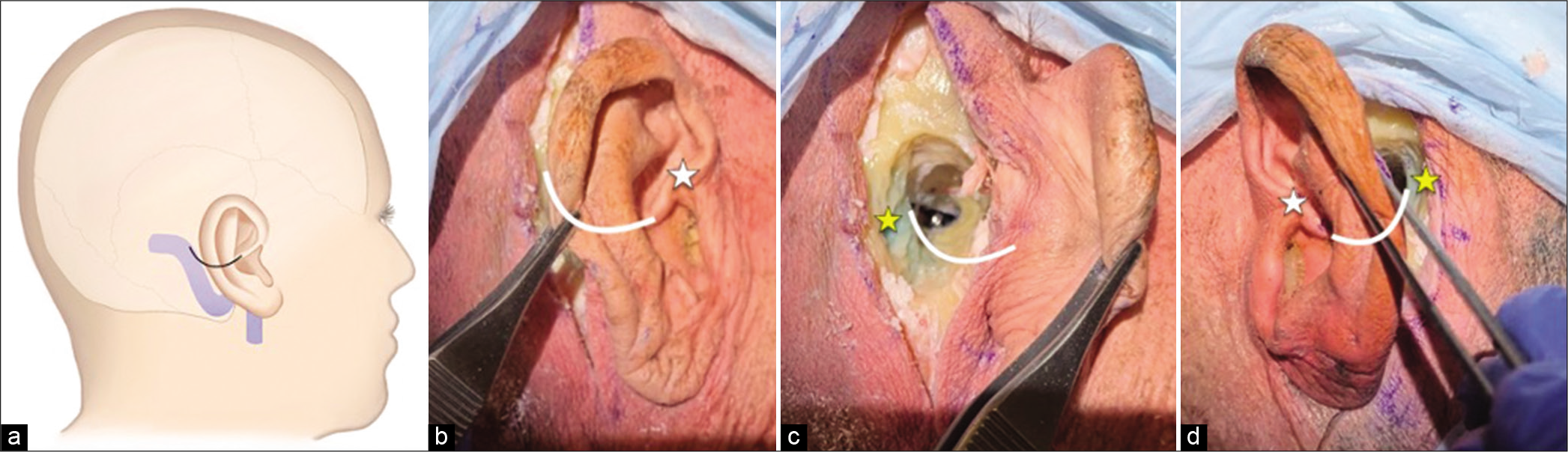
Figure 1:
The “Crus of Helix curvature” landmark for identification of the anterior border of the sigmoid sinus during a minimally invasive presigmoid approach. (a) Artistic depiction of the relevant anatomy. (b) description of the landmark in the pinna for the right-side approach on a cadaver. (c) Description of the landmark for the right-side presigmoid approach on the same cadaver as in (b). (d) The landmark applied to the right-side approach on another cadaver model. An imaginary line that follows the curvature of the crus posteriorly can trace the potential position of the anterior margin of the SS. The White Asterix denotes the crus, and the yellow Asterix denotes the sigmoid sinus, in (b), (c), and (d).
The crus of the helix is a fold of cartilage in the pinna located above the external auditory canal (EAC). The crus (the Latin for “foot”) represents the inferomedial end of the helix and correlates to the concha below and the tragus in front.[
The “crus of helix curvature” characterizes a simple and easy-touse landmark, and its proximity to the intended incision may prove a helpful surface landmark of the SS. In addition, the “crus of helix curvature” may aid in planning the center of the bony mastoid opening in both vertical and horizontal directions.
The surgical landmarks that utilize the local bony anatomy within the surgical exposure are likely to be more accurate compared to skin surface landmarks.[
We applied the “crus of helix curvature” landmark for a limited infratentorial presigmoid approach on five formalin-fixed, injected adult cadaveric heads on both sides, for a total of 10 sides. A straight incision over the retroauricular sulcus and along the anterior edge of the mastoid process was made. The incision is centered in the vertical plane on the posterior extension of the crus of the helix. Presigmoid mastoid was noted in the center of the skin incision in 100% of the specimens. The crus of helix curvature was superimposed on the anterior border of the SS on 6 sides (60%). On the other four sides, the curvature lays within 5 mm of the anterior SS border (40%). This was consistent with the simplicity and the applicability of this landmark for such approaches.
Limitations
The principal limitation of this surface landmark is related to its accuracy, which needs to be verified in the future studies. However, we believe that this is an easily applicable landmark with significant value during complex skull base procedures. In addition, the variability of this landmark in terms of age, gender, or racial characteristics can be validated in the future studies.[
CONCLUSION
For the minimally invasive (focused) presigmoid approaches, the “crus of helix curvature” can be used as a landmark for the anterior border of the SS, which can aid in the speed and safety of the procedure. The ease of use of this landmark makes it convenient for physicians early in training.
However, this sign should not be overrated. Further studies are needed to validate these findings in a larger cohort to increase the safety of complex lateral or posterior skull base approaches.
Declaration of patient consent
Patients’ consent not required as patients’ identities were not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Barut NR, Kale AN, Turan Suslu HK, Ozturk A, Bozbuga M, Sahinoglu K. Evaluation of the bony landmarks in transcondylar approach. Br J Neurosurg. 2009. 23: 276-81
2. Cascio Rizzo A, Paolucci M, Altavilla R, Brunelli N, Assenza F, Altamura C. Daith piercing in a case of chronic migraine: A possible vagal modulation. Front Neurol. 2017. 8: 624
3. Hall S, Gan YC. Anatomical localization of the transversesigmoid sinus junction: Comparison of existing techniques. Surg Neurol Int. 2019. 10: 186
4. Hayes CM. The ear: Excision and repair. Dermatol Clin. 1998. 16: 109-25
5. Jian ZH, Sheng MF, Li JY, Li Y, Weng ZJ, Chen G. Precise localization in craniotomy with a retrosigmoid keyhole approach: Microsurgical anatomy and clinical study. Front Surg. 2022. 9: 809098
6. Sop FY, D’Ercole M, Izzo A, Rapisarda A, Ioannoni E, Caricato A. The impact of neuronavigation on the surgical outcome of microvascular decompression for trigeminal neuralgia. World Neurosurg. 2021. 149: 80-5
7. Standring S. Evidence-based surface anatomy. Clin Anat. 2012. 25: 813-5

