

- Neurointervencionismo, Hospital El Cruce Néstor Kirchner, Florencio Varela, Buenos Aires, Argentina.
DOI:10.25259/SNI-44-2019
Copyright: © 2019 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Javier Goland, Gustavo Doroszuk. Transradial approach for endovascular diagnosis and treatment of ruptured cerebral aneurysms: A descriptive study. 10-May-2019;10:87
How to cite this URL: Javier Goland, Gustavo Doroszuk. Transradial approach for endovascular diagnosis and treatment of ruptured cerebral aneurysms: A descriptive study. 10-May-2019;10:87. Available from: http://surgicalneurologyint.com/surgicalint-articles/9343/
Date of Submission
08-Nov-2018
Date of Acceptance
23-Jan-2019
Date of Web Publication
10-May-2019
Abstract
Background: For cardiovascular procedures, the transradial approach has been documented to yield fewer complications than the femoral approach. It has become the approach of choice for diagnostic and therapeutic interventions involving the coronary arteries. However, few published data exist on using this approach for neuroendovascular procedures and we describe a series of ruptured cerebral aneurysms diagnosed and treated using the transradial approach.
Methods: All patients scheduled for cerebral angiography to diagnose and treat subarachnoid hemorrhages at our hospital from June 2016 to May 2018, by right radial artery access, were recruited and followed prospectively. The main outcomes of interest were the length of the procedure (in minutes), the success of treatment, and the incidence of postprocedural complications.
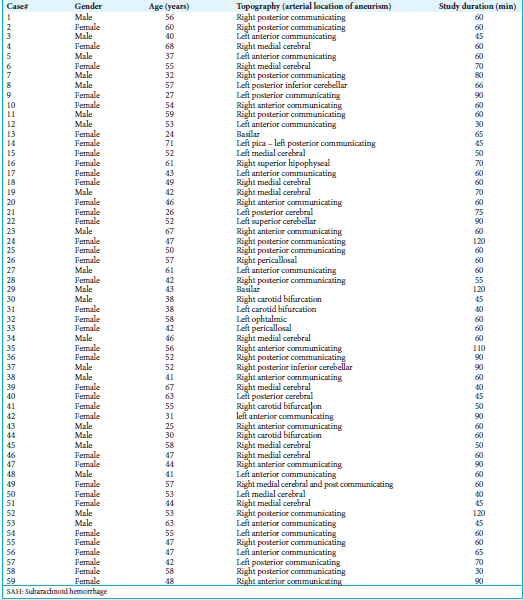
Results: Over the observation period, 59 patients (66% women, mean age = 48 years) with a combined 61 aneurysms treated were identified who met inclusion criteria. Of the 61 aneurysms treated, eight (13%) were within the posterior circulation (13%) and 53 (87%) the anterior circulation. Average procedural duration was 64.9 min. No occlusion or spasm of the radial artery was observed during any procedure. All patients had immediate pre- and post-embolization angiography, which revealed the guide catheter coming from the right subclavian artery. A radial pulse was evident after all interventions. All procedures were considered successful at treating the ruptured aneurysm, and no patient experienced a clinically significant complication related to the approach.
Conclusions: The transradial approach is a viable option for the diagnosis and endovascular treatment of acute cerebral aneurysms in different locations.
Keywords: Aneurysms, endovascular, subarachnoid hemorrhage, transradial approach
BACKGROUND
Endovascular coiling is considered a Class 1 Level B recommendation for ruptured cerebral aneurysms when the procedure is performed at experienced health centers.[
Complications associated with the femoral approach, whether used diagnostically or therapeutically and despite taking all the above-mentioned precautions, include hematomas at the puncture site (1.3%), retroperitoneal hematomas (0.4%), pseudoaneurysms (0.1%), and arterial dissections (0.3%), with higher incidences of these in anticoagulated and anti-aggregated patients. Low back pain, arteriovenous fistulae at the puncture site, femoral nerve injury, chronic ischemia of the lower limb, and thromboemboli are other complications that have been described.[
The radial approach for coronary angiography was initially described in 1989.[
In addition to its use for coronary procedures, there have been published series describing diagnostic transradial cerebral angiographies,[
METHODS
At our institution, between June 1, 2016, and May 31, 2018, a radial access was employed for 61 aneurysms that were evaluated and treated in 59 patients with subarachnoid hemorrhage. All patients with incidental aneurysms, aneurysms already diagnosed by previous studies, and fusiform aneurysms ineligible for endovascular coiling were excluded from this series. Patient information was extracted from the hospital’s medical record database. All the procedures were performed by either one or both of the current authors, jointly, at Hospital El Cruce in Buenos Aires, Argentina.
All patients with right radial pulse palpable underwent right radial arteriopuncture.[
All diagnostic studies to assess the supra-aortic vessels were performed with a Simmons Type II catheter (Merit Medical Systems, Utah, USA) on a 0.035-inch-thick hydrophilic guidewire.
After the diagnostic study, a 260 cm-long hydrophilic guidewire was passed either through the external carotid artery on the side corresponding to the aneurysm or through the left vertebral artery [
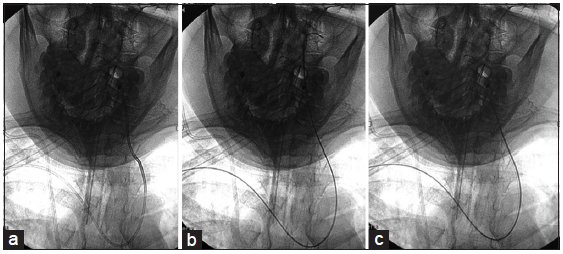
Once coiling was completed, the microcatheter was removed and angiographic acquisition was performed to demonstrate the guide catheter’s trajectory from the right subclavian artery to the cervical vessel. Next, the guide catheter and sheath were removed, following irrigation, through the lateral route, with 5 cc of nitroglycerin (200 µg/mL). Heparin was not reversed, and a direct compression was left over the puncture site after study completion for 1 h.[
RESULTS
Over a 2-year span, between June 2016 and May 2018, 59 patients with cerebral aneurysms at different locations were treated by endovascular coiling through transradial access. In two of these 59 patients, two separate aneurysms were treated, since it was impossible to determine which one had caused the patient’s subarachnoid hemorrhage, resulting in a total of 61 aneurysms treated. Of the 59 patients, 39 (66%) were women, and the average age was 48 years. Of the 61 aneurysms treated, eight (13%) were within the posterior circulation (13%), while the remaining 53 (87%) arose within the anterior circulation. The average duration of the procedure was 64.9 min. No occlusion or spasm of the radial artery was observed during any procedure. All patients had immediate postembolization angiography, which revealed the aneurysms occluded with coils and the guide catheter within the right subclavian artery [
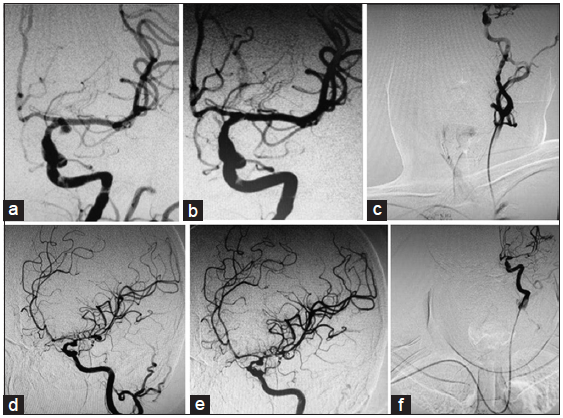
Figure 2
Diagnostic and post therapeutic control angiographic images. (a) Aneurysm located at the left carotid artery bifurcation, (b) Final post therapeutic control, (c) Final control image showing guide catheter within the subclavian artery, (d) Aneurysm located at the left cerebral media artery bifurcation, (e) Final post therapeutic control, (f) Final control image showing guide catheter within the subclavian artery.
DISCUSSION
In this paper, we describe 61 endovascular coiling procedures performed in 59 subarachnoid hemorrhage patients to treat cerebral aneurysms at a variety of different locations. All 61 aneurysms were accessed by introducing the catheter through the radial artery, an approach that was highly efficient and performed without complications. To date, ours is the largest published series of ruptured cerebral aneurysms embolized by endovascular coiling through the radial artery. We resolved all the cases of this series with coiling technique, but it could have been possible to perform double catheter or remodeling balloon techniques if it would have been necessary.
Radial access is used for angiography and coronary angioplasty procedures worldwide. Some series have been reported on cerebral angiographies performed by transradial access, but the use of this approach to evaluate supra-aortic vessels and to provide endovascular treatment of cerebral aneurysms has, thus far, failed to achieve the same level of acceptance afforded coronary interventions.
Two empirically supported reasons for adopting the radial approach are patient preference and the lower number of complications that occur at the puncture site, relative to the femoral approach.[
CONCLUSIONS
The right transradial approach is an option for the endovascular diagnosis and treatment of cerebral aneurysms of different locations that require a 6Fr or smaller catheter’s size. We observed no topographic limitations or arterial injuries treating aneurysms by this route. This is the largest series of ruptured cerebral aneurysms diagnosed and treated endovascularly through the right radial artery up to date.
References
1. Agostoni P, Biondi-Zoccai GG, de Benedictis ML, Rigattieri S, Turri M, Anselmi M. Radial versus femoral approach for percutaneous coronary diagnostic and interventional procedures; systematic overview and meta-analysis of randomized trials. J Am Coll Cardiol. 2004. 44: 349-56
2. Bakhshi F, Namjou Z, Andishmand A, Panabadi A, Bagherinasab M, Sarebanhassanabadi M. Effect of positioning on patient outcomes after coronary angiography: A single-blind randomized controlled trial. J Nurs Res. 2014. 22: 45-50
3. Bendok BR, Przybylo JH, Parkinson R, Hu Y, Awad IA, Batjer HH. Neuroendovascular interventions for intracranial posterior circulation disease via the transradial approach: Technical case report. Neurosurgery. 2005. 56: E626-
4. Benit E, Vranckx P, Jaspers L, Jackmaert R, Poelmans C, Coninx R. Frequency of a positive modified Allen’s test in 1,000 consecutive patients undergoing cardiac catheterization. Cathet Cardiovasc Diagn. 1996. 38: 352-4
5. Campeau L. Percutaneous radial artery approach for coronary angiography. Cathet Cardiovasc Diagn. 1989. 16: 3-7
6. Connolly ES, Rabinstein AA, Carhuapoma JR, Derdeyn CP, Dion J, Higashida RT. Guidelines for the management of aneurysmal subarachnoid hemorrhage: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2012. 43: 1711-37
7. Cooper CJ, El-Shiekh RA, Cohen DJ, Blaesing L, Burket MW, Basu A. Effect of transradial access on quality of life and cost of cardiac catheterization: A randomized comparison. Am Heart J. 1999. 138: 430-6
8. Cox N. Managing the femoral artery in coronary angiography. Heart Lung Circ. 2008. 17: S65-9
9. Din JN, Murphy A, Chu K, Forman P, Mildenberger RD, Fretz EB. Radial artery pseudoaneurysms after transradial cardiac catheterisation. Vasa. 2016. 45: 229-32
10. Eichhöfer J, Horlick E, Ivanov J, Seidelin PH, Ross JR, Ing D. Decreased complication rates using the transradial compared to the transfemoral approach in percutaneous coronary intervention in the era of routine stenting and glycoprotein platelet IIb/IIIa inhibitor use: A large single-center experience. Am Heart J. 2008. 156: 864-70
11. Esente P, Giambartolomei A, Simons AJ, Levy C, Caputo RP. Overcoming vascular anatomic challenges to cardiac catheterization by the radial artery approach: Specific techniques to improve success. Catheter Cardiovasc Interv. 2002. 56: 207-11
12. Fessler RD, Wakhloo AK, Lanzino G, Guterman LR, Hopkins LN. Transradial approach for vertebral artery stenting: Technical case report. Neurosurgery. 2000. 46: 1524-7
13. Goland J, Doroszuk GF, Garbugino SL, Ypa MP. Transradial approach to treating endovascular cerebral aneurysms: Case series and technical note. Surg Neurol Int. 2017. 8: 73-
14. Hildick-Smith DJ, Lowe MD, Walsh JT, Ludman PF, Stephens NG, Schofield PM. Coronary angiography from the radial artery experience, complications and limitations. Int J Cardiol. 1998. 64: 231-9
15. Jo KW, Park SM, Kim SD, Kim SR, Baik MW, Kim YW. Is transradial cerebral angiography feasible and safe? A Single center’s experience. J Korean Neurosurg Soc. 2010. 47: 332-7
16. Jolly SS, Yusuf S, Cairns J, Niemelä K, Xavier D, Widimsky P. Radial versus femoral access for coronary angiography and intervention in patients with acute coronary syndromes (RIVAL): A randomised, parallel group, multicentre trial. Lancet. 2011. 377: 1409-20
17. Kiemeneij F, Laarman GJ, de Melker E. Transradial artery coronary angioplasty. Am Heart J. 1995. 129: 1-7
18. Kim JH, Park YS, Chung CG, Park KS, Chung DJ, Kim HJ. Feasibility and utility of transradial cerebral angiography: Experience during the learning period. Korean J Radiol. 2006. 7: 7-13
19. Lawson MF, Velat GJ, Fargen KM, Hoh BL, Mocco J. Direct radial artery access with the 070 neuron guide catheter for aneurysm coiling: A novel application of the neuron catheter for cerebral interventions. Neurosurgery. 2012. 71: onsE329-34
20. Lee DH, Ahn JH, Jeong SS, Eo KS, Park MS. Routine transradial access for conventional cerebral angiography: A single operator’s experience of its feasibility and safety. Br J Radiol. 2004. 77: 831-8
21. Lee MS, Applegate B, Rao SV, Kirtane AJ, Seto A, Stone GW. Minimizing femoral artery access complications during percutaneous coronary intervention: A comprehensive review. Catheter Cardiovasc Interv. 2014. 84: 62-9
22. Levy EI, Boulos AS, Fessler RD, Bendok BR, Ringer AJ, Kim SH. Transradial cerebral angiography: An alternative route. Neurosurgery. 2002. 51: 335-40
23. Louvard Y, Krol M, Pezzano M, Sheers L, Piechaud JF, Marien C. Feasibility of routine transradial coronary angiography: A single operator’s experience. J Invasive Cardiol. 1999. 11: 543-8
24. Ludman PF, Stephens NG, Harcombe A, Lowe MD, Shapiro LM, Schofield PM. Radial versus femoral approach for diagnostic coronary angiography in stable angina pectoris. Am J Cardiol. 1997. 79: 1239-41
25. Maniotis C, Koutouzis M, Andreou C, Lazaris E, Tsiafoutis I, Zografos T. Transradial approach for cardiac catheterization in patients with negative Allen’s test. J Invasive Cardiol. 2015. 27: 416-20
26. Matsumoto Y, Hongo K, Toriyama T, Nagashima H, Kobayashi S. Transradial approach for diagnostic selective cerebral angiography: Results of a consecutive series of 166 cases. AJNR Am J Neuroradiol. 2001. 22: 704-8
27. Nohara AM, Kallmes DF. Transradial cerebral angiography: Technique and outcomes. AJNR Am J Neuroradiol. 2003. 24: 1247-50
28. Ricci MA, Trevisani GT, Pilcher DB. Vascular complications of cardiac catheterization. Am J Surg. 1994. 167: 375-8
29. Schönholz C, Nanda A, Rodríguez J, Shaya M, D’Agostino H. Transradial approach to coil embolization of an intracranial aneurysm. J Endovasc Ther. 2004. 11: 411-3
30. Valgimigli M, Campo G, Penzo C, Tebaldi M, Biscaglia S, Ferrari R. Transradial coronary catheterization and intervention across the whole spectrum of Allen test results. J Am Coll Cardiol. 2014. 63: 1833-41
31. Wu CJ, Hung WC, Chen SM, Yang CH, Chen CJ, Cheng CI. Feasibility and safety of transradial artery approach for selective cerebral angiography. Catheter Cardiovasc Interv. 2005. 66: 21-6

