

- Department of Neurosurgery, Neurosurgical Clinic, AOUP “Paolo Giaccone”, Post Graduate Residency Program in Neurosurgery, Italy.
- Department of Experimental Biomedicine and Clinical Neurosciences, School of Medicine, Palermo, Italy.
- Department of Neuroscience, Division of Neurosurgery, Reproductive and Odontostomatological Sciences, Napoli, Italy.
- Department of Neurosurgery, Villa Sofia Hospital, Palermo, Italy.
- Department of Neurosurgery, ARNAS Garibaldi, Catania, Italy.
Correspondence Address:
Lara Brunasso
Department of Experimental Biomedicine and Clinical Neurosciences, School of Medicine, Palermo, Italy.
Department of Neurosurgery, ARNAS Garibaldi, Catania, Italy.
DOI:10.25259/SNI_407_2020
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Luigi Basile1,2, Lara Brunasso1,2, Rosa Maria Gerardi3, Rosario Maugeri1,2, Domenico Gerardo Iacopino1,2, Carlo Gulì1,2, Maria Angela Pino1,2, Silvana Tumbiolo4, Giovanni Federico Nicoletti5, Francesca Graziano2,5. Traumatic lumbar disc extrusion mimicking spinal epidural hematoma: Case report and literature review. 21-Oct-2020;11:348
How to cite this URL: Luigi Basile1,2, Lara Brunasso1,2, Rosa Maria Gerardi3, Rosario Maugeri1,2, Domenico Gerardo Iacopino1,2, Carlo Gulì1,2, Maria Angela Pino1,2, Silvana Tumbiolo4, Giovanni Federico Nicoletti5, Francesca Graziano2,5. Traumatic lumbar disc extrusion mimicking spinal epidural hematoma: Case report and literature review. 21-Oct-2020;11:348. Available from: https://surgicalneurologyint.com/surgicalint-articles/10347/
Date of Submission
05-Jul-2020
Date of Acceptance
29-Sep-2020
Date of Web Publication
21-Oct-2020
Abstract
Background: Because the neurological presentation of spinal epidural hematomas (SEH) is often not specific, they may be misdiagnosed as acute lumbar disk herniations. Here, we present a case in which a traumatic disc extrusion mimicked an epidural hematoma and reviewed the appropriate literature.
Case Description: A 27-year-old male sustained a high-energy fall. The lumbar MRI scan showed a L4-S1 ventral medium/high signal intensity mass on the T1- and high signal intensity lesion on T2-weighted images; the original diagnosis was spinal epidural hematoma. However, at surgery, consisting of a left L4 and L5 hemilaminectomy with L4-L5 and L5-S1 laminotomy, an extruded lumbar disc was encountered at the L4-L5 level and removed; no additional pathology or SEH was found at either level.
Conclusion: On MR, SEH may mimic acute lumbar disk herniations. Depending on the clinical symptoms/signs, surgical intervention will both correctly confirm the diagnosis and relieve neural compression.
Keywords: Extruded disc herniation, Magnetic resonance imaging, Spinal epidural hematoma, Traumatic disc extrusion
INTRODUCTION
Trauma, coagulation disorders, spine surgery, and/or lumbar spinal punctures/epidural injections are the major factors predisposing patients to developing spinal epidural hematomas (SEH).[
CASE REPORT
A 27-year-old man presented with a high-energy fall who presented with a severe paraparesis and bilateral hypoanesthesia in both lower extremities.
MR findings
The spine lumbosacral MRI scan showed a bilateral, longitudinally oriented mass in the anterior epidural space between the posterior walls of L4 down to S1. It markedly compressed both the cauda equina and anterior L5 and S1 nerve roots [
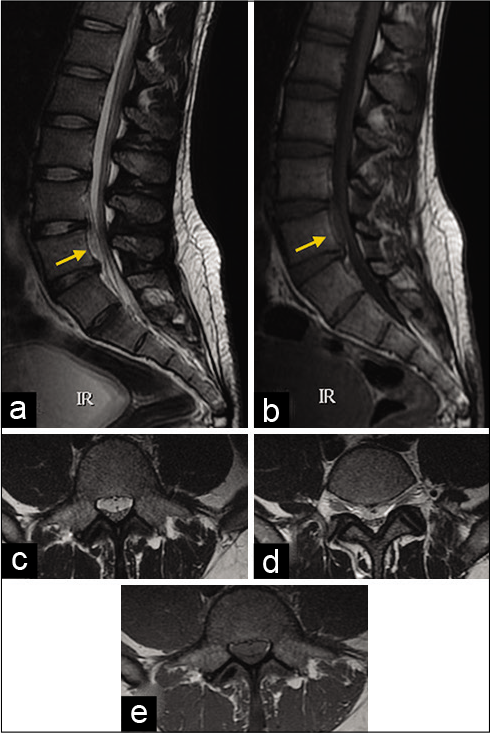
Figure 1:
Sagittal T2-weighted (a) and sagittal T1-weighted (b) MRI showed a longitudinally oriented mass-like lesion in the anterior epidural space (arrow). The mass presented with high signal intensity on T2-weighted images and medium/high signal intensity on T1-weighted images. Axial T2-weighted (c and d) and axial T1-weighted (e) MRI showed that the dural sac was compressed by the ventral mass.
Surgery
Through a left L4 hemilaminectomy and L4-L5 foraminotomy, a large disc fragment was found that had migrated inferiorly below both L5 roots. The disk fragment was removed, and a L4-L5 microsurgical discectomy was completed; there was no epidural hematoma. The same procedure was performed at L5-S1 where the posterior longitudinal ligament appeared similarly disrupted but there was no additional disc fragment or epidural hematoma. Postoperatively, the patient exhibited slight recovery of lower limbs motor and sensor function, improvement being noted predominantly on the right side. The postoperative lumbar MRI confirmed adequate canal decompression without any further lesions being identified [
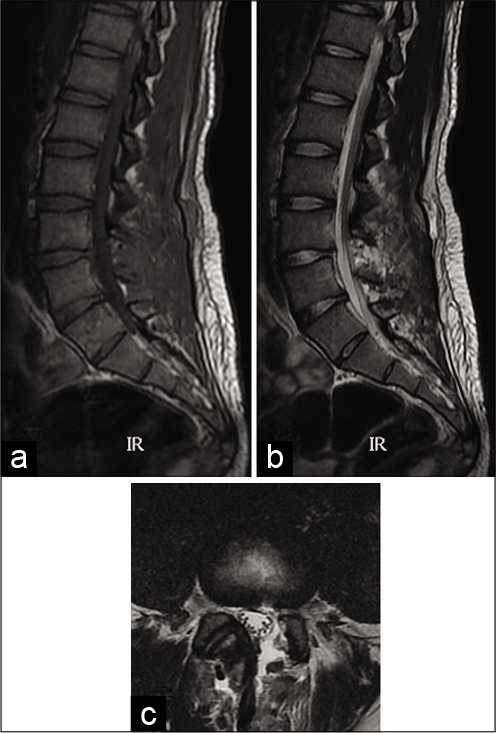
Figure 2:
Sagittal T1-weighted and T2-weighted (a and b) MRI showed the complete removal of the herniated lumbar disk and no residual signs of the preoperative longitudinally oriented mass-like lesion in the anterior epidural space. Axial T2-weighted (c) MRI showed neither dural sac nor nerve compression.
DISCUSSION AND LITERATURE REVIEW
MRI findings are the most reliable for diagnosing traumatic disc herniations. Traumatic disc herniation is most evident on T2-weighted images that usually have low signal intensity on T2-weighted and a high signal intensity on T1-weighted images. Morphological changes to the disc resulting in signal alterations on MRI depend on the severity of the trauma. T2-weighted MRI can also reveal hyperintense cord contusions from the compression and stripping of the posterior longitudinal ligament.[
The MRI findings of acute SEH have been described differently showing isointense or hypointense signals on T1-weighted images (whereas subacute and chronic hemorrhages have a hyperintense appearance on T1-weighted images) and heterogeneity or mixed high/low signals on T2-weighted studies. Notably, traumatic disc herniations, unlike epidural hematomas, usually regress in size over time.[
In our patient, the herniated mass showed a medium/high SI on the T1-weighted MRIs and high SI on T2-weighted MRIs [
We identified four similar reports of traumatic lumbar disk herniation mimicking epidural hematomas and we reported a table with comparable cases [

In spine trauma, conservative management is generally accepted as a first-line of management in cases without neurologic injury or gross instability. Typically, surgical intervention is required as the presence of neurological deficits.
CONCLUSION
On MR, SEH may mimic acute lumbar disk herniations. Depending on the clinical symptoms/signs, surgical intervention will both correctly confirm the diagnosis and relieve neural compression.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Bennett DL, George MJ, Ohashi K, El-Khoury GY, Lucas JJ, Peterson MC. Acute traumatic spinal epidural hematoma: Imaging and neurologic outcome. Emerg Radiol. 2005. 11: 136-44
2. Brinckmann P. Injury of the annulus fibrosus and disc protrusions. An in vitro investigation on human lumbar discs. Spine (Phila Pa 1976). 1986. 11: 149-53
3. Domenicucci M, Mancarella C, Santoro G, Dugoni DE, Ramieri A, Arezzo MF. Spinal epidural hematomas: Personal experience and literature review of more than 1000 cases. J Neurosurg Spine. 2017. 27: 198-208
4. Dorsay TA, Helms CA. MR imaging of epidural hematoma in the lumbar spine. Skeletal Radiol. 2002. 31: 677-85
5. Figueroa J, DeVine JG. Spontaneous spinal epidural hematoma: Literature review. J Spine Surg. 2017. 3: 58-63
6. Giri PJ, Sharma MS, Jaiswal AK, Behari S, Jain VK. Extruded lumbar disc associated with epidural hematoma. Case report. J Neurosurg. 2006. 104: 282-4
7. Jain N, Crouser N, Yu E. Lumbar intervertebral disc herniation masquerading as an epidural hematoma: A case report and review of the literature. JBJS Case Connect. 2018. 8: e59
8. Kil JS, Park JT. Posterior epidural herniation of a lumbar disk fragment at L2-3 that mimicked an epidural hematoma. Korean J Spine. 2017. 14: 115-7
9. Kim JH, Kim SH, Lee SK, Moon BJ, Lee JK. Traumatic lumbar disc herniation mimicking epidural hematoma: A case report and literature review. Medicine (Baltimore). 2019. 98: e15438
10. Kreppel D, Antoniadis G, Seeling W. Spinal hematoma: A literature survey with meta-analysis of 613 patients. Neurosurg Rev. 2003. 26: 1-49
11. Sander AL, Laurer H, Lehnert T, El Saman A, Eichler K, Vogl TJ. A clinically useful classification of traumatic intervertebral disk lesions. AJR Am J Roentgenol. 2013. 200: 618-23
12. Sklar EM, Post JM, Falcone S. MRI of acute spinal epidural hematomas. J Comput Assist Tomogr. 1999. 23: 238-43
13. Song KJ, Lee KB, Kim DY, Lee SY. A traumatic disc herniation mimicking an epidural hematoma in a young adult-a case report. Neurosurg Q. 2012. 22: 81-3
14. Watanabe N, Ogura T, Kimori K, Hase H, Hirasawa Y. Epidural hematoma of the lumbar spine, simulating extruded lumbar disk herniation: Clinical, discographic, and enhanced magnetic resonance imaging features. A case report. Spine (Phila Pa 1976). 1997. 22: 105-9

