

- Department of Neurosurgery, Soonchunhyang University Cheonan Hospital, Cheonan, Republic of Korea,
- Department of Otorhinolaryngology, Soonchunhyang University Cheonan Hospital, Cheonan, Republic of Korea.
Correspondence Address:
Hyuk-Jin Oh, Department of Neurosurgery, Soonchunhyang University Cheonan Hospital, Cheonan, Republic of Korea.
DOI:10.25259/SNI_61_2022
Copyright: © 2022 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Beom Mo Kang1, Hyuk-Jin Oh1, Kwang-Hui Ryu2, Jae-Min Ahn1. Treatment of pituitary adenoma with spontaneous cerebrospinal rhinorrhea using nasoseptal flap, two case reports. 23-Jun-2022;13:262
How to cite this URL: Beom Mo Kang1, Hyuk-Jin Oh1, Kwang-Hui Ryu2, Jae-Min Ahn1. Treatment of pituitary adenoma with spontaneous cerebrospinal rhinorrhea using nasoseptal flap, two case reports. 23-Jun-2022;13:262. Available from: https://surgicalneurologyint.com/surgicalint-articles/11669/
Date of Submission
15-Jan-2022
Date of Acceptance
21-May-2022
Date of Web Publication
23-Jun-2022
Abstract
Background: Postoperative cerebrospinal fluid (CSF) leakages are well documented, but pituitary adenoma with spontaneous CSF rhinorrhea as the initial symptoms are extremely rare. The objective of this study is to report two rare cases of pituitary adenoma with spontaneous CSF rhinorrhea successfully operated by endoscopic transsphenoidal approach with vascularized nasoseptal flap (NSF).
Case Description: A 70-year-old woman presented with a 6-month history of watery rhinorrhea and posterior nasal drip that worsened when her head leaning forward. Sella magnetic resonance image (MRI) demonstrated pituitary macroadenoma (3.4 × 2.7 cm) invading cavernous sinus, clivus, and sphenoid sinus. A 47-year-old woman presented with a 10-month history of watery rhinorrhea and posterior nasal drip. Sella MRI demonstrated pituitary macroadenoma (6.3 × 4.6 cm) invading cavernous sinus, clivus, sphenoid sinus, and middle fossa. Both patients underwent endoscopic endonasal transsphenoidal operation and skull base reconstruction with vascularized NSF. The postoperative clinical course was uneventful and CSF rhinorrhea disappeared completely.
Conclusion: Pituitary adenoma should be suspected if there is a watery CSF rhinorrhea that occurs without a history of trauma or nasal disease. In addition, effective treatment can be performed using NSF, a technique for endoscopic skull base reconstruction.
Keywords: Cerebrospinal fluid leak, Cerebrospinal fluid rhinorrhea, Endoscopy, Pituitary neoplasm, Skull base
INTRODUCTION
The spontaneous cerebrospinal fluid (CSF) rhinorrhea has an extremely rare clinical condition and is difficult to diagnose to the physician. It is usually caused by trauma, but rarely occurs with congenital defects, associated complications after transsphenoidal surgery, or pituitary adenoma shrinkage after during treatment such as bromocriptine.[
CASE PRESENTATION
This study was approved by Institutional Review Board of Soonchunhyang University Cheonan Hospital.
Case 1
A 70-year-old woman presented with a 6-month history of watery rhinorrhea, which was worsened when she lowered her head. She had never had a head trauma or otology-related surgery and had no special medical history other than poorly controlled diabetes. Neurological examinations showed alert consciousness and no visual impairment was observed. Watery rhinorrhea was a clear liquid with no fever or neck stiffness observed. General blood test and CSF biochemical analysis revealed that they were within the normal range without evidence of infection. Ostiomeatal unit computed tomography (CT) scan showed fluid collection in sphenoid sinus with bony defects in skull base and pituitary fossa. Magnetic resonance image (MRI) demonstrated large mass of invading pituitary fossa, sphenoid sinus, ethmoid sinus, cavernous sinus, and clivus [
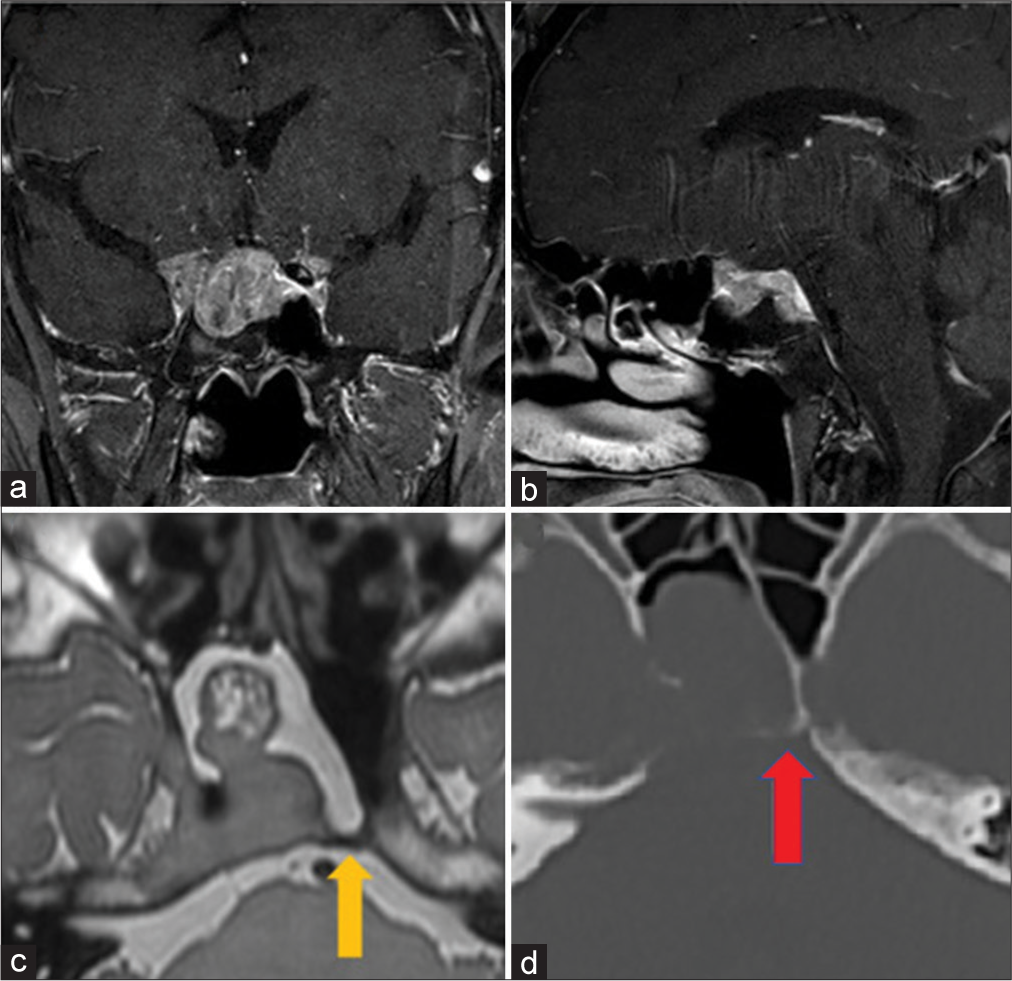
Figure 1:
Preoperative magnetic resonance image in Case 1. (a) Gadolinium-enhanced coronal image was obtained. (b) Gadolinium-enhanced sagittal image was obtained. (c) Vista axial image was obtained. Yellow arrow indicates the thinnest part of the bone and it points to the most likely part as a suspected cerebrospinal fluid leak. (Yellow arrow) (d) Cranial computed tomography axial image showed sphenoid bony defect and fluid collection at the sphenoid sinus (Red arrow).
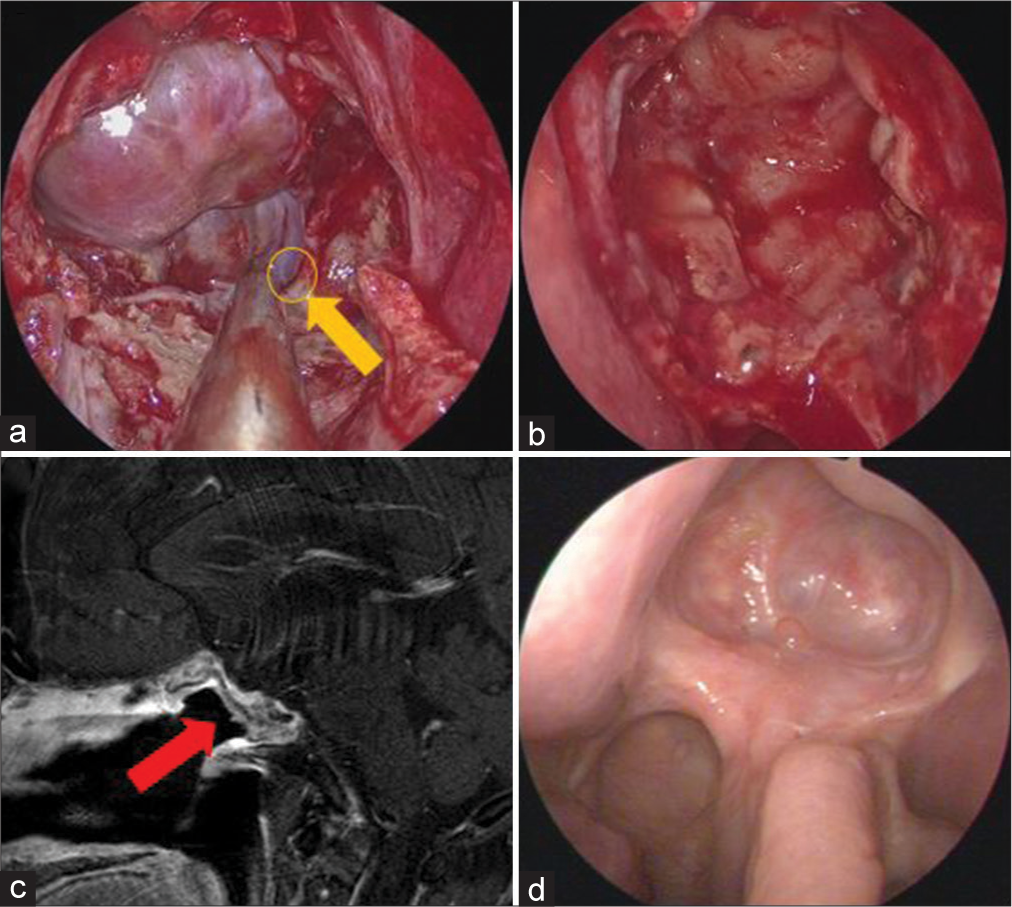
Figure 2:
Intraoperative endoscope image and follow-up sinus endoscopy image in Case 1. (a) After exposing sphenoid sinus, cerebrospinal fluid leak point was identified on posterior wall of sphenoid sinus and clivus. (Yellow arrow and Yellow circle) (b) After subtotal removal of the tumor, defect was packed with fat tissue, fibrin glue, and tensor fascia lata. And the cavity was entirely covered by vascularized nasoseptal flap. (c) Nasoseptal flap was stably observed on postoperative T1-weighted sagittal magnetic resonance image. (Red arrow). (d) Sinus endoscopy image was obtained after 8 months after surgery. No defect was identified.
After removal of mass, defect was packed with fat tissue and fibrin glue. The vascularized septal flap using the right nasoseptal mucosa was covered over the entire defect. Lumbar drain for CSF drainage was maintained after surgery and was removed on the 10th postoperative day. There was no CSF rhinorrhea postoperatively. Histopathology was confirmed as a pituitary adenoma. Ki-67 was 1% which demonstrates that invasiveness of pituitary adenoma was low and no other specific findings were observed. No CSF rhinorrhea was observed 18 months after surgery.
Case 2
A 47-year-old woman presented with a huge mass lesion at skull base on a CT performed for a health screening. She had never had a head trauma or otology-related surgery and had a well-controlled hypertension with single medication. She had a little watery rhinorrhea when she lowered her head from 10-month ago, but she thought that it was rhinitis and did not go to hospital. Neurological examinations showed alert consciousness and no visual impairment was observed. Watery rhinorrhea was a clear liquid with no fever or neck stiffness observed. General blood test and CSF biochemical analysis revealed that they were within the normal range without evidence of infection. Brain CT showed large mass in the mid-cranial fossa, sella, and suprasellar region with bony destructions. Sella MRI demonstrated large mass of invading middle cranial fossa, pituitary fossa, sphenoid sinus, ethmoid sinus, cavernous sinus, and clivus [
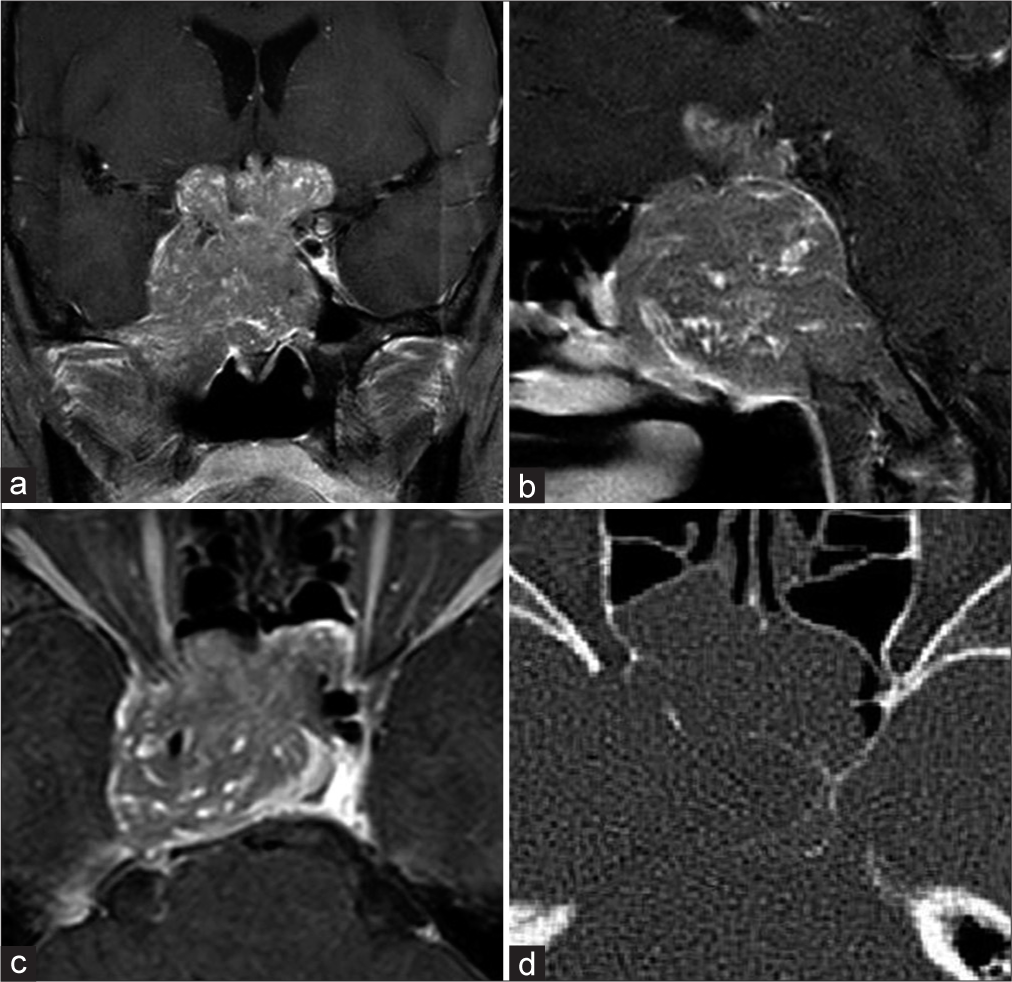
Figure 3:
Preoperative magnetic resonance image in Case 2. (a) Gadolinium-enhanced coronal image was obtained. (b) Gadolinium-enhanced sagittal image was obtained. (c) Gadolinium-enhanced axial image was obtained. (d) Cranial computed tomography axial image showed bony destruction of sphenoidal bone due to brain tumor and fluid collection at the sphenoid sinus.
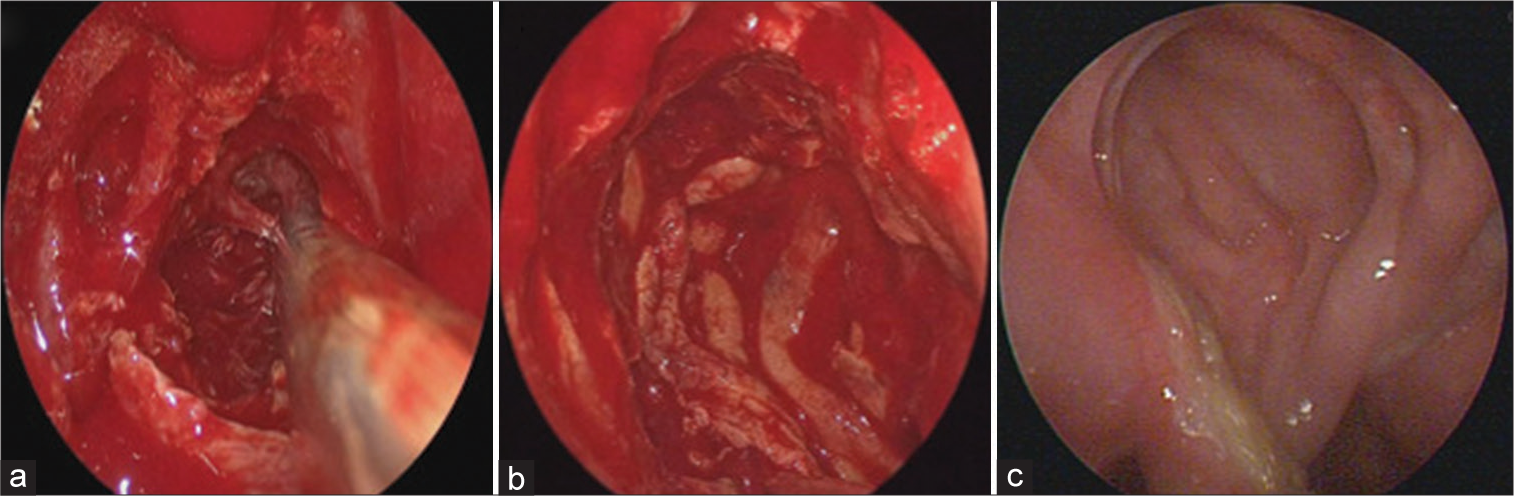
Figure 4:
Intraoperative endoscope image and follow-up sinus endoscopy image in Case 2. (a) Clivus was destroyed due to tumor invasion. After exposing the right side ethmoid bone and upper tuberculum sellae, tumor was observed (b) After partial resection of the tumor, defect was packed with fat tissue, fibrin glue, and tensor fascia lata. And the cavity was entirely covered by vascularized nasoseptal flap (c) Sinus endoscopy image was obtained after 4 months after surgery. No defect was identified.
After removal of mass, defect was packed with fat tissue and fibrin glue. The vascularized septal flap using the nasoseptal mucosa was covered over the entire defect. Histopathology was confirmed as a pituitary adenoma and ki-67 was 1% and no other specific findings were observed. Lumbar drain for CSF drainage was maintained after surgery. Lumbar drain for CSF drainage was maintained after surgery and was removed on the ninth postoperative. There was no CSF rhinorrhea postoperatively and no CSF rhinorrhea was observed 18 months after surgery.
DISCUSSION
The spontaneous CSF is usually caused by trauma, complications after transsphenoidal surgery, or pituitary adenoma shrinkage after during treatment such as bromocriptine.[
The spontaneous CSF rhinorrhea in pituitary adenoma without treatment reported 16 cases in 13 English literatures.[
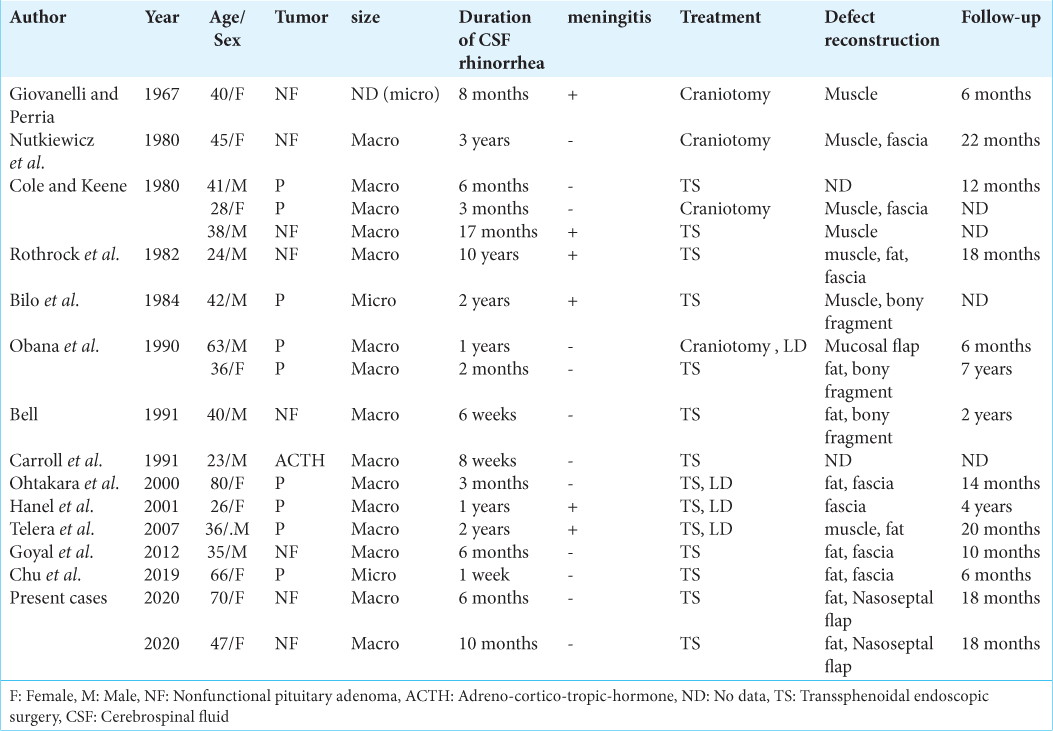
Although the pathophysiology of spontaneous CSF rhinorrhea in pituitary adenoma without treatment is unknown, there are three possible mechanisms. First, direct erosion of the skull base by tumor can lead to spontaneous CSF rhinorrhea. Nutkiewicz et al. assumed that a strong and competent diaphragm sellae could possibly be combined with the folding of the evaginated arachnoid space membrane, allowing the pituitary tumor to expand downward and promote CSF leakage into the sphenoid sinus.[
The spontaneous CSF rhinorrhea is often mistaken for allergic rhinitis of chronic sinusitis, resulting in delayed diagnosis or inappropriate management. Duration of spontaneous CSF rhinorrhea in these cases is long. Therefore, spontaneous CSF rhinorrhea may be high risk factor of meningitis. Among 16 cases, six got meningitis.[
At present, endoscopic transsphenoidal surgery appears to be the treatment of choices for CSF rhinorrhea because success rate reported is close to 95%.[
Many surgeons tried to use vascularized flaps harvested from the nasal cavity. Septal flap and middle turbinate flaps were used for endonasal repair of CSF leak.[
We underwent endoscopic transsphenoidal repair using NSF in both cases, commonly used for reconstruction of the endoscopic skull base surgery. To the best our knowledge, this is the first reported of pituitary adenoma with spontaneous CSF rhinorrhea using NSF.[
CONCLUSION
We present two cases of a pituitary adenoma with spontaneous CSF rhinorrhea using NSF. Pituitary adenoma should be suspected if there is a CSF rhinorrhea that occurs without a history of trauma or nasal disease. In addition, effective treatment can be performed using NSF, a technique for endoscopic skull base reconstruction.
Author contributions
Data curation: Beom-Mo Kang, Hyuk-Jin Oh, and KwangHui Ryu, Resources: Hyuk-Jin Oh, Writing – original draft: Beom-Mo Kang, Hyuk-Jin Oh, and Jae-Min Ahn Writing – review and editing: Hyuk-Jin Oh.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
This work was supported by the Soonchunhyang University Research Fund and the National Research Foundation of Korea (NRF) grant funded by the Korean government (Ministry of Science and ICT) (grant number: NRF-2019R1G1A109991313).
References
1. Bell MM. Transient cerebrospinal fluid rhinorrhea, blurred vision, and headache as presenting symptoms of pituitary adenoma. J Am Board Fam Pract. 1991. 4: 347-9
2. Bilo HJ, Ponssen H, van der Veen EA, Wolbers JG. Rhinorrhoea as the presenting symptom of pituitary adenoma. Clin Neurol Neurosurg. 1984. 86: 47-9
3. Calcaterra TC. Extracranial surgical repair of cerebrospinal rhinorrhea. Ann Otol Rhinol Laryngol. 1980. 89: 108-16
4. Carroll WR, Cohen S, Sullivan MJ. Spontaneous CSF rhinorrhea: An unusual presentation of a pituitary adenoma. Otolaryngol Head Neck Surg. 1991. 104: 380-3
5. Cavallo LM, Messina A, Gardner P, Esposito F, Kassam AB, Cappabianca P. Extended endoscopic endonasal approach to the pterygopalatine fossa: Anatomical study and clinical considerations. Neurosurg Focus. 2005. 19: E5
6. Chu X, Zhang Y, Tuo L, Cui L, Zhang P, Yuan X. Spontaneous cerebrospinal fluid rhinorrhea associated with an incidental pituitary adenoma. Br J Neurosurg. 2019. 20: 1-4
7. Cole IE, Keene M. Cerebrospinal fluid rhinorrhoea in pituitary tumours. J R Soc Med. 1980. 73: 244-54
8. Fujii M, Goto N, Shimada K, Moriyama H, Kikuchi K, Kida A. Demonstration of the nasal septal branches of the sphenopalatine artery by use of a new intravascular injection method. Ann Otol Rhinol Laryngol. 1996. 105: 309-11
9. Giovanelli M, Perria C. Cerebrospinal rhinorrhea with pituitary adenoma. (Case report). Acta Neurochir (Wien). 1967. 16: 261-6
10. Goyal N, Borkar SA, Agrawal D, Mahapatra AK. Pituitary adenoma presenting with cerebrospinal fluid rhinorrhea as the sole symptom. Neurol India. 2012. 60: 307-8
11. Hadad G, Bassagasteguy L, Carrau RL, Mataza JC, Kassam A, Snyderman CH. A novel reconstructive technique after endoscopic expanded endonasal approaches: Vascular pedicle nasoseptal flap. Laryngoscope. 2006. 116: 1882-6
12. Hanel RA, Prevedello DM, Correa A, Antoniuk A, Araújo JC. Cerebrospinal fluid fistula as the presenting manifestation of pituitary adenoma: Case report with a 4-year follow-up. Arq Neuropsiquiatr. 2001. 59: 263-5
13. Hirsch O. Successful closure of cere brospinal fluid rhinorrhea by endonasal surgery. AMA Arch Otolaryngol. 1952. 56: 1-12
14. Kassam AB, Thomas A, Carrau RL, Snyderman CH, Vescan A, Prevedello D. Endoscopic reconstruction of the cranial base using a pedicled nasoseptal flap. Neurosurgery. 2008. 63: S44-52
15. Lee HY, Kim HU, Kim SS, Son EJ, Kim JW, Cho NH. Surgical anatomy of the sphenopalatine artery in lateral nasal wall. Laryngoscope. 2002. 112: 1813-8
16. McCabe BF. The osteo-mucoperiosteal flap in repair of cerebrospinal fluid rhinorrhea. Laryngoscope. 1976. 86: 537-9
17. McCoul ED, Anand VK, Singh A, Nyquist GG, Schaberg MR, Schwartz TH. Long-term effectiveness of a reconstructive protocol using the nasoseptal flap after endoscopic skull base surgery. World Neurosurg. 2014. 81: 136-43
18. Nutkiewicz A, DeFeo DR, Kohut RI, Fierstein S. Cerebrospinal fluid rhinorrhea as a presentation of pituitary adenoma. Neurosurgery. 1980. 6: 195-7
19. Obana WG, Hodes JE, Weinstein PR, Wilson CB. Cerebrospinal fluid rhinorrhea in patients with untreated pituitary adenoma: Report of two cases. Surg Neurol. 1990. 33: 336-40
20. Ohtakara K, Matsubara T, Kojima T, Taki W, Waga S. Cerebrospinal fluid rhinorrhea associated with untreated prolactinoma case report. Neurol Med Chir (Tokyo). 2000. 40: 413-8
21. Rothrock JF, Laguna JF, Reynolds AF. CSF rhinorrhea from untreated pituitary adenoma. Arch Neurol. 1982. 39: 442-3
22. Simal-Julián JA, Miranda-Lloret P, Pérez de San Román Mena L, Sanromán-Álvarez P, García-Piñero A, Sanchis-Martín R. Impact of multilayer vascularized reconstruction after skull base endoscopic endonasal approaches. J Neurol Surg B Skull Base. 2020. 81: 128-35
23. Soudry E, Turner JH, Nayak JV, Hwang PH. Endoscopic reconstruction of surgically created skull base defects: A systematic review. Otolaryngol Head Neck Surg. 2014. 150: 730-8
24. Telera S, Conte A, Cristalli G, Occhipinti E, Pompili A. Spontaneous cerebrospinal fluid rhinorrhea as the presenting symptom of sellar pathologies: Three demonstrative cases. Neurosurg Rev. 2007. 30: 78-82

