

- Department of Othopedics, Clinica Alemana, Santiago, Chile.
DOI:10.25259/SNI_794_2020
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Ratko Yurac, Juan Jose Zamorano, Guisela Quinteros, Guillermo Izquierdo, Felipe Novoa, Rocío Brañes, Manuel Valencia, Alvaro Silva, Bartolomé Marré. Treatment strategies for managing cervical spine injuries in rugby players. 05-Jan-2021;12:6
How to cite this URL: Ratko Yurac, Juan Jose Zamorano, Guisela Quinteros, Guillermo Izquierdo, Felipe Novoa, Rocío Brañes, Manuel Valencia, Alvaro Silva, Bartolomé Marré. Treatment strategies for managing cervical spine injuries in rugby players. 05-Jan-2021;12:6. Available from: https://surgicalneurologyint.com/?post_type=surgicalint_articles&p=10509
Date of Submission
06-Nov-2020
Date of Acceptance
14-Dec-2020
Date of Web Publication
05-Jan-2021
Abstract
Background: Cervical spine fractures are potentially catastrophic injuries in rugby players. Here, we reviewed seven patients who sustained rugby-related cervical spine fractures. Notably, three of seven fractures were missed on initial X-rays, but were ultimately documented on CT studies obtained an average of 10 days later.
Methods: Seven patients sustained cervical spine fracture attributed to rugby (2009–2016) and were followed an average of 52 posttrauma months. Most injuries occurred at the C6-C7 level, and six of seven patients required surgery. Further, only two of seven patients exhibited resultant neurological deficits (e.g., one myelopathy and one radiculopathy).
Results: Although the rugby injury was sufficiently documented on initial X-rays in four patients, three initial X-rays missed fractures, which were documented on the CT studies obtained an average of 10 days later.
Conclusion: Rugby-related cervical fractures must be considered where players continue to complain of pain following trauma. Notably, routine X-rays may miss fractures in 3 of 7 cases (43%), thus warranting supplemental CT examinations to definitively rule out fractures.
Keywords: Cervical fracture, Cervical spine injuries, Return to sport, Rugby players, Tackles injuries
INTRODUCTION
Cervical injuries in rugby, although infrequent, may have devastating consequences such as significant neurologic injury.[
Here, we evaluated seven rugby players who sustained cervical fractures. However, 3 (43%) were missed on immediate posttraumatic X-rays but were diagnosed an average of 10 days later utilizing CT examinations.
MATERIALS AND METHODS
We evaluated seven patients who sustained rugby-related cervical fractures (2009–2016). Multiple clinical variables were studied utilizing basic statistics/SPSS software. Specifically, we studied the accuracy and frequency with which immediate posttraumatic plain X-rays failed to document cervical fractures in these patients, and at what interval subsequent CT studies correctly demonstrated such fractures.
Clinical data
Patient’s demographics and injury profile are described in [
RESULTS
X-ray versus CT confirmation of cervical fractures/levels in seven rugby patients
Radiological confirmation of cervical fractures occurring in seven rugby players required X-rays alone in four cases, while three CT studies were critical in defining originally missed fractures an average of 10 days later.
Surgery
Six patients required surgery for spinal instability attributed to rugby-related cervical fractures: five included anterior fusion utilizing cages, plates, and bone graft, while one underwent a posterior fusion with screws/bone graft [
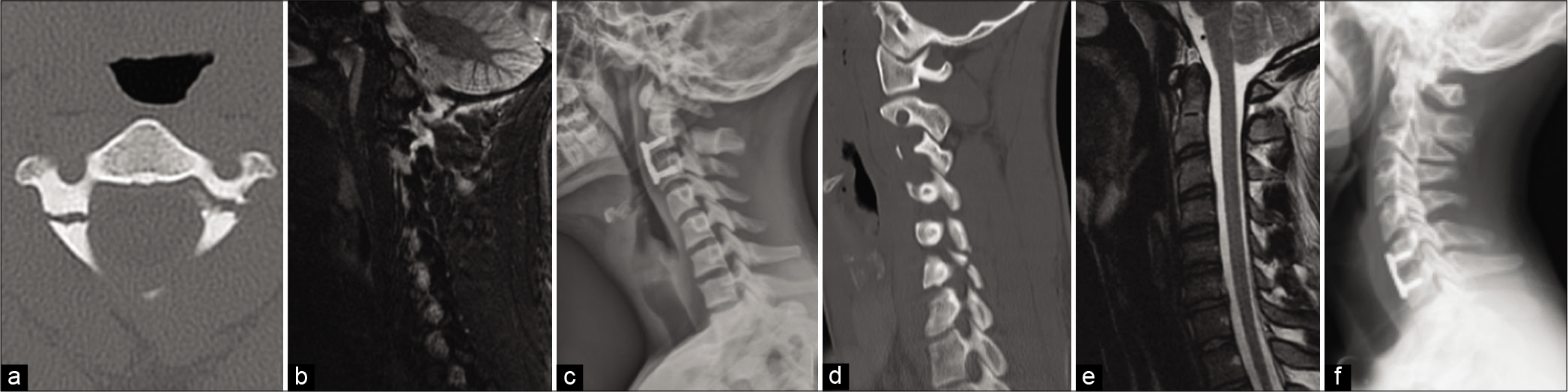
Figure 1:
(a) Axial CT scan of Case 3: bilateral C2 pars fracture with C2-C3 spondylolisthesis. (b) Sagittal STIR MRI of Case 3 showing C2-C3 ligamentous injury. (c) Lateral X-Ray of Case 3 after anterior C2-C3 arthrodesis with cage, plate and iliac crest graft. (d) Left sagittal CT scan of Case 4: Left C6 lateral mass fracture. (e) Mid-sagittal T2 MRI of Case 4 showing C6-C7 disc injury. (f) Lateral X-Ray of Case 4 after anterior C6-C7 arthrodesis with cage, plate and bone graft.

Postoperative course
The average postoperative follow-up duration was 52 months (range 37–117). None of the patients developed any postoperative or nonoperative complications.
DISCUSSION
In our series, four patients had cervical spine fractures confirmed on immediate postinjury X-ray studies, while three with initially negative X-ray studies but persistent pain complaints required additional CT studies obtained an average of 10 days posttrauma to diagnose a fracture.
The available literature regarding the diagnosis/treatment/ outcomes following cervical fractures in rugby players is limited. Certainly, one- or two-level instrumented fusions involving the subaxial cervical spine in these athletes serves as a relative contraindication to resume play if no radiographic fusion has been documented. Some would consider return to play once patients clinically exhibit pain-free range of motion and dynamic X-rays/CT studies confirmation of fusion.[
CONCLUSION
For seven patients with rugby-related cervical spine fractures, X-rays alone accurately document fractures in four patients, while three, with initial negative X-ray findings, required subsequent CT scans (e.g., an average of 10 days later) to establish the diagnosis of a cervical fracture.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Dennison CR, Macri EM, Cripton PA. Mechanisms of cervical spine injury in rugby union: Is it premature to abandon hyperflexion as the main mechanism underpinning injury?. Br J Sports Med. 2012. 46: 545-9
2. Hutton MJ, McGuire RA, Dunn R, Williams R, Robertson P, Twaddle B. Catastrophic cervical spine injuries in contact sports. Global Spine J. 2016. 6: 721-34
3. Quarrie K, Gianotti S, Murphy I. Injury risk in New Zealand rugby union: A nationwide study of injury insurance claims from 2005 to 2017. Sports Med. 2020. 50: 415-28
4. Quarrie KL, Cantu RC, Chalmers DJ. Rugby union injuries to the cervical spine and spinal cord. Sports Med. 2002. 32: 633-53
5. Shelly MJ, Butler JS, Timlin M, Walsh MG, Poynton AR, O’Byrne JM. Spinal injuries in Irish rugby: A ten-year review. J Bone Joint Surg Br. 2006. 88: 771-5
6. Swain MS, Lystad RP, Pollard H, Bonello R. Incidence and severity of neck injury in Rugby Union: A systematic review. J Sci Med Sport. 2011. 14: 383-9
7. Vives MJ, Harris CB.editors. Spine Injuries in Sports. Orthopaedic Knowledge Update. Spine 5, Rosemont, IL: American Academy of Orthopaedic Surgeons; 2017. p. 519-31

