

- Department of Neurosurgery, Gold Coast University Hospital, 1 Hospital Boulevard, Southport, Queensland 4125, Australia
- Department of Neurosurgery, Royal Adelaide Hospital, North Terrace, Adelaide, South Australia 5000, Australia
Correspondence Address:
Thorbjorn Loch-Wilkinson
Department of Neurosurgery, Royal Adelaide Hospital, North Terrace, Adelaide, South Australia 5000, Australia
DOI:10.4103/2152-7806.161407
Copyright: © 2015 Loch-Wilkinson T. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.How to cite this article: Loch-Wilkinson T, Tsimiklis C, Santoreneos S. Trigeminal neuralgia associated with Chiari 1 malformation: symptom resolution following craniocervical decompression and duroplasty: Case report and review of the literature. Surg Neurol Int 23-Jul-2015;6:
How to cite this URL: Loch-Wilkinson T, Tsimiklis C, Santoreneos S. Trigeminal neuralgia associated with Chiari 1 malformation: symptom resolution following craniocervical decompression and duroplasty: Case report and review of the literature. Surg Neurol Int 23-Jul-2015;6:. Available from: http://surgicalneurologyint.com/surgicalint_articles/trigeminal-neuralgia-associated-with-chiari-1-malformation-symptom-resolution-following-craniocervical-decompression-and-duroplasty-case-report-and-review-of-the-literature/
Abstract
Background:Trigeminal neuralgia (TN) may rarely be the presenting or only symptom of Chiari 1 malformation (CM). Isolated case reports have described resolution of TN following craniocervical decompression where TN is present in association with CM.
Case Report:This report discusses an unusual case of pure TN associated with CM that was successfully treated with craniocervical decompression and duroplasty and reviews the limited literature on the subject.
Conclusion:TN may be the sole presenting symptom of CM and can be successfully managed with craniocervical decompression. Clinicians should be aware of the association of TN with CM and consider surgical management.
Keywords: Chiari malformation, craniocervical decompression, duroplasty, trigeminal neuralgia
INTRODUCTION
Trigeminal neuralgia (TN) may rarely be the presenting or only symptom of Chiari 1 malformation (CM). Isolated case reports have described resolution of TN following craniocervical decompression where TN is present in association with CM. This report discusses an unusual case of this nature that was successfully treated with craniocervical decompression and duroplasty and reviews the limited literature on the subject.
CASE REPORT
A 39-year-old female presented with severe right sided facial pain of sudden onset. Her pain was so severe that she was admitted to a rural hospital for pain management. Her facial pain did not respond to oral medications including high dose carbamazepine, pregabalin, nonsteroidal antiinflammatory drugs (NSAIDS) and opiates. The patient was transferred to a tertiary hospital and investigation with magnetic resonance imaging (MRI) demonstrated a CM with tonsillar descent to the C1 level and very mildly increased T2 signal in the upper cervical cord [
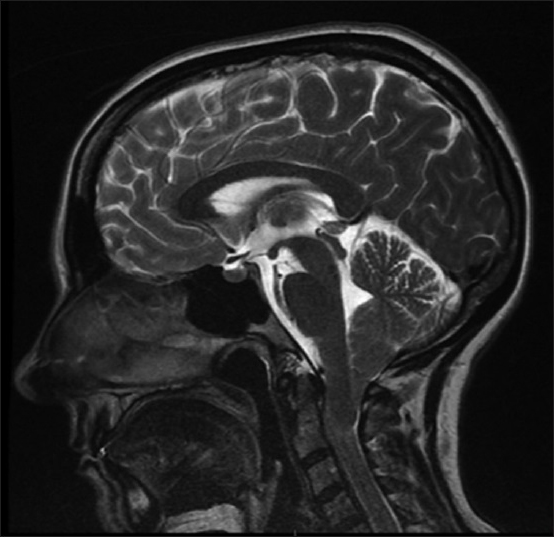
The patient proceeded to have a craniocervical decompression and duroplasty 8 weeks after first presentation of symptoms. At surgery tight arachnoid bands constricting the cerebellar tonsils were noted and the posterior aspect of the medulla had a gliotic and tented appearance consistent with chronic compression. Division of the arachnoid bands was performed and diathermy of the cerebellar tonsils without subpial aspiration. Native pericranium was used for duraplasty. There were no surgical complications. Following surgery the patient had immediate relief of facial pain and remains asymptomatic 1 year postsurgery with a satisfactory MRI appearance [

CONCLUSIONS
TN associated with CM is limited to a very small number of case reports. A 2008 case report with a literature review found only 19 cases in the English language literature,[
Postulated mechanisms of generation of TN due to Chiari malformation include (i) vascular compression at the nerve root entry zone, which could be affected by hydrocephalus or anatomic factors related to the Chiari malformation, such as a small posterior fossa; (ii) demyelination; (iii) microischaemic changes; and (iv) direct brainstem compression.[
Case reports describe a range of successful treatments in cases of TN associated with Chiari malformation including medical treatment with carbamazepine[
This case report contributes to the very limited number of case reports of Chiari malformation with pure TN, and those successfully treated with craniocervical decompression and duroplasty. Neurologists and neurosurgeons should consider this diagnosis in presentations of TN with concurrent CM and consider surgical treatment.
References
1. Ayuso-Peralta L, Jiménez-Jiménez FJ, Tejeiro J, Zurdo M, Cabrera-Valdivia F, García-Albea E. Trigeminal neuralgia associated with Arnold Chiari malformation. Rev Neurol. 1999. 29: 1345-
2. Caranci G, Mercurio A, Altieri M, Di Piero V. Trigeminal neuralgia as the sole manifestation of an Arnold-Chiari type I malformation: Case report. Headache. 2008. 48: 625-7
3. Chakraborty A, Bavetta S, Leach J, Kitchen N. Trigeminal neuralgia presenting as Chiari I malformation. Minim Invasive Neurosurg. 2003. 46: 47-9
4. Gelabert González M. Trigeminal neuralgia as the first symptom of Chiari malformation. Neurologia. 2001. 16: 189-90
5. Gnanalingham K, Joshi SM, Lopez B, Ellamushi H, Hamlyn P. Trigeminal neuralgia secondary to Chiari's malformation-treatment with ventriculoperitoneal shunt. Surg Neurol. 2005. 63: 586-8
6. González-Bonet LG, Piquer J. Trigeminal Neuralgia: A Symptom of Chiari I. Neurosurgery. 2012. 71: 911-2
7. Iváñez V, Moreno M. Trigeminal neuralgia in children as the only manifestation of Chiari I malformation. Rev Neurol. 1999. 28: 485-7
8. Papanastassiou AM, Schwartz RB, Friedlander RM. Chiari I malformation as a cause of trigeminal neuralgia: Case report. Neurosurgery. 2008. 63: E614-5
9. Peñarrocha M, Okeson JP, Peñarrocha MS, Angeles Cervello M. Orofacial pain as the sole manifestation of syringobulbia-syringomyelia associated with Arnold-Chiari malformation. J Orofac Pain. 2001. 15: 170-3
10. Rosetti P, Oulad Ben Taib N, Brotchi J, De Witte O. Arnold Chiari Type I malformation presenting as a trigeminal neuralgia: Case report. Neurosurgery. 1999. 44: 1122-4
11. Teo C, Nakaji P, Serisier D, Coughlan M. Resolution of trigeminal neuralgia following third ventriculostomy for hydrocephalus associated with chiari I malformation: Case report. Minim Invasive Neurosurg. 2005. 48: 302-5
12. Than KD, Sharifpour M, Wang AC, Thompson BG, Pandey AS. Chiari I malformation manifesting as bilateral trigeminal neuralgia: Case report and review of the literature. J Neurol Neurosurg Psychiatry. 2011. 82: 1058-9
13. Tortosa A, Arbizu T, Ferran E, Peres Serra J. Arnold Chiari malformation presenting as trigeminal neuralgia. Neurologia. 1991. 6: 148-50
14. Uldry PA, Fankhauser H, de Tribolet N. Trigeminal involvement and peripheral facial paralysis caused by Arnold-Chiari malformation with hydrocephalus. Neurochirurgie. 1985. 31: 73-5
15. Vince GH, Bendszus M, Westermaier T, Solymosi L, Ernestus RI, Matthies C. Bilateral trigeminal neuralgia associated with Chiari's type I malformation. Br J Neurosurg. 2010. 24: 474-6


Bikal Gurung
Posted April 27, 2018, 4:01 am
Hi my name is Bikal Gurung, 39 year old male from UK. In 2013 I was diagnosed CM with syrinx at the upper cervical area. No surgical intervention has done yet. Since 2014 I have developed this horrible disease trigiminal neuralgia which could be secondary to Chiari Malformation (I am paraplegic as well due to spinal injury in 2003). I have mixed opinion from neurologists whether or not my tn is due to my CM. After reading the story above I am quite sure this trigiminal neuralgia I am suffering is because of Chiari Malformation. I am really looking forward to have the operation done for my cm so that this horrible symptom will gone.