

- Section of Neurosurgery Hospital, CMQ Premiere, Puerto Vallarta, Mexico
Correspondence Address:
Luis A. Robles
Section of Neurosurgery Hospital, CMQ Premiere, Puerto Vallarta, Mexico
DOI:10.4103/2152-7806.198734
Copyright: © 2017 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Luis A. Robles. True oblique axis fracture associated with congenital anomalies of the upper cervical spine: Case report of an unusual fracture pattern. 19-Jan-2017;8:7
How to cite this URL: Luis A. Robles. True oblique axis fracture associated with congenital anomalies of the upper cervical spine: Case report of an unusual fracture pattern. 19-Jan-2017;8:7. Available from: http://surgicalneurologyint.com/surgicalint_articles/true-oblique-axis-fracture-associated-with-congenital-anomalies-of-the-upper-cervical-spine-case-report-of-an-unusual-fracture-pattern/
Date of Submission
24-Aug-2016
Date of Acceptance
12-Nov-2016
Date of Web Publication
19-Jan-2017
Abstract
Background:Acute traumatic axis fractures are common cervical spine injuries often caused by road accidents or falls. They are usually classified into three different types, namely, odontoid fractures, Hangman's fractures, and miscellaneous fractures. Congenital malformations of the craniovertebral junction (CVJ), although typically asymptomatic, may result in neural compression or instability, especially following trauma. Here, the authors present an unusual oblique axis fracture occurring in conjunction with several malformations of the upper cervical spine.
Case Description:Following a motor vehicle accident, a 25-year-old female's radiographic studies showed an oblique axis fracture involving both the anterior and posterior elements along with an anterior and posterior Klippel–Feil syndrome (KFS) anomaly. Following treatment in a halo vest, the patient maintained alignment, and ultimately the fracture was fused.
Conclusions:True oblique fractures of the axis are rare, as in the case presented, and may occasionally occur in conjunction with KFS of the upper cervical spine.
Keywords: C2 fracture, craniovertebral congenital anomalies, Klippel–Feil syndrome, miscellaneous axis fractures, oblique axis fracture
INTRODUCTION
Oblique axis fractures are rare, and the unique anatomy/biomechanics of the axis contributes to a variety of fracture patterns following cervical trauma.[
CASE REPORT
Following a motor vehicle accident, a 25-year-old female complained of intense neck pain, but remained neurologically intact. The lateral cervical radiograph showed an oblique fracture of the axis; the fracture diagonally separated the vertebra in two parts and extended from the body of the axis to the posterior elements. In addition, the computed tomography (CT) scan revealed several craniovertebral junction (CVJ) anomalies, which included spontaneous KFS fusion of the C2-C3 disc space and the C2-C3 right articular facets/laminae. Furthermore, the anterior C1-arch was bifid and there was a partial agenesis of the posterior C1 arch [Figure
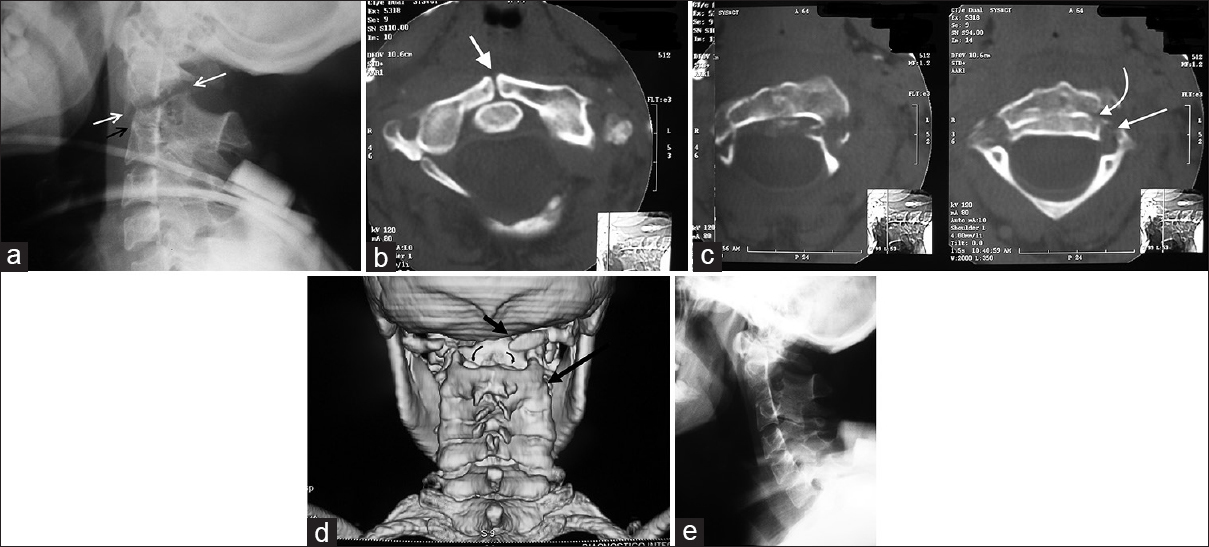
Figure 1
(a) Lateral radiograph. An oblique fracture of the axis is observed. The fracture line extends obliquely from posterior elements to the vertebral body (white arrows). The fracture line divides obliquely the axis vertebra in two fragments. Note the C2-C3 intervertebral space fusion (black arrow). (b) Axial CT. There is an absence of midline fusion of anterior C1 arch (white arrow). The presence of sclerosis of both borders indicates that this is not a fracture. (c) Axial CT. This image shows the fracture in the body of C2 (curve arrow). The fracture line in the posterior elements runs through supero-anterior border of the pars and foramina transversarium (straight arrow). (d) 3D CT reconstruction. The posterior arch of C1 is incomplete (short arrow). Also note the absence of right C2-C3 articular space (long arrow) and fusion of laminae. The fracture line in the body of the axis is also observed (curved arrows). (e) Lateral radiograph showing adequate alignment after treatment with halo-vest. Note the bridging callus in the anterior border of the C2 body
DISCUSSION
Unique axis fracture with craniovertebral junction anomalies
Different types of CVJ anomalies may accompany upper cervical KFS.[
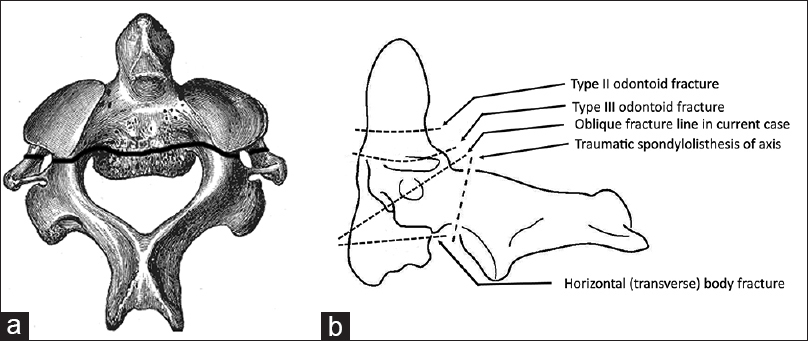
Figure 2
(a) A schematic drawing of the fracture line observed in this case. The fracture line traverse both anterior (body of C2) and posterior elements (pars, lateral masses, foramina tranversarium). (b) This image shows the most common type of C2 fractures and the oblique fracture observed in this patient
Upper cervical vertebral anomalies increase susceptibility to trauma
Patients with ankylosing spondylitis or diffuse idiopathic skeletal hyperostosis are uniquely prone to sustaining spinal fractures following even trivial trauma.[
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Nagib MG, Maxwell RE, Chou SN. Identification and management of high-risk patients with Klippel-Feil syndrome. J Neurosurg. 1984. 6: 523-30
2. Pryputniewicz DM, Hadley MN. Axis fractures. Neurosurgery. 2010. 66: 68-82
3. Ryken TC, Hadley MN, Aarabi B, Dhall SS, Gelb DE, Hurlbert RJ. Management of isolated fractures of the axis in adults. Neurosurgery. 2013. p. 132-50
4. Westerveld LA, Verlaan JJ, Oner FC. Spinal fractures in patients with ankylosing spinal disorders: A systematic review of the literature on treatment, neurological status and complications. Eur Spine J. 2009. 18: 145-56

