

- Department of Spinal Surgery, Kameda Medical Center, Kamogawa-Shi, Chiba, Japan.
DOI:10.25259/SNI_851_2020
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Isamu Miura, Motoo Kubota, Nobuhiko Momozaki, Masahito Yuzurihara. Two cases of normal pressure hydrocephalus caused by ependymoma of the cauda equina. 05-Jan-2021;12:8
How to cite this URL: Isamu Miura, Motoo Kubota, Nobuhiko Momozaki, Masahito Yuzurihara. Two cases of normal pressure hydrocephalus caused by ependymoma of the cauda equina. 05-Jan-2021;12:8. Available from: https://surgicalneurologyint.com/surgicalint-articles/10507/
Date of Submission
28-Nov-2020
Date of Acceptance
12-Dec-2020
Date of Web Publication
05-Jan-2021
Abstract
Background: Normal pressure hydrocephalus (NPH) associated with tumors of the cauda equina is rare. Here, we report two cases of NPH attributed to cauda equina ependymomas.
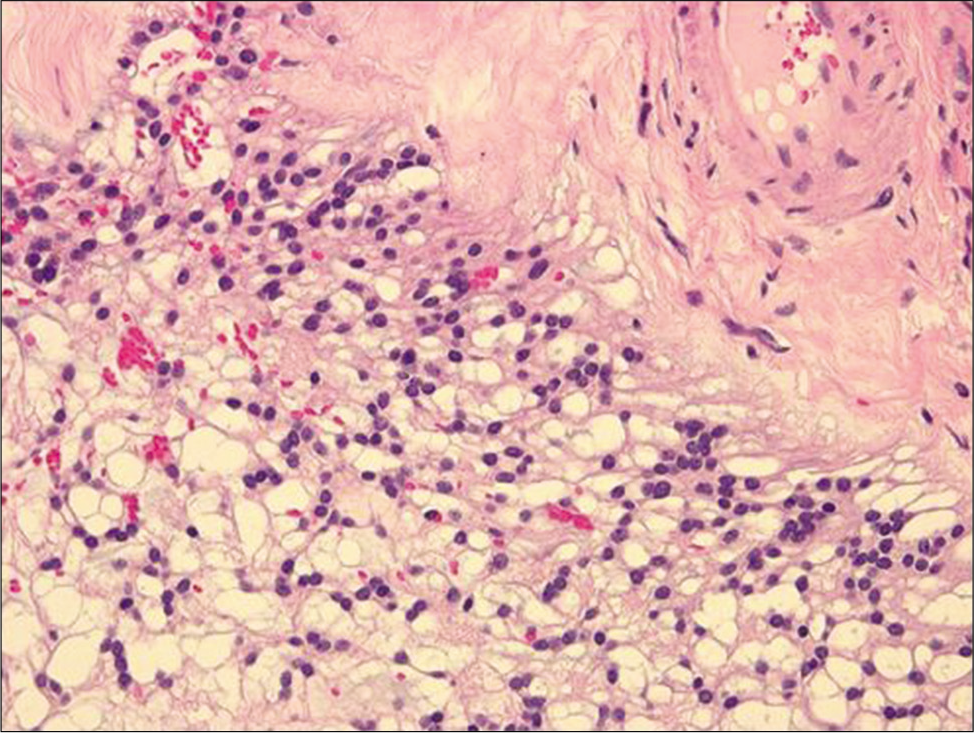
Case Description: A 63-year-old male presented with progressive gait disturbance, dementia, and urinary incontinence. When the lumbar MR documented an intradural tumor involving the cauda equina at the L2-L3 level; the tumor was excised; pathologically, it proved to be a myxopapillary ependymoma. Postoperatively, however, the patient’s continued gait disturbance led to a brain CT that documented ventricular dilation consistent with NPH; following ventriculoperitoneal (VP) shunt placement his symptoms improved. A 65-year-old female also presented with gait disturbance, dementia, and urinary retention. Here, procedures were performed in reverse. When a brain CT showed hydrocephalus, a VP shunt was placed. When symptoms persisted, a lumbar MR demonstrated a T12-L2 intradural tumor; following a lumbar laminectomy for tumor excision, symptoms stabilized. The pathological diagnosis was also consistent with a conus/cauda equina ependymoma. Over the next 10 years, the patient had residual bladder dysfunction (e.g., requiring straight catheterization), but had no shunt dysfunction.
Conclusion: We observed two cases of ependymomas of the cauda equina and brain CTs documenting NPH that was successfully surgically managed with stabilization of neurological deficit. In the first case, L2-L3 laminectomy for tumor removal was succeeded by shunting for NPH, while in the second case, initial VP shunting for NPH was followed by a T12-L2 laminectomy for tumor excision.
Keywords: Cauda equina, Ependymoma, Myxopapillary ependymoma, Normal pressure hydrocephalus, Spinal tumor
INTRODUCTION
Normal pressure hydrocephalus (NPH) associated with tumors of the cauda equina is rare.[
CASE DESCRIPTION
Case 1
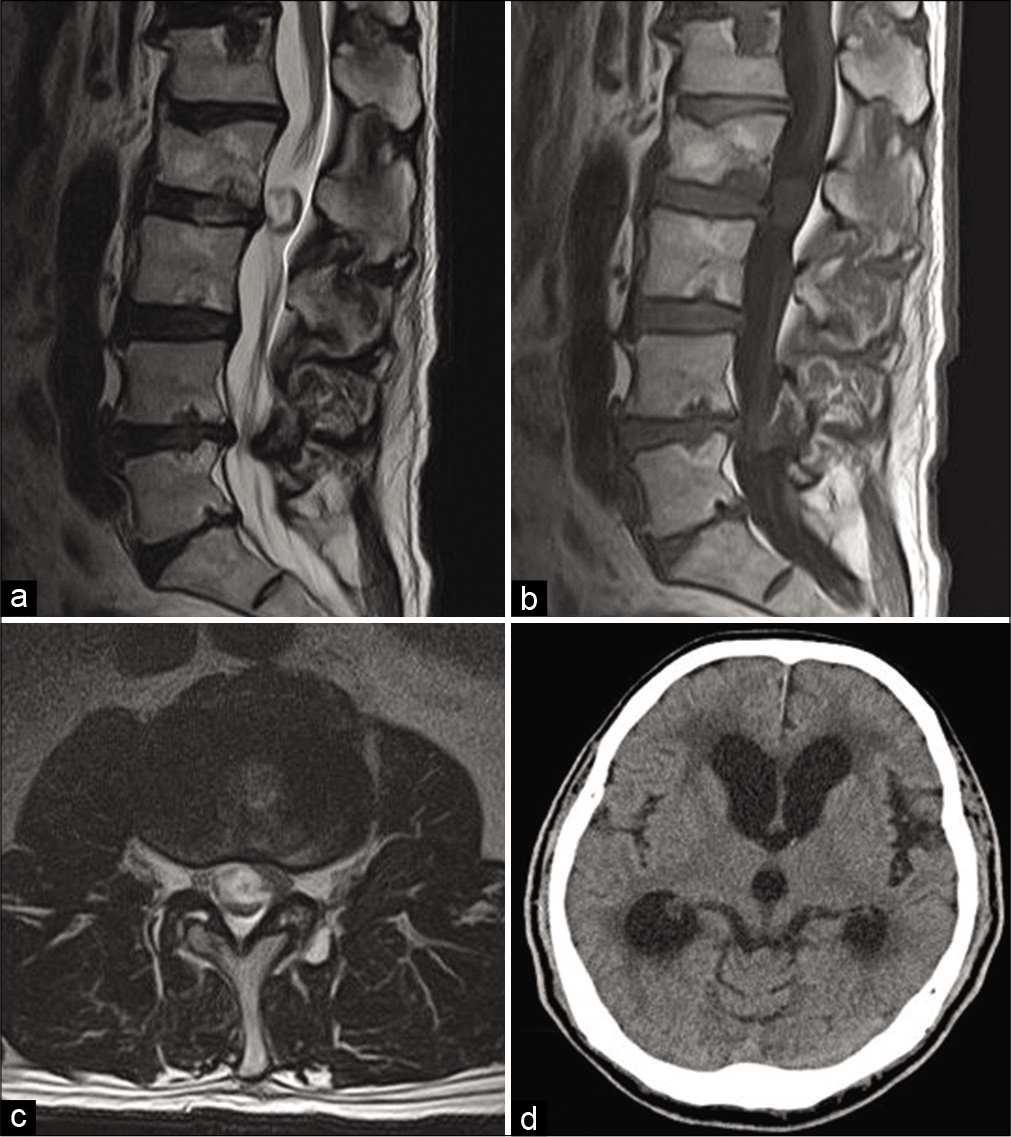
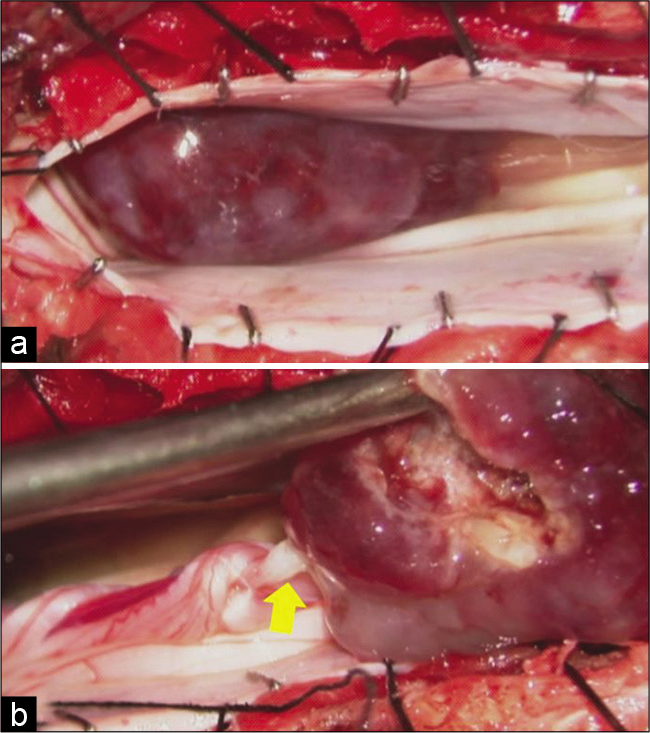
A 63-year-old male developed right lower extremity weakness over a 6-month period associated with gait disturbance, dementia, and urinary incontinence. The lumbar MR demonstrated an intradural tumor at the L2-L3 level involving the cauda equina: the lesion was hypointense on T1 and hyperintense on T2-weighted images, but due to renal failure, no contrast was administered [

Case 2
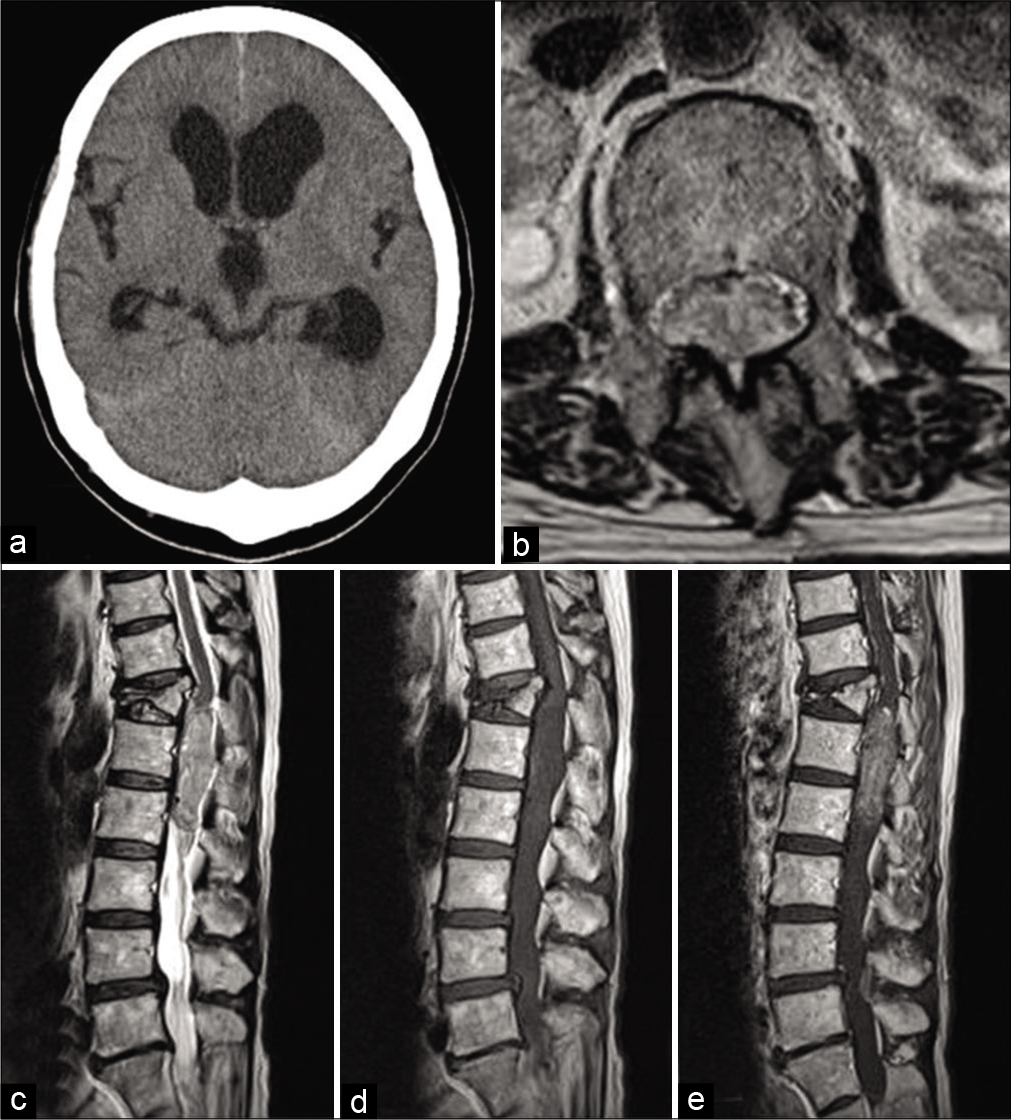
A 65-year-old female also presented with gait disturbance, dementia, and urinary retention; her neurological examination only revealed an ataxic gait. The brain CT demonstrated ventricular dilation consistent with NPH and a VP shunt was placed [
DISCUSSION
NPH associated with tumors of the cauda equina is rare.[
CONCLUSION
Here, we presented two cases of cauda equina ependymomas that contributed to increased intracranial pressure (e.g., consistent with NPH). The first patient required primary thoracolumbar/lumbar L2-L3 ependymoma tumor excision followed by secondary VP shunting, while in the second case, initial VP shunting was succeeded by T12-L2 laminectomy for tumor removal.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Khoulali M, Haouas MY, Mortada J, Srour R. Tumors of the conus medullaris and of the cauda equina associated with chronic hydrocephalus: about 2 cases. Pan Afr Med J. 2018. 29: 206
2. Phan TG, Krauss WE, Fealey RD. Recurrent lumbar ependymoma presenting as headache and communicating hydrocephalus. Mayo Clin Proc. 2000. 75: 850-2
3. Ting SL, Jobli AT, Sim SK, Ojep DK. Myxopapillary ependymoma of cauda equina presented with communicating hydrocephalus and papilloedema: A case report. Med J Malaysia. 2019. 74: 338-40
4. Tzekov C, Naydenov E, Kalev O. Ependymoma of the cauda equina starting with communicating hydrocephalus: A case report. Pediatr Neurosurg. 2007. 43: 399-402
5. Wajima D, Ida Y, Inui T, Nakase H. Normal pressure hydrocephalus caused by a spinal neurinoma at the cauda equina level: A case report. Neurol Med Chir (Tokyo). 2014. 54: 423-7

