

Unilateral atlantoaxial pseudoarticulation: A case report, literature review, and proposed mechanism
- Department of Neurological Surgery, The Ohio State University, Columbus, Ohio, United States.
DOI:10.25259/SNI_603_2019
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Ryan G. Eaton, Stephanus V. Viljoen. Unilateral atlantoaxial pseudoarticulation: A case report, literature review, and proposed mechanism. 07-Feb-2020;11:20
How to cite this URL: Ryan G. Eaton, Stephanus V. Viljoen. Unilateral atlantoaxial pseudoarticulation: A case report, literature review, and proposed mechanism. 07-Feb-2020;11:20. Available from: https://surgicalneurologyint.com/surgicalint-articles/9863/
Date of Submission
24-Dec-2019
Date of Acceptance
20-Jan-2020
Date of Web Publication
07-Feb-2020
Abstract
Background: Atlantoaxial pseudoarticulation rarely involves the cervical spine, and its etiology is unclear. In theory, pseudoarticulation is comparable to Bertolotti’s syndrome in the lumbar spine or may be attributed to an aberrant focal fusion between C0-C1-C2 that occurs during the gastrulation of embryologic development.
Case Description: A 39-year-old female presented with neck pain and upper extremity weakness. Magnetic resonance/computed tomography studies documented a left-sided unilateral pseudoarticulation between the lamina of C1 and C2 causing compression of the dorsal spinal cord. Following resection of the accessory C1/C2 joint utilizing a C1 hemilaminectomy and partial C2 laminectomy, the patient’s neck pain and weakness resolved. Histologically, the tissue showed benign osteocartilaginous tissue with no synovial capsule.
Conclusion: Here, the authors present a case of occiput-C1-C2 pseudojoint formation, leading to clinical and radiographic findings of cord compression due to boney outgrowth.
Keywords: Accessory joint, Atlantoaxial joint, Bertolotti’s syndrome, Cervical spine, Pseudoarticulation
INTRODUCTION
Pseudoarticulations of the C1-C2 complex are rare.[
CASE REPORT
A 39-year-old female presented with a 10-month history of the right-sided neck pain and bilateral hand numbness/weakness, accompanied by leg heaviness. Her neck pain was exacerbated by movement but was also present at rest. She described an accident while on an all-terrain vehicle 2 years ago but did not recall sustaining any specific cervical injury. She exhibited 4/5 strength involving both hands and the right triceps, decreased sensation throughout the hands, with diminished light touch, pain, and temperature in the hands. Reflexes remained intact. The outside computed tomography obtained 2 months previously demonstrated osseous hypertrophy of the C1 lamina, while the cervical magnetic resonance (MR) showed a pseudoarticulation between the lamina of C1 and C2 [
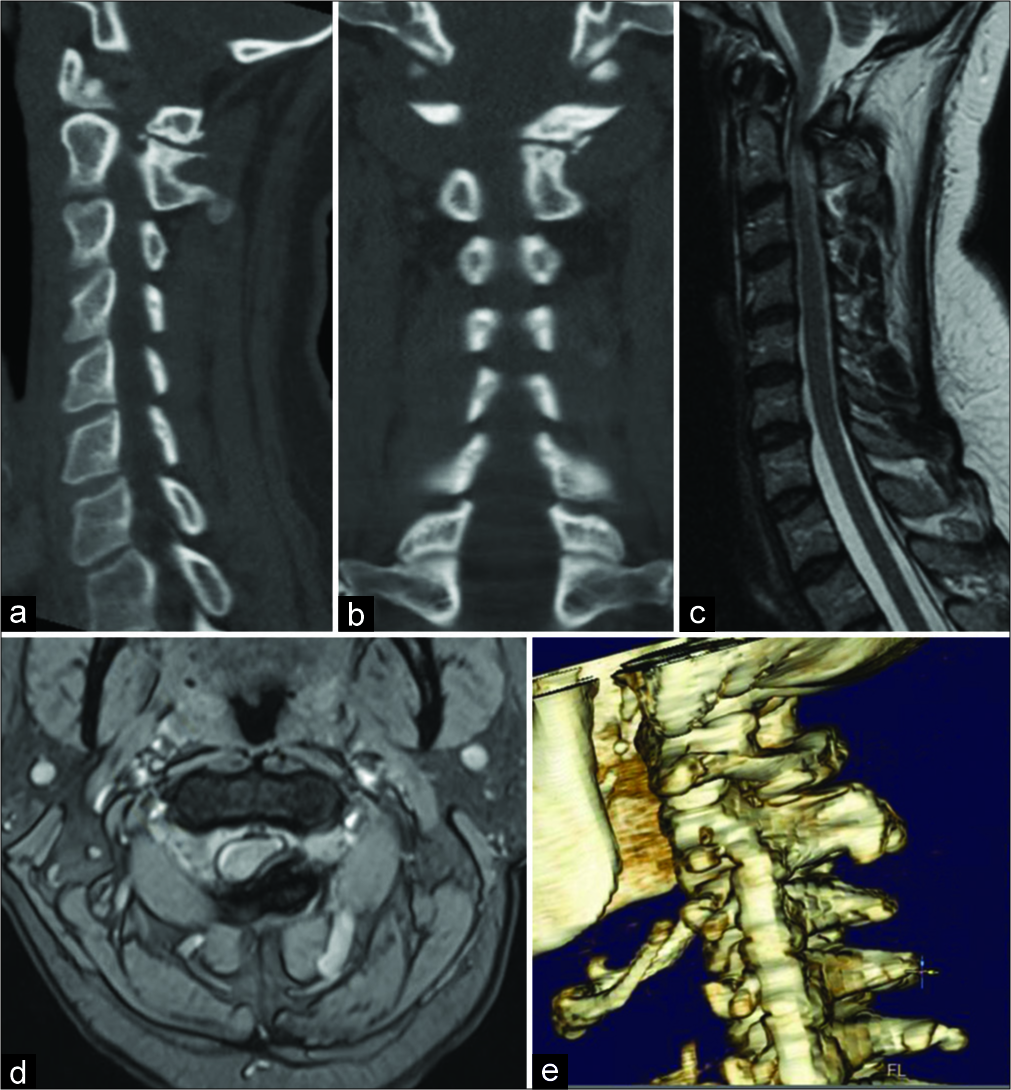
Figure 1:
Computed tomography (CT) images in sagittal (a) and coronal (b) plans show an osseous pseudojoint between the left lamina of C1 and C2. T2-weighted magnetic resonance images in the sagittal (c) and axial (d) planes demonstrate the degree of cord compression caused by the complex. Finally, the topography of the pseudojoint can be appreciated on three-dimensional CT reconstruction (e).
The patient underwent left-sided C1 hemilaminectomy and partial C2 laminectomy at which time the thickened pseudoarticulation at C1 was removed and was sent for pathology. Histologically, it proved to be “benign osteocartilaginous tissue with fibrosis.” The patient did well and regained full strength bilaterally on postoperative day 1. Two weeks later, initial neck pain and prior numbness resolved. Postoperative flexion and extension films showed no delayed instability. Six months later, with mild residual occipital pain, the MR image demonstrated complete resection of the lesion and no residual left-sided stenosis.
DISCUSSION
We found three similar reported cases in the literature focusing on C1-C2 pseudoarticulation [
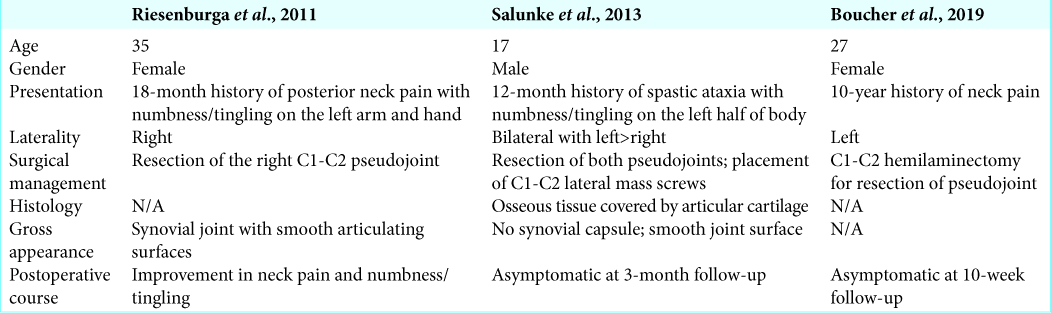
All three cases underwent successful resection of the pseudoarticulation with neurologic improvement.[
Further work is required to quantify the relationship between subaxial kyphosis and formation of upper cervical accessory joints. Further work should focus on delineating the clinical conditions that may increase risk for the formation of upper cervical accessory joints, particularly the degree subaxial kyphosis.
CONCLUSION
This case describes a 39-year-old female who presented with neck pain and was found to have left-sided unilateral pseudoarticulation between the lamina of C1 and C2 causing compression of the dorsal spinal cord who improved with C1 hemilaminectomy and partial C2 laminectomy. Atlantoaxial pseudoarticulation of the C1-C2 complex is exceedingly rare and, in theory, is comparable to Bertolotti’s syndrome in the lumbar spine, although further work is needed to describe the biologic and mechanical factors that are involved in this disorder.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Boucher AB, Kashlan ON, Gary MF, Refai D. Atlantoaxial pseudoarticulation as a cause of neck pain: case illustration. J Neurosurg Spine. 2018. 30: 182-3
2. Jancuska JM, Spivak JM, Bendo JA. A review of symptomatic lumbosacral transitional vertebrae: Bertolotti’s syndrome. Int J Spine Surg. 2015. 9: 42-
3. Klimo P, Rao G, Brockmeyer D. Congenital anomalies of the cervical spine. Neurosurg Clin N Am. 2007. 18: 463-78
4. Mahato NK. Morphological traits in sacra associated with complete and partial lumbarization of first sacral segment. Spine J. 2010. 10: 910-5
5. Riesenburger RI, Klimo P, Yao KC. A fourth atlantoaxial joint: An initial description. Spine J. 2011. 11: e6-9
6. Salunke P, Futane S, Vaiphei K. Posterior bilateral supernumerary atlantoaxial facets: True or false joint?. Spine (Phila Pa 1976). 2013. 38: E1633-5

