

- Department of Orthopaedics and Spine Surgery, Bharat Ratna Dr. Babasaheb Ambedkar Memorial Hospital, Byculla, Mumbai,
- Spine Services, Chaitanya Spine Clinic, Cardinal Gracias Memorial Hospital, Vasai, Mumbai, Maharashtra, India,
- Spine Services, Star Medica, Aguascalientes, Mexico,
- Department of Orthopaedics, Lilavati Hospital and Research Centre, Bandra, Mumbai, Maharashtra, India.
Correspondence Address:
Atif Naseem, Department of Orthopaedics and Spine Surgery, Bharat Ratna Dr. Babasaheb Ambedkar Memorial Hospital, Byculla, Mumbai, Maharashtra, India.
DOI:10.25259/SNI_900_2022
Copyright: © 2022 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Ayush Sharma1, Atif Naseem1, Harsh Agrawal1, Nandan Marathe2, Felipe Eduardo Nares-Lopez3, Manojkumar B. Gaddikeri4. Unilateral facet cyst at the atlantoaxial joint leading to cervical myelopathy: A case report and review of literature. 02-Dec-2022;13:557
How to cite this URL: Ayush Sharma1, Atif Naseem1, Harsh Agrawal1, Nandan Marathe2, Felipe Eduardo Nares-Lopez3, Manojkumar B. Gaddikeri4. Unilateral facet cyst at the atlantoaxial joint leading to cervical myelopathy: A case report and review of literature. 02-Dec-2022;13:557. Available from: https://surgicalneurologyint.com/surgicalint-articles/12043/
Date of Submission
28-Sep-2022
Date of Acceptance
08-Nov-2022
Date of Web Publication
02-Dec-2022
Abstract
Background: Spinal synovial cysts are rare in the cervical spine where they may cause myeloradiculopathy. Contrast MR studies help differentiate these from other lesions. The optimal treatment is often surgical removal.
Case Description: A 47-year-old male presented with axial neck pain, numbness, and left-hand paresthesia. When the MR study showed dorsolateral cord compression due to a left-sided C1–C2 facet cyst, he underwent a unilateral decompression/fusion. Adequate cyst removal/excision was documented on a postoperative MR performed 2 weeks and 3 months postoperatively.
Conclusion: A 47-year-old male presented with myelopathy attributed to an MR-documented dorsolateral C1/ C2 facet cyst. Following excision/decompression of the cyst and posterior fusion, the patient’s symptoms/signs resolved.
Keywords: Cervical spine cysts, Goel-Harms technique, Unilateral C1-C2 fusion, Unilateral facet cyst
INTRODUCTION
Cervical spinal arachnoid cysts, alternatively called ganglion, retrodental, or juxtafacet cysts, are rare in the cervical spine.[
CASE DESCRIPTION
A 47-year-old male presented with a nontraumatic 4-month history of axial neck pain, with numbness/paresthesia in involving his left upper limb (i.e., C6/C7 distribution).
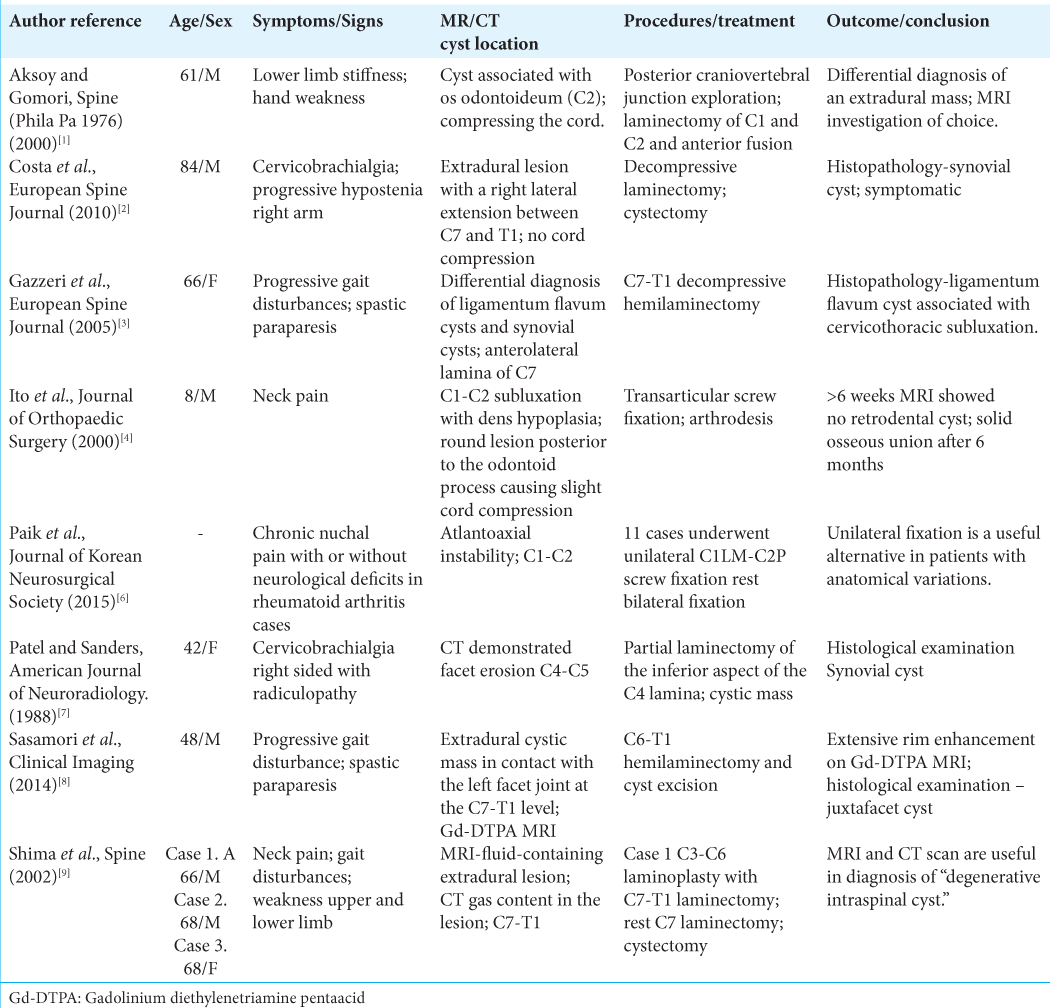
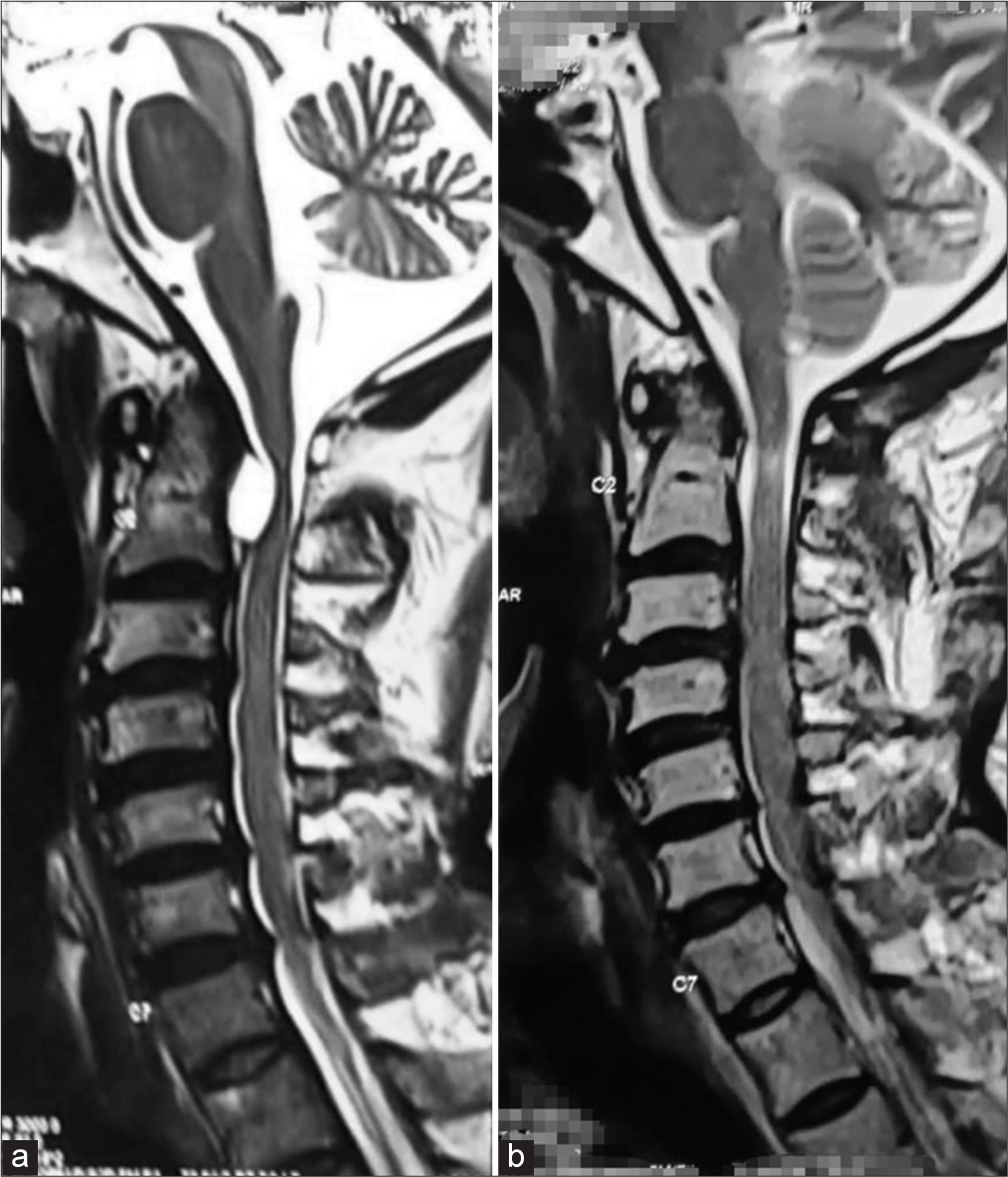
The preoperative neck 7 visual analog score (VAS), 28 Oswestry Disability Index, and 16 modified Japanese Orthopaedic Association (mJOA) scores were consistent with radiculopathy/myelopathy. The MRI showed 0.7 × 1.1 × 1.3 T1 hypo/T2 hyperintense nonenhancing extradural cystic lesion at the C2 level. It was located beneath the posterior longitudinal ligament (PLL) resulting in cervical spinal cord compression/severe canal stenosis with a high-intensity left cord signal. The preoperative CT angiogram showed that the vertebral arteries were not involved, while also confirming the maximum diameter of the C2 pedicle (i.e., isthmus 2.6 mm on the right and 3 mm on the left side).
Surgery and postoperative outcome
The patient underwent a C1–C2 lateral mass pedicle screw/ rod fusion only on the left side (i.e., Goel-Harms technique) as the C2 isthmus was too small on the right [

DISCUSSION
Few reports of high cervical synovial cysts
Few reports of supra-axial cervical synovial cysts are found in the literature [
Import of preoperative CT and CTA studies
The preoperative CT demonstrated that the maximum diameter of the contralateral pedicle on the right was just 2.6 mm, insufficient for the placement of a screw, while the left pedicle at 3.0 mm was adequate for screw fixation. In addition, the CTA documented that the left synovial cyst did not impinge on the vertebral artery.
Surgery
The patient successfully underwent a left-sided C1/C2 pedicle screw fusion alone.[
CONCLUSION
Synovial cysts of the cervical spine are extremely rare. They are best defined by contrast MRI studies and respond well to direct surgical excision utilizing decompression alone or decompression with fusion as indicated.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Publication of this article was made possible by the James I. and Carolyn R. Ausman Educational Foundation.
Conflicts of interests
There are no conflicts of interest.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Journal or its management. The information contained in this article should not be considered to be medical advice; patients should consult their own physicians for advice as to their specific medical needs.
References
1. Aksoy FG, Gomori JM. Symptomatic cervical synovial cyst associated with an os odontoideum diagnosed by magnetic resonance imaging: Case report and review of the literature. Spine. 2000. 25: 1300-2
2. Costa F, Menghetti C, Cardia A, Fornari M, Ortolina A. Cervical synovial cyst: Case report and review of literature. Eur Spine J. 2010. 19: 100-2
3. Gazzeri R, Galarza M, Gorgoglione L, Bisceglia M, D’Angelo V. Cervical cyst of the ligamentum flavum and C7-T1 subluxation: Case report. Eur Spine J. 2005. 14: 807-9
4. Ito T, Hayashi M, Ogino T. Retrodental synovial cyst which disappeared after posterior C1-C2 fusion: A case report. J Orthop Surg. 2000. 8: 83-7
5. Miller JD, Al-Mefty O, Middleton TH. Synovial cyst at the craniovertebral junction. Surg Neurol. 1989. 31: 239-42
6. Paik SC, Chun HJ, Bak KH, Ryu J, Choi KS. Unilateral C1 lateral mass and C2 pedicle screw fixation for atlantoaxial instability in rheumatoid arthritis patients: Comparison with the bilateral method. J Korean Neurosurg Soc. 2015. 57: 460-4
7. Patel SC, Sanders WP. Synovial cyst of the cervical spine: Case report and review of the literature. AJNR Am J Neuroradiol. 1988. 9: 602
8. Sasamori T, Hida K, Anzai K, Yano S, Kato Y, Tanaka S. A case of cervical juxtafacet cyst with extensive rim enhancement on Gd-DTPA MRI. Clin Imag. 2014. 38: 199-201
9. Shima Y, Rothman SL, Yasura K, Takahashi S. Degenerative intraspinal cyst of the cervical spine: Case report and literature review. Spine. 2002. 27: E18-22

