

- Department of Neurosurgery, National Hospital Organization Nagasaki Medical Center, Omura, Nagasaki, Japan.
- Department of Nurse Practitioner, National Hospital Organization Nagasaki Medical Center, Omura, Nagasaki, Japan.
Correspondence Address:
Ichiro Kawahara, Department of Neurosurgery, Nagasaki Medical Center, Omura, Nagasaki, Japan.
DOI:10.25259/SNI_1108_2021
Copyright: © 2022 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Eri Shiozaki1, Ichiro Kawahara1, Daiki Uchida1, Yoichi Morofuji1, Tomonori Ono1, Wataru Haraguchi1, Kazuya Honda2, Tomoya Moritsuka2, Keisuke Tsutsumi1. Unruptured cerebral aneurysms with the segmental duplicated middle cerebral artery formed a fenestrated structure at origin. 29-Jan-2022;13:33
How to cite this URL: Eri Shiozaki1, Ichiro Kawahara1, Daiki Uchida1, Yoichi Morofuji1, Tomonori Ono1, Wataru Haraguchi1, Kazuya Honda2, Tomoya Moritsuka2, Keisuke Tsutsumi1. Unruptured cerebral aneurysms with the segmental duplicated middle cerebral artery formed a fenestrated structure at origin. 29-Jan-2022;13:33. Available from: https://surgicalneurologyint.com/surgicalint-articles/11363/
Date of Submission
04-Nov-2021
Date of Acceptance
08-Jan-2022
Date of Web Publication
29-Jan-2022
Abstract
Background: Middle cerebral artery (MCA) has a significantly lower incidence of anatomical variations than other intracranial arteries. We present an extremely rare case of unruptured aneurysms with the segmental duplicated MCA (d-MCA) formed a fenestrated structure at origin.
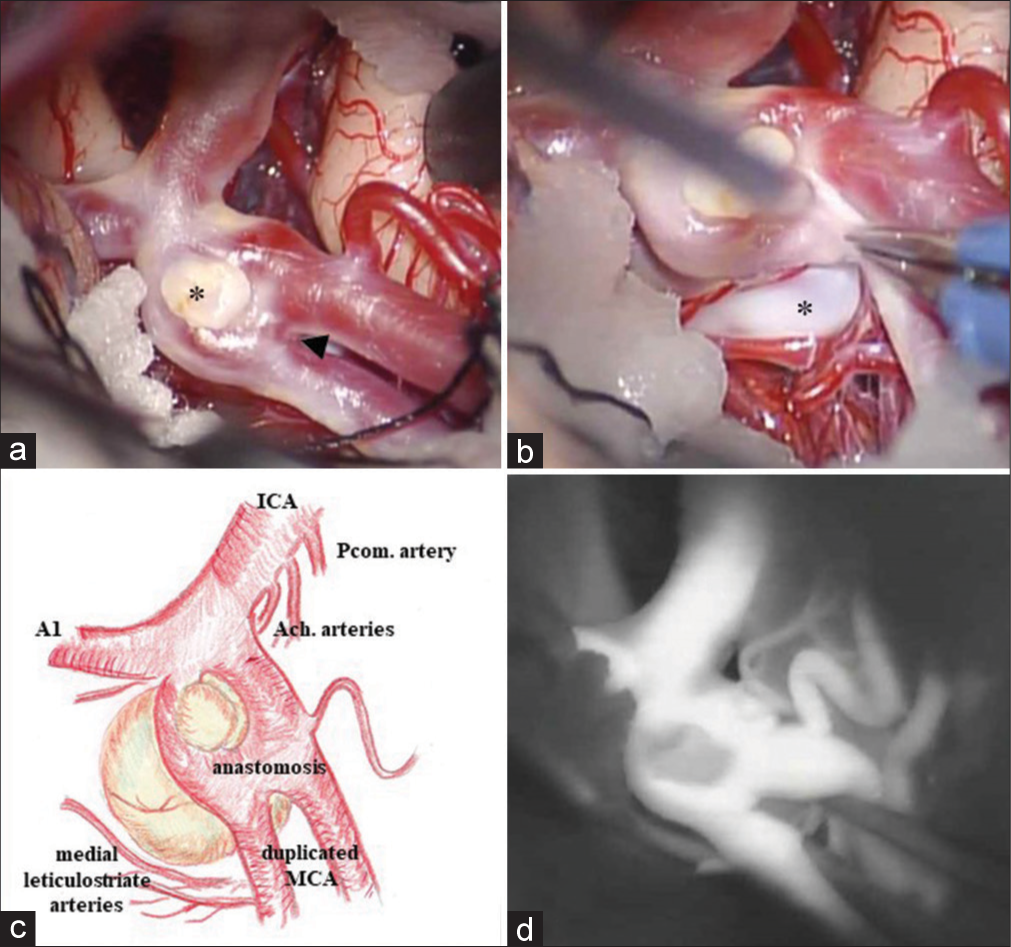
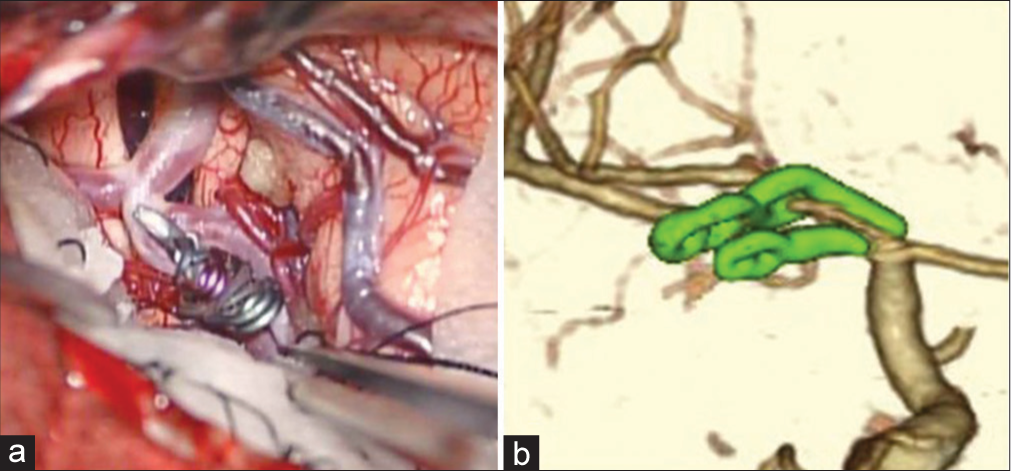
Case Description: A 55-year-old female underwent direct surgery for the unruptured aneurysms at the top of the right internal cerebral artery with d-MCA. The d-MCA branches separated at the right internal cerebral artery top and had comparable with that of the main MCA trunk. Moreover, there was an anastomosis between the d-MCA branches. We diagnosed this anastomosis as segmental d-MCA. Two aneurysmal domes were identified during surgery at the origin of the d-MCA, which the main dome protruding backward was wide necked and another small one was collapsed or thrombosed protruding forward. We used a fenestrated clip for the posterior projecting dome, and the aneurysms were successfully obliterated.
Conclusion: Although cerebral aneurysms associated with d-MCA are rare, there are technical difficulties in the surgical management. A fenestrated clip might be most reasonable to obtain patency of the parent arteries for the posterior projecting aneurysms if the perforators can be avoided.
Keywords: Anastomosis, Cerebral aneurysm, Fenestrated clip, Segmental duplicated middle cerebral artery
INTRODUCTION
Anomalies of the middle cerebral artery (MCA) occur less frequently than those of other major intracranial arteries.[
CASE DESCRIPTION
A 55-year-old woman, right handed with hypertension presented with chronic headache. The patient was smoker and had no family history of stroke. Magnetic resonance imaging suspected an unruptured aneurysm at the top of the right ICA [
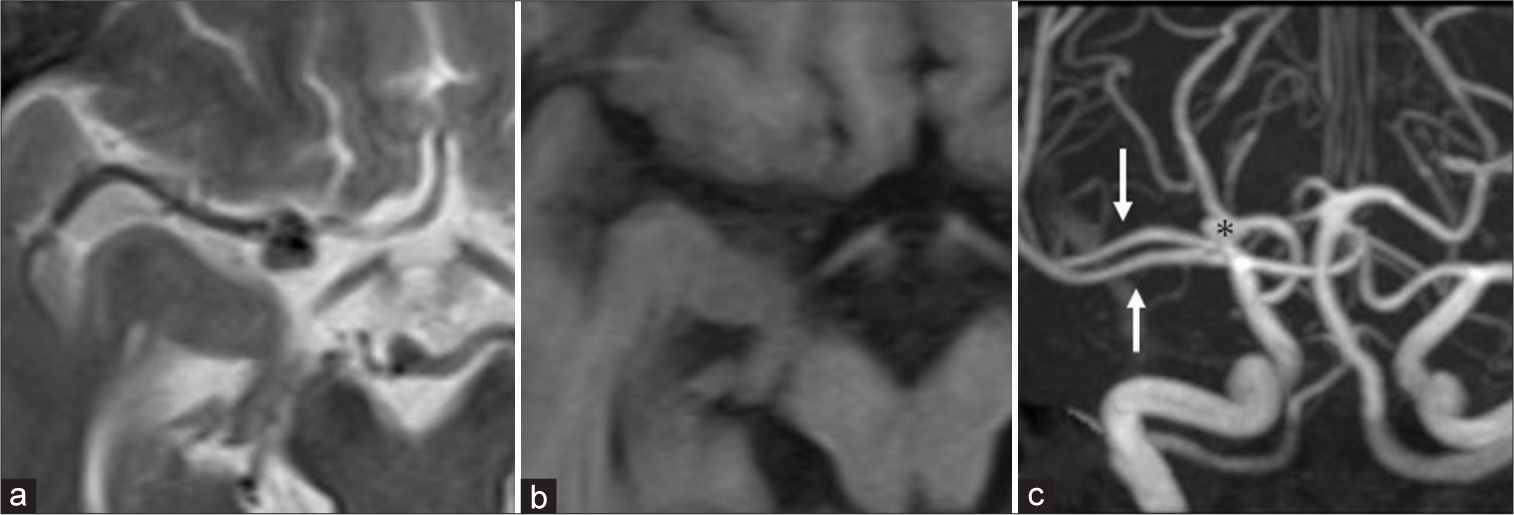
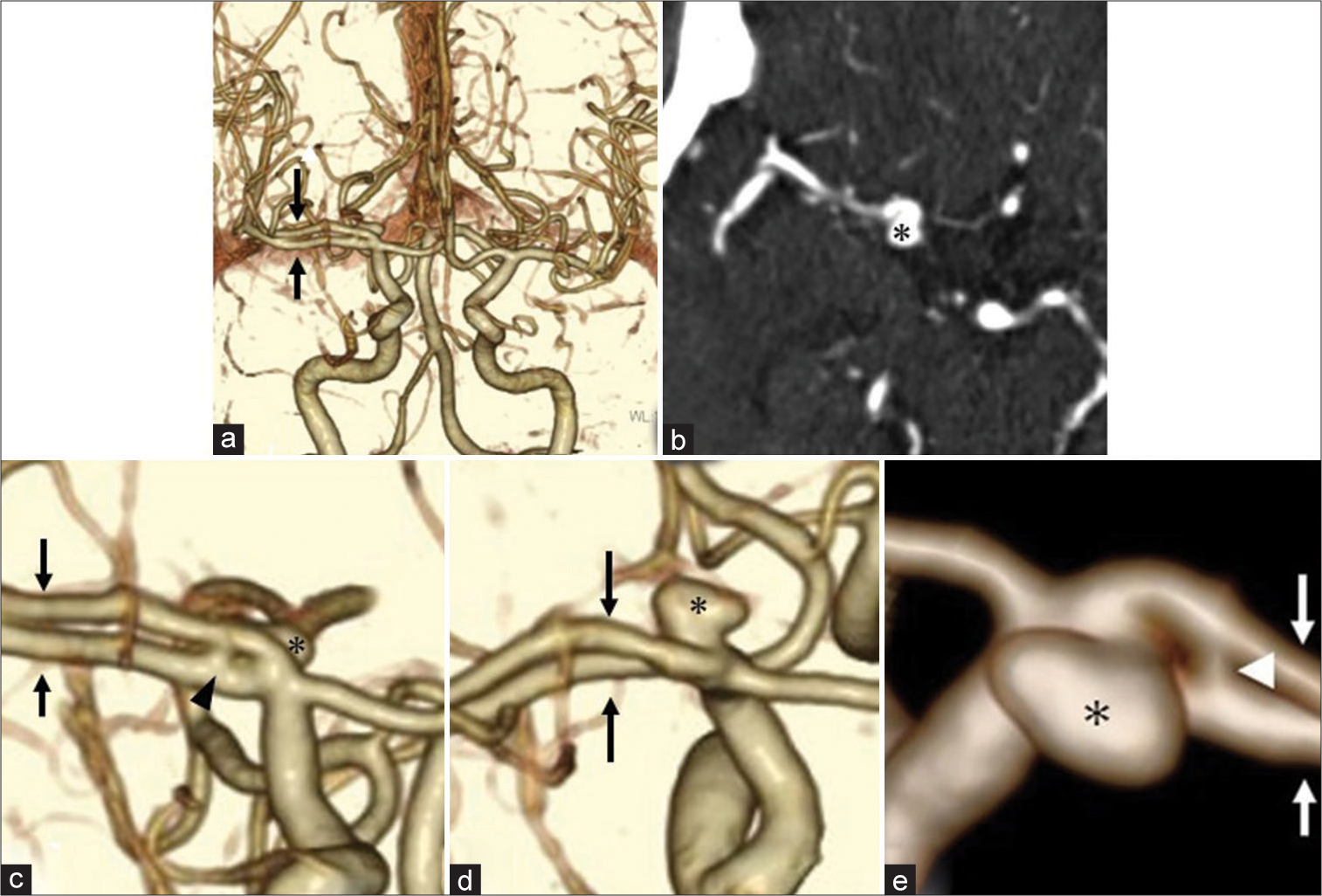
Figure 2:
Computed tomographic angiography (CTA) demonstrates an aneurysm protruding backward (asterisk) and the duplicated middle cerebral artery (d-MCA) branches (arrows). There is an anastomosis (arrowhead) between d-MCA branches at the origin (a, c-e: three-dimensional CTA, b: source imaging of CTA).
DISCUSSION
The most frequent anatomical variations of the MCA are accessory MCA (ac-MCA), d-MCA, duplicate origin of MCA (do-MCA), MCA fenestration, and twig-like MCA.[
In 1973, Teal et al. proposed the term ac-MCA as arterial branches arising from ACA or anterior communicating artery coursed with the MCA into the Sylvian fissure, and termed d-MCA as anomalous MCA arising from the ICA regardless of its size.[
The present case is the type A d-MCA and could be actually ICA trifurcation, since the d-MCA and ACA branches had almost identical diameters.[
The mechanism of the development of MCA anomaly associated aneurysms is an interesting issue and some authors have suggested that hemodynamic stress at the origin of the abnormal vessel might contribute to the formation of the aneurysm.[
The d-MCA has perforating arteries to the anterior perforated substance and may contribute to the normal cerebral blood flow to the frontal lobe and the basal ganglia through the perforating arteries.[
CONCLUSION
We experienced a rare case of the aneurysms at the origin of the segmental d-MCA. Although cerebral aneurysms associated with d-MCA are rare, there are technical difficulties in the surgical management. Fenestrated clips might be suitable to obtain patency of parent arteries.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Crompton MR. The pathology of ruptured middle-cerebral aneurysms with special reference to the differences between the sexes. Lancet. 1962. 2: 421-5
2. Elsharkawy A, Ishii K, Niemelä M, Kivisaari R, Lehto H, Hernesniemi J. Management of aneurysms at the origin of duplicated middle cerebral artery: Series of four patients with review of the literature. World Neurosurg. 2013. 80: e313-8
3. Hou K, Xu K, Liu H, Li G, Yu J. The clinical characteristics and treatment considerations for intracranial aneurysms associated with middle cerebral artery anomalies: A systematic review. Front Neurol. 2020. 11: 564797
4. Kai Y, Hamada J, Morioka M, Yano S, Kudo M, Kuratsu J. Treatment of unruptured duplicated middle cerebral artery aneurysm: Case report. Surg Neurol. 2006. 65: 190-3
5. Kaliaperumal C, Jain N, McKinstry CS, Choudhari KA Carotid. “trifurcation” aneurysm: Surgical anatomy and management. Clin Neurol Neurosurg. 2007. 109: 538-40
6. Komiyama M, Nakajima H, Nishikawa M, Yasui T. Middle cerebral artery variations: Duplicated and accessory arteries. AJNR Am J Neuroradiol. 1998. 19: 45-9
7. Padget DH. The development of the cranial arteries in the human embryo. Contrib Embryol. 1948. 32: 205-62
8. Stojanović NN, Kostić A, Mitić R, Berilažić L. Correlation between multiple cerebral aneurysms and a rare type of segmental duplication of the middle cerebral artery. BMC Neurol. 2020. 20: 3
9. Teal JS, Rumbaugh CL, Bergeron RT, Segall HD. Anomalies of the middle cerebral artery: Accessory artery, duplication, and early bifurcation. Am J Roentgenol Radium Ther Nucl Med. 1973. 118: 567-75
10. Uchiyama N. Anomalies of the middle cerebral artery. Neurol Med Chir (Tokyo). 2017. 57: 261-6

