

- Department of Neurosurgery, Medical Faculty, Universitas Airlangga, Dr. Soetomo General Hospital, Surabaya Neuroscience Institute, Surabaya, Indonesia
- Faculty of Medicine, Universitas Airlangga, Dr. Soetomo General Hospital, Surabaya Neuroscience Institute, Surabaya, Indonesia
- Department of Neurosurgery, H. Adam Malik General Hospital, Medan, Indonesia
- Department of Neurosurgery, Medical Faculty, Universitas Sebelas Maret, Dr. Moewardi General Hospital, Surakarta, Indonesia
Correspondence Address:
Asra Al Fauzi
Department of Neurosurgery, Medical Faculty, Universitas Sebelas Maret, Dr. Moewardi General Hospital, Surakarta, Indonesia
DOI:10.4103/sni.sni_138_17
Copyright: © 2017 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Asra Al Fauzi, Wihasto Suryaningtyas, Joni Wahyuhadi, M. Arifin Parenrengi, Agus Turchan, Maria C. Wijaya, Michael Jonatan, Mahyudanil, Hanis Setyono. Upward migration and peroral extrusion of a peritoneal shunt catheter: Case report and review of the literature. 09-Aug-2017;8:178
How to cite this URL: Asra Al Fauzi, Wihasto Suryaningtyas, Joni Wahyuhadi, M. Arifin Parenrengi, Agus Turchan, Maria C. Wijaya, Michael Jonatan, Mahyudanil, Hanis Setyono. Upward migration and peroral extrusion of a peritoneal shunt catheter: Case report and review of the literature. 09-Aug-2017;8:178. Available from: http://surgicalneurologyint.com/surgicalint-articles/upward-migration-and-peroral-extrusion-of-a-peritoneal-shunt-catheter-case-report-and-review-of-the-literature/
Date of Submission
11-Apr-2017
Date of Acceptance
24-May-2017
Date of Web Publication
09-Aug-2017
Abstract
Background:Various complications after ventriculoperitoneal (VP) shunt surgery have been reported, but peroral extrusion of peritoneal catheter is an extremely rare complication, and only 20 cases have been reported since 1987. The pathophysiology still remains unclear and the management is challenging.
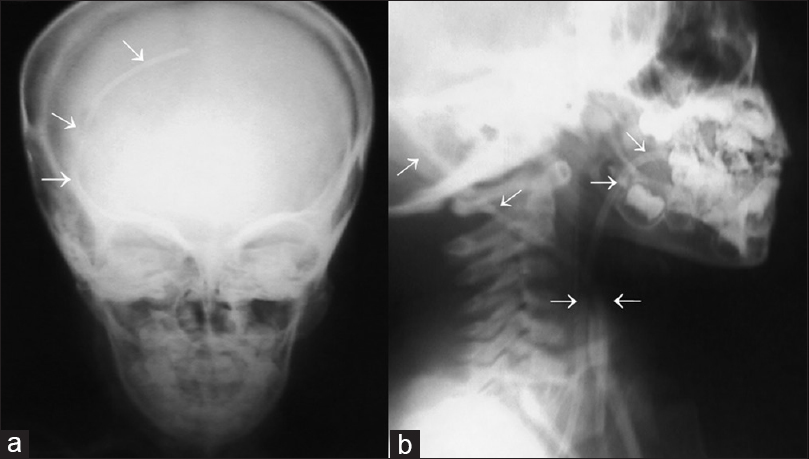
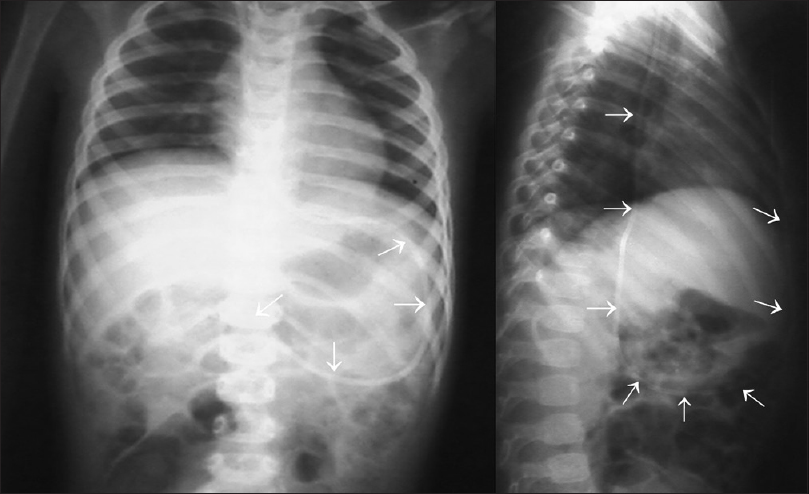
Case Description:A 5-year-old boy presented with a catheter coming out of his mouth. The boy had a posterior fossa tumor surgery and had VP shunt insertion 1 year earlier. Clinical signs and imaging studies showed that the distal end of the catheter had perforated the gaster and migrated upward and extruded through the mouth. Emergency removal of the shunt and proper treatment were done and he made uneventful recovery.
Conclusion:Peroral extrusion of VP shunt is extremely rare. Clinicians should be aware of this complication. With early diagnosis and proper management, the prognosis for good recovery is excellent, with only two deaths being reported in the literature. Complication of shunt extrusion is difficult to avoid, but knowing the risk factors, pathophysiology and proper management will decrease the morbidity and mortality of such cases.
Keywords: Management, patophysiology, peroral extrusion, risk factors, VP shunt
INTRODUCTION
Ventriculoperitoneal (VP) shunt is the most widely used procedure to treat hydrocephalus.[
CASE HISTORY
A 5-year-old boy presented with peroral extrusion at the distal end of a VP shunt catheter. The boy had been diagnosed by magnetic resonance imaging as having posterior fossa tumor and hydrocephalus when aged 4 years. A surgery was performed and VP shunt catheter was inserted using a Chhabra-slit-in-spring silicone shunt system. After the surgery, the patient remained well with the exception of mild gait disturbance. One week before admission to our hospital, the boy complaint of upper abdominal discomfort with emesis. In the following day, he regurgitated and severed peritoneal catheter exiting through the mouth.
Examination
At the time of admission, the boy was afebrile and fully conscious. We found no evidence of meningitis or increased intracranial pressure. The abdomen was soft and bowel sounds were normal. There was no sign of inflammation along the shunt tract. The peritoneal catheter was found extruding from his mouth [

Treatment
The boy underwent emergency shunt removal. During intubation the distal catheter was seen coming out of the esophagus. Surgical incision was made in the previous scar in the scalp and in median abdomen. The distal catheter was cut at the abdomen site before entering the peritoneal cavity. The ventricular catheter was disconnected from the chamber, and there was a flow of CSF from the ventricular catheter. Analysis of the CSF did not reveal any sign of infection. The ventricular end and the chamber were removed through the scalp incision, and part of the distal catheter under thoracic tract was removed through the median abdomen incision. The distal catheter in peritoneal cavity, which had perforated the stomach wall, was removed easily by pulling out through the opening of the mouth. We removed the whole catheter and observed the patient for 3 days. External drainage was not performed. The boy was nil peroral and maintained on intravenous fluids and antibiotics for 3 days. During the observation there was no sign of meningitis or peritonitis. There was no signs and symptoms of increased intracranial pressure, which meant the boy had become shunt independent, thereby no replacement shunt system was required. After 5 days of treatment, the boy was discharged in satisfactory condition and is currently doing well.
DISCUSSION
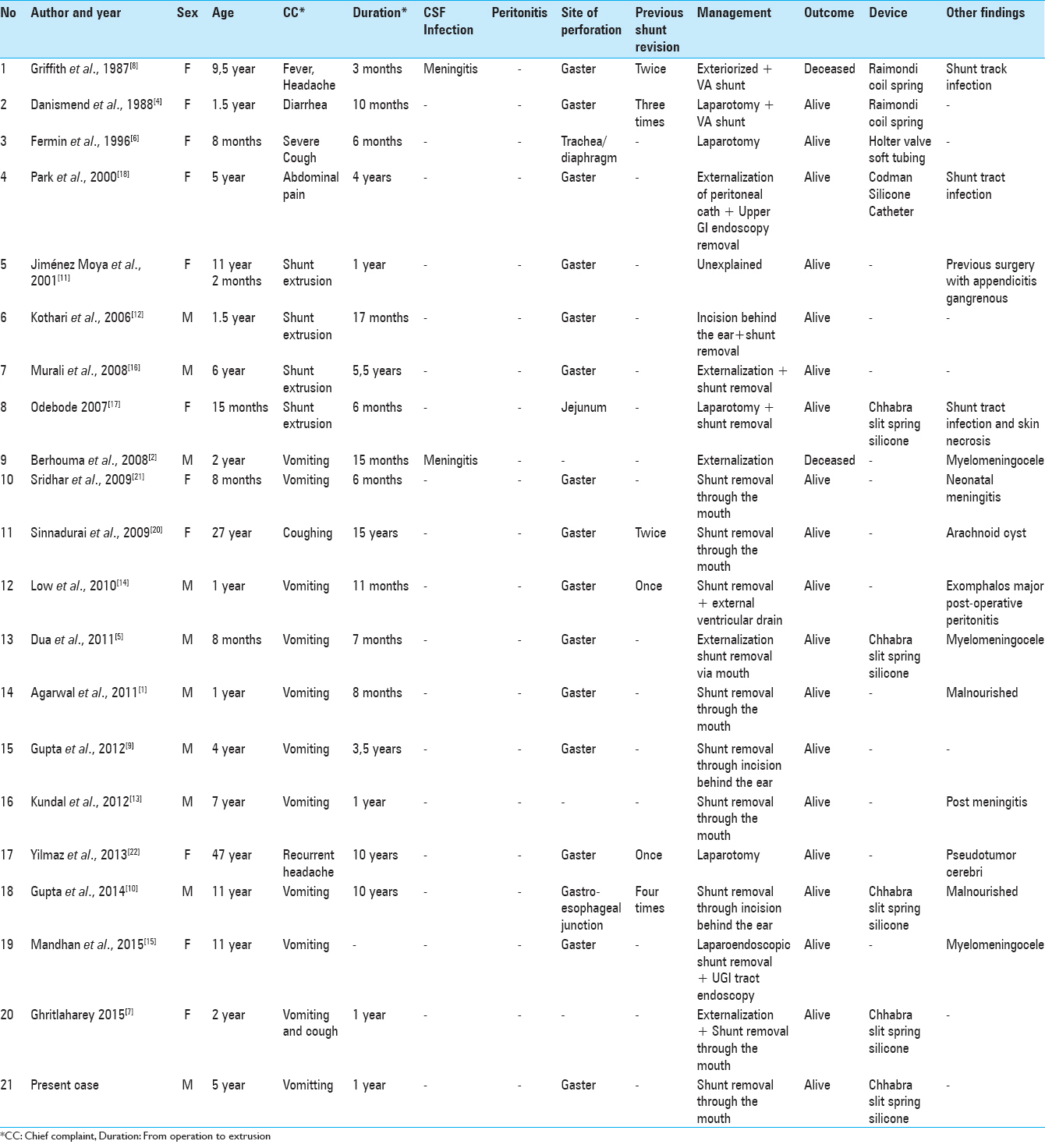
We conducted literature search of all cases of peroral extrusion of a VP catheter shunt via PubMed and MEDLINE, and identified 20 cases (excluding the present case) of peroral extrusion of a VP shunt catheter, which are summarized in
Pathophysiology
According to our case literatures review, all had a delayed presentation, which meant that the perforation is caused by a chronic process rather than acute injury (e.g., during the procedure). An important part of the pathophysiology of perforation is local inflammation and repeated pressure on the bowel wall. Inflammation leads to formation of an encasing fibrosis, which anchored the catheter to the serosal surface of the bowel wall. The site of catheter adherence to the bowel wall is then subjected to repeated pressure, due to the “pushing” effect of intestinal movements,[
Risk factors
The etiology of migration and extrusion of a VP shunt catheter has not been fully understood. From the literatures that we have reviewed, we identified the risk factors associated with extrusion of the peritoneal catheter and divided them into internal (ensuing from the host) and external factors. Internal factors include: (1) age, (2) nutritional status, (3) bioreactivity, (4) previous abdominal surgery and (5) chronic immobilization. Younger age has been mentioned as a prominent risk factor for bowel perforation in much literatures,[
External factors include: (1) surgical error, (2) infection, (3) shunt type, and (4) shunt length. Perforation caused by surgical error is mainly associated with an acute presentation, which was not shown in any of the cases we reviewed. Surprisingly, from our review of the literature, no cases presented clinically with peritonitis, and 2 out of 21 (9.5%) presented with CSF infection, which led to a grave outcome as both patients are deceased. A proposed explanation for the low number of infection is a protective mechanism by the fibrous encasement of the catheter which prevented extension of infection from the bowel to the peritoneal cavity. Then again, many of the cases we reviewed have gaster as the site of perforation, which had a lower number of bacterial colonization compared to other sites of the bowel, such as the colon. Infection of the shunt tract itself may contribute through a mechanism which is similar to silicone allergy or mechanical irritation, eventually leading to local inflammation by means of foreign body reaction.[
Management
From the literature we have reviewed, our recommendation for the principles of treatment for shunt catheter perforation with peroral extrusion is: (1) emergency removal, (2) appropriate antibiotic therapy, (3) nil per oral, (4) reinsertion (if necessary). Emergency removal can be performed by open laparotomy, endoscopy, or pulling the catheter manually through the mouth. Earlier cases tend to choose open laparotomy as a method of removal, because laparotomy aided in visualization of any opening in the bowel caused by perforation that might need primary closure.[
Infection control is an important part of the management of this complication. Our case emphasizes the importance of confirming early presence of infection. Broad spectrum antibiotics that cover the intestinal flora should be started at the time of admission. The risk of contamination during removal of the catheter should be minimized, by performing removal of the catheter with minimally invasive procedure and under antibiotic cover.[
Keeping the patient nil per oral is necessary for the healing process in bowel perforation cases. Recommendation for nil per orally management in our case is three days for recovery of the bowel. Several previous reports, recommendations for fasting after treatment vary greatly, mostly between 2 and 4 days.[
The patient might not need a replacement shunt because they might have become shunt independent, probably because their CSF pathway has already healed from the time of shunt placement or the primary cause has been corrected.[
Outcome
From the literature we get on the case of VP shunt complications with peroral extrusion; almost all the outcome is good. Only two cases of deaths were reported as a result of complication of meningitis. With proper management, the case could provide an optimal outcome with minimal morbidity.
CONCLUSION
Upward migration and peroral extrusion of VP shunt is extremely rare. Clinicians should be aware of this complication with early diagnosis and proper management. The best management should be emergency shunt removal by pulling the distal catheter through the mouth and prevention of ascending infection. In most of the cases, the prognosis for good recovery is excellent, with only two death being reported in the literature. The mortality cases were associated with complication of meningitis. Complication of shunt extrusion is difficult to avoid, but knowing the risk factors, pathophysiology and proper management will decrease the morbidity and mortality of such cases.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Agarwal M, Adhana R, Namdev H, Yadav YR, Agrawal T. Transoral extrusion of the ventriculo-peritoneal shunt: A case report and review of literature. J Pediatr Neurosci. 2011. 6: 149-51
2. Berhouma M, Messerer M, Houissa S, Khaldi M. Transoral protrusion of a peritoneal catheter: A rare complication of ventriculoperitoneal shunt. Pediatr Neurosurg. 2008. 44: 169-71
3. Brownlee JD, Brodkey JS, Schaefer IK, Mostello L, Robson M, Heggers J. Colonic perforation by ventriculoperitoneal shunt tubing: A case of suspected silicone allergy. Surg Neurol. 1998. 49: 21-4
4. Danismend N, Kuday C. Unusual complication of ventriculoperitoneal shunt. Neurosurgery. 1988. 22: 798-
5. Dua R, Jain R. Peroral extrusion of ventriculoperitoneal shunt: A case report and review of the literature. Cent Eur Neurosurg. 2011. 72: 107-8
6. Fermin S, Fernández-Guerra RA, Sureda PJ. Extrusion of peritoneal catheter through the mouth. Childs Nerv Syst. 1996. 12: 553-5
7. Ghritlaharey RK. Review of the Management of Peroral Extrusion of Ventriculoperitoneal Shunt Catheter. J Clin Diagn Res. 2016. 10: PE01-6
8. Griffith JA, DeFeo D. Peroral extrusion of a ventriculoperitoneal shunt catheter. Neurosurgery. 1987. 21: 259-61
9. Gupta M, Digra NC, Sharma N, Goyal S, Agrawal A. Peroral extrusion of the peritoneal catheter in an infant. N Am J Med Sci. 2012. 4: 290-1
10. Gupta R, Mala TA, Gupta A, Paul R, Malla SA, Gupta AK. Transoral migration of peritoneal end of ventriculoperitoneal shunt with perforation of gastro-esophageal junction: A case report of a rare complication. Bangladesh J Med Sci. 2014. 13: 492-5
11. Jiménez Moya A, Penela Vélez De Guevara T, Gracia Remiro R, Romero Escós D, Santana Rodríguez C, Reig Del Moral C. Extrusion of a ventriculoperitoneal shunt catheter through the mouth. An Esp Pediatr. 2001. 54: 609-10
12. Kothari P, Shankar G, Kulkarni B. Extruded ventriculo-peritoneal shunt: An unusual complication. J Indian Assoc Pediatr Surg. 2006. 11: 255-6
13. Kundal VK, Gajdhar M, Sharma C, Agrawal D, Kundal R. Wandering distal end of ventriculoperitoneal shunt: Our experience with five cases and review of literature. J Nepal Paediatr Soc. 2013. 32: 266-9
14. Low SW, Sein L, Yeo TT, Chou N. Migration of the abdominal catheter of a ventriculoperitoneal shunt into the mouth: A rare presentation. Malays J Med Sci. 2010. 17: 64-7
15. Mandhan P, Wong M, Samarakkody U. Laparoendoscopic removal of peroral extrusion of a ventriculoperitoneal shunt. Asian J Endosc Surg. 2015. 8: 95-7
16. Murali R, Ravikumar V. Transoral migration of peritoneal end of ventriculoperitoneal shunt: A case report of a rare complication and review of literature. J Pediatr Neurosci. 2008. 3: 166-8
17. Odebode TO. Jejunal perforation and peroral extrusion of a peritoneal shunt catheter. Br J Neurosurg. 2007. 21: 235-6
18. Park C-K, Wang K-C, Seo JK, Cho B-K. Transoral protrusion of a peritoneal catheter: A case report and literature review. Child's Nerv Syst. 2000. 16: 184-9
19. Sathyanarayana S, Wylen EL, Baskaya MK, Nanda A, Bando Y, Manabe Y. Spontaneous bowel perforation after ventriculoperitoneal shunt surgery: Case report and a review of 45 cases. Surg Neurol. 2000. 54: 388-96
20. Sinnadurai M, Winder MJ. Silicone spaghetti. J Clin Neurosci. 2009. 16: 1348-50
21. Sridhar K, Karmarkar V. Peroral extrusion of ventriculoperitoneal shunt: Case report and review of literature. Neurol India. 2009. 57: 334-6
22. Yilmaz MB, Egemen E, Tonge M, Kaymaz M. Transoral protrusion of a peritoneal catheter due to gastric perforation 10 years after a ventriculoperitoneal shunting – Case report and review of the literature. Turk Neurosurg. 2011. 23: 285-8

