

- Department of Neurosurgery, Moriyama Memorial Hospital, Tokyo, Japan
Correspondence Address:
Atsushi Ishida
Department of Neurosurgery, Moriyama Memorial Hospital, Tokyo, Japan
DOI:10.4103/2152-7806.187494
Copyright: © 2016 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Ishida A, Matsuo S, Asakuno K, Nemoto A, Niimura K, Yoshimoto H, Shiramizu H, Ubagai R, Yuzawa M, Hori T. Utility of crankshaft clips for middle cerebral artery aneurysms: A single-center experience of 150 cases. Surg Neurol Int 01-Aug-2016;7:
How to cite this URL: Ishida A, Matsuo S, Asakuno K, Nemoto A, Niimura K, Yoshimoto H, Shiramizu H, Ubagai R, Yuzawa M, Hori T. Utility of crankshaft clips for middle cerebral artery aneurysms: A single-center experience of 150 cases. Surg Neurol Int 01-Aug-2016;7:. Available from: http://surgicalneurologyint.com/surgicalint_articles/utility-crankshaft-clips-middle-cerebral-artery-aneurysms-single%e2%80%91center-experience-150-cases/
Abstract
Background:Applying more than one clip for a complicated-shaped aneurysm is an established strategy, particularly for middle cerebral arteries (MCA). However, obliterating the cleft of the internal elastic lamina with a single clip is theoretically possible because the line is usually on a single plane. Crankshaft clips were reformed for that purpose decades ago, but are not widely used and have been described in almost no report ever since.
Methods:To reconsider and describe the utility of crankshaft clips for complicated MCA aneurysms and to articulate the advantages and limitations of the clips, we meticulously analyzed a series of more than 150 cases in which the crankshaft clips were used, predominantly for treatment of MCA aneurysms, at Moriyama Memorial Hospital between August 2010 and December 2015.
Results:Readjustment of the clip was not necessary in almost all cases, and the first application was the final one. None of the patients had morbidity or mortality related to the surgical technique. To date, we have not experienced any trouble or recurrence.
Conclusions:Crankshaft clips are useful and safe for clipping of complicated MCA aneurysms.
Keywords: Crankshaft clip, closure line, middle cerebral aneurysm, multiple clipping
INTRODUCTION
Despite the recent undeniable success of endovascular obliteration of intracranial aneurysms,[
Meanwhile, crankshaft clips were created by modifying a bayonet clip to occlude the thin wall or reddish bleb of the neck close to the parent artery.[
Here, we describe our experience using crankshaft clips at Moriyama Memorial Hospital between August 2010 and December 2015.
MATERIALS AND METHODS
Since 2010, advanced versions of 3 newly designed bayonet clips have become available from Elgiloy as Sugita 2 clips (crankshaft clips; manufactured by Mizuho Ikakogyo Co. Ltd., Tokyo, Japan) [
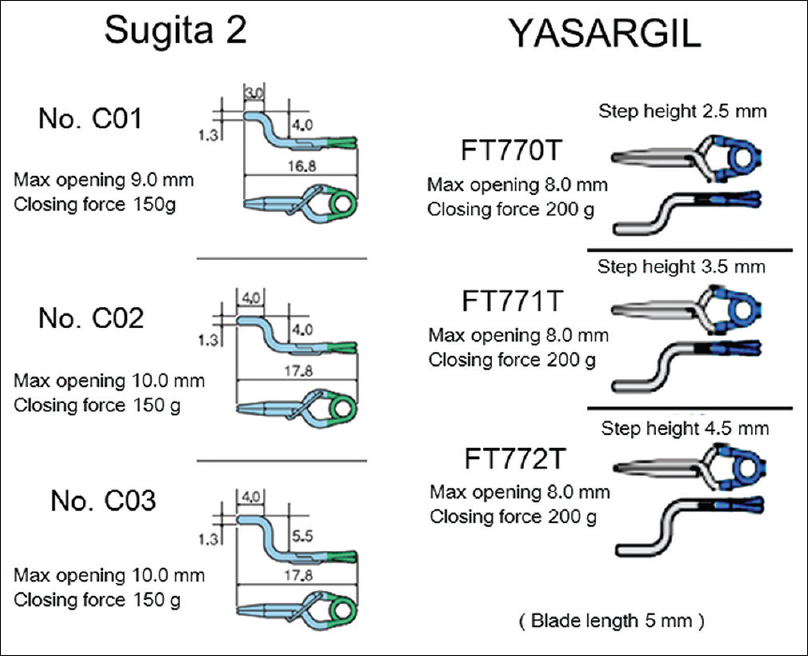
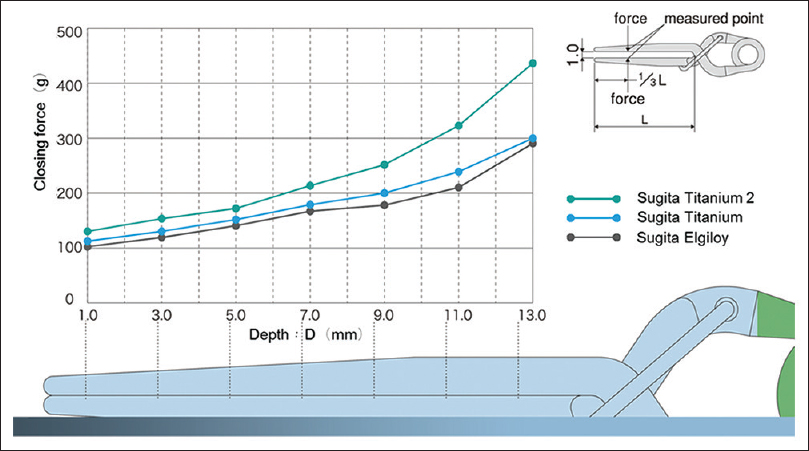
The primary difference between the former clips and the newer titanium clips is the constituent. Therefore, in terms of the opening width of the crankshaft clips, Sugita clips are more advantageous. The purpose of the crankshaft clip is to occlude the thin wall or reddish bleb with its shank portion because these parts are the most likely future origin of bleeding, and therefore, should be closed completely. Mizuho reported a graph showing the comparison between closing force and depth of Sugita clips in their official site.[
We examined a series of 150 cases in which crankshaft clips were used at Moriyama Memorial Hospital between August 2010 and December 2015. Of the 150 cases, 146 (96%) were MCA aneurysms, and of the remaining 6, there were 4 anterior communicating artery (ACOM) aneurysms, 1 basilar top aneurysm, and 1 distal anterior cerebral artery (ACA) aneurysm. Forty percent of the aneurysms ruptured and 70% of them occurred in women. Only cases with aneurysmal size <10 mm were included.
Ishikawa et al. described 3 different types of aneurysm configurations,[
For our cohort, final confirmation of the bifurcation type was done after meticulous exposure of the aneurysm and parent arteries. Rupture did not occur in most cases; therefore, temporary clipping or adenosine administration, used for ruptured cases only,[
RESULTS
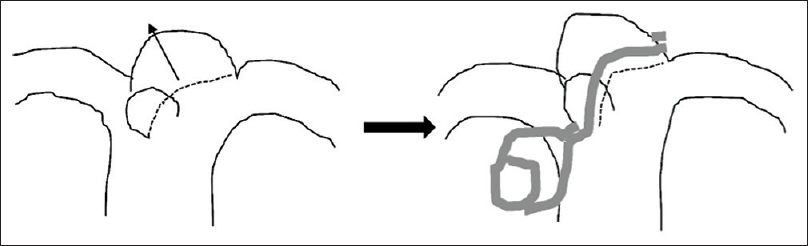
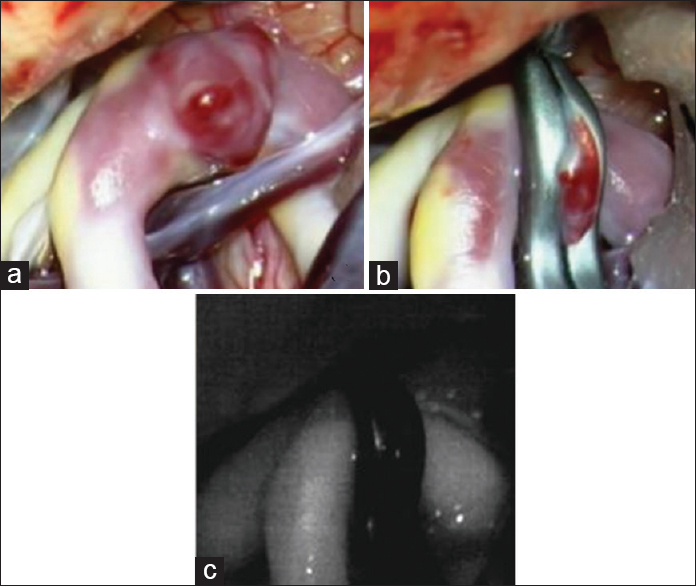
More than 150 crankshaft clips were used, predominantly for MCA aneurysms. We achieved an ideal closure line with the crankshaft clip in all cases. Two types of MCA aneurysms were closed using crankshaft clips. First, which dominated the series, has a main round dome with a thin-wall bleb [
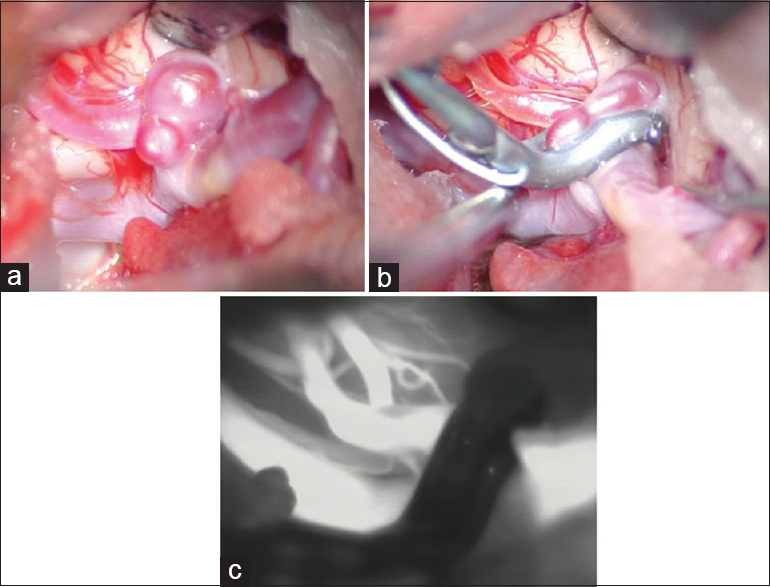
Figure 4
Illustrative case 1. (a-c) intraoperative pictures. (a) A clearly exposed right middle cerebral artery aneurysm with a bleb in front of it and its parent arteries. (b) A crankshaft clip was nicely applied. (c) Indocyanine Green angiography shows a complete clipping and patency of its parent arteries
The clip that most used was the medium-sized Sugita 2 clip (C02). This clip has a 4 mm blade and a 4 mm shank portion and fits in most cases to make an ideal closure line [Figures
DISCUSSION
Despite the recent dramatic improvement in endovascular treatment,[
Multiple clipping has been a widely used technique for complicated MCA aneurysms because the ideal closure line can be achieved with it.[
Another advantage of the crankshaft clipping compared to multiple clipping is its continuity. Regardless of how close the clips are, there still is a cleft of internal elastic lamina from which a recurrence can originate. Closing the closure line without discontinuity gives patients the best opportunity for ultimate cure of the aneurysm. Because the shank portion of the crankshaft clip has a stronger closing force, it is ideal for obliterating a fragile bleb. The closing forces of Sugita 2 clips are 150 g, measured at one-third point from the tip, however, those at the shank portion of the clips are estimated at more than 200 g because the force increases closer to its coil part.[
While crankshaft clipping is not feasible in the case of a large, atherosclerotic aneurysm, here we used the clip for large-sized (almost 10 mm) MCA aneurysms in a couple of cases. However, a single crankshaft clip was not strong enough to close the long, hard neck, and an additional “booster clip” was necessary. The “picket fence” clipping technique is a recently reported method for clipping large, atherosclerotic aneurysms using a number of parallel straight clips;[
One of the limitations of using a single crankshaft clipping is that it requires wide space because the operator should face the closure line perpendicularly for a complete obliteration. Therefore, it is useful for aneurysms located in a wider location such as MCA aneurysms in which the aneurysmal neck often includes the arterial junction. They are also useful for some ACOM aneurysms if enough space is available. In our series, the crankshaft clips were used for aneurysms in locations other than the MCA in only six cases.
SUMMARY
Crankshaft clips are useful and safe for clipping of complicated MCA aneurysms. We could make ideal closure lines with the clips by using a couple of tips. This could be an alternative method of multiple clipping technique.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Acciarri N, Toniato G, Raabe A, Lanzino G. Clipping techniques. J Neurosurg Sci. 2016. 60: 83-94
2. Last accessed on 2016 Mar 24. Available at: https://www.aesculapusa.com/products/neurosurgery/aneurysm-clips .
3. Amagasaki K, Higa T, Takeuchi N, Kakizawa T, Shimizu T. Late recurrence of subarachnoid hemorrhage due to regrowth of aneurysm after neck clipping surgery. Neurol Med Chir. 2002. 42: 496-500
4. Briganti F, Delehaye L, Leone G, Sicignano C, Buono G, Marseglia M. Flow diverter device for the treatment of small middle cerebral artery aneurysms. J Neurointerv Surg. 2016. 8: 287-94
5. Dashti R, Hernesniemi J, Niemelä M, Rinne J, Lehecka M, Shen H. Microneurosurgical management of middle cerebral artery bifurcation aneurysms. Surg Neurol. 2007. 67: 441-56
6. Davies JM, Lawton MT. “Picket Fence” clipping technique for large and complex aneurysms. Neurosurg Focus. 2015. 39: V17-
7. Hallout S. Surgical treatment of middle cerebral artery aneurysms without using indocyanine green videoangiography assistance: Retrospective monocentric study of 263 clipped aneurysms. World Neurosurg. 2015. 84: 972-7
8. Ikeda DS, Marlin ES, Shaw A, Powers CJ. Successful endovascular reconstruction of a recurrent giant middle cerebral artery aneurysm with multiple telescoping flow diverters in a pediatric patient. Pediatr Neurosurg. 2015. 50: 88-93
9. Ishida A, Matsuo S, Asakuno K, Nemoto A, Niimura K, Yoshimoto H. Rebleeding from clipped aneurysm after 35 years Report of 2 cases. Surg Neurol Int. 2015. 6: 134-
10. Ishikawa T. Clipping techniques for cerebral aneurysms. Special consideration for closure line and application angle. No Shinkei Geka Sokuho. 2007. 17: 804-14
11. Ishikawa T, Nakayama N, Moroi J, Kobayashi N, Kawai H, Muto T. Concept of ideal closure line for clipping of middle cerebral artery aneurysms--Technical note. Neurol Med Chir. 2009. 49: 273-7
12. Jeon HJ, Kim SY, Park KY, Lee JW, Huh SK. Ideal clipping methods for unruptured middle cerebral artery bifurcation aneurysms based on aneurysmal neck classification. Neurosurg Rev. 2016. 39: 215-24
13. Kalakoti P, Bir SC, Murray RD, Ahmed O, Nanda A. Technical nuances of clipping a middle cerebral artery bifurcation aneurysm. Neurosurg Focus. 2015. 39: V2-
14. Kashimura H, Ogasawara K, Kubo Y, Ogawa A. Complete neck clipping of internal carotid-posterior communicating artery aneurysms using bayonet-shaped aneurysm clips: Technical note. Neurol Med Chir. 2007. 47: 282-4
15. Kato Y, Sano H, Kanaoka N, Hayakawa M, Iritani K, Katada K. Mechanism and prevention of enlargement or new development of aneurysm following treatment by clipping or coiling. Neurol Res. 2000. 22: 692-8
16. Kiran NA, Jahromi BR, Velasquez JC, Hijazy F, Goehre F, Kivisaari R. Double-clip technique for the microneurosurgical management of very small (<3 mm) intracranial aneurysms. Neurosurgery. 2015. 11: 3-7
17. Lescher S, du Mesnil de Rochemont R, Berkefeld J. Woven Endobridge (WEB) device for endovascular treatment of complex unruptured aneurysms-A single center experience. Neuroradiology. 2016. 58: 383-90
18. Nussbaum ES, Erickson DL. The fate of intracranial microaneurysms treated with bipolar electrocoagulation and parent vessel reinforcement. Neurosurgery. 1999. 45: 1174-5
19. Osawa M, Obinata C, Kobayashi S, Tanaka Y. Newly designed bayonet clips for complicated aneurysms: Technical note. Neurosurgery. 1995. 36: 425-6
20. Ota N, Tanikawa R, Noda K, Tsuboi T, Kamiyama H, Tokuda S. The efficiency of the new Yasargil titanium fenestrated mini-clips for ideal clipping of a cerebral aneurysm. Surg Neurol Int. 2015. 23: S553-9
21. Sano H. Treatment of complex intracranial aneurysms of anterior circulation using multiple clips. Acta Neurochir Suppl. 2010. 107: 27-31
22. Smith TR, Cote DJ, Dasenbrock HH, Hamade YJ, Zammar SG, El Tecle NE. Comparison of the efficacy and safety of endovascular coiling versus microsurgical clipping for unruptured middle cerebral artery aneurysms: A systematic review and meta-analysis. World Neurosurg. 2015. 84: 942-53
23. Steklacova A, Bradac O, Charvat F, De Lacy P, Benes V. “Clip first” policy in management of intracranial MCA aneurysms: Single-centre experience with a systematic review of literature. Acta Neurochir. 2016. 158: 533-46
24. Last accessed on 2016 Mar 24. Available at: http://www.mizuhomedical.co.jp/products/?id=1345513487.2246 .

