

- Department of Neurosurgery, State University of New York Upstate Medical University, Syracuse, New York, United States.
DOI:10.25259/SNI_9_2020
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Haydn Hoffman, Carlos R. Goulart, Michael A. Galgano. Utilizing vertebral body autograft for anterior cervical corpectomy/fusion. 18-Feb-2020;11:24
How to cite this URL: Haydn Hoffman, Carlos R. Goulart, Michael A. Galgano. Utilizing vertebral body autograft for anterior cervical corpectomy/fusion. 18-Feb-2020;11:24. Available from: https://surgicalneurologyint.com/surgicalint-articles/9874/
Date of Submission
07-Jan-2020
Date of Acceptance
16-Jan-2020
Date of Web Publication
18-Feb-2020
Abstract
Background:There are numerous ways to reconstruct cervical vertebral bodies and achieve arthrodesis following anterior cervical corpectomy and fusion (ACF). However, device and donor site complications abound. Here, we describe a novel technique for performing ACF using the vertebral body itself as a structural autograft.
Methods: The anterior cervical spine was accessed and discectomies were performed rostral and caudal to the corpectomy. Five millimeter troughs were drilled on the lateral borders of the vertebral body, and it was removed en bloc. The autograft was rotated 90°, and an anterior cervical plate was selected to span the length of the graft, allowing for fixation to the adjacent vertebral bodies. The plate was secured to the graft, the graft was placed in the bony defect, and the plate was secured to the adjacent levels.
Results: This corpectomy reconstructive technique was successfully applied in a 57-year-old female with cervical myelopathy due to a C5–C6 disc herniation with caudal migration. The C6 vertebral body was used as a structural autograft. Postoperatively, the patient experienced satisfactory improvement in her myelopathy, and the construct appeared stable 8 months later.
Conclusion:This corpectomy reconstructive technique takes advantage of the favorable osteogenic properties of autograft, while avoiding donor site morbidity as well as the cost and complications of other devices, such as cages. Further cases are required to verify the safety, efficacy, and biomechanical stability of this technique.
Keywords: Autograft, Cervical spine, Corpectomy
INTRODUCTION
Anterior cervical corpectomy and fusion (ACF) requires reconstruction of the vertebral body defect utilizing a variety of autografts, allografts, and devices. Autograft reconstruction has been studied extensively and yields superior fusion rates and lower incidence of graft collapse than allograft.[
TECHNIQUE
Illustrative case
A 57-year-old female presented with cervical myelopathy (Nurick Grade 4) attributed to a magnetic resonance imaging documented large C5–C6 disc herniation with caudal migration [
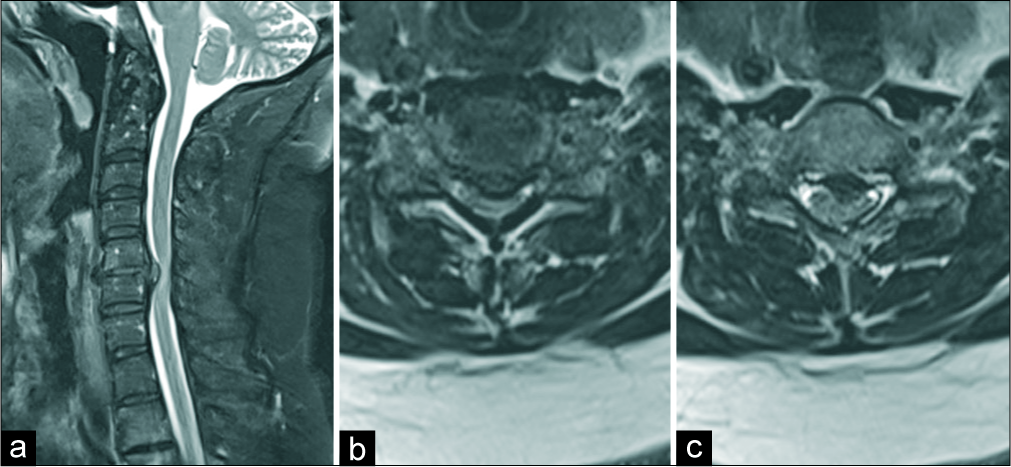
Figure 1:
(a) Sagittal and (b) axial T2-weighted magnetic resonance imaging (MRI) at the level of the C5–C6 disc space demonstrate a large C5–C6 disc herniation causing spinal cord compression. (c) Additional axial T2-weighted MRI at the level of the mid-C6 vertebral body demonstrates the caudal migration of the herniated disc.
Operative technique
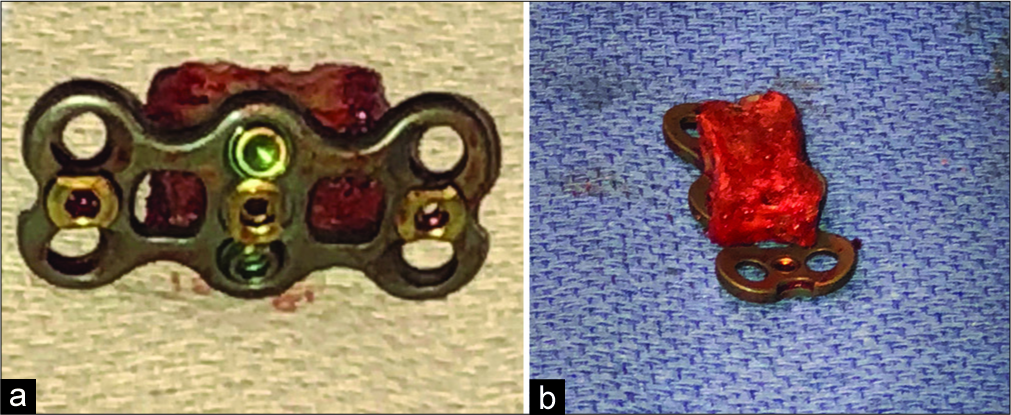
Following routine anterior cervical exposure of the C5, C6, and C7 vertebral bodies, discectomies were performed rostral and caudal to the level of the corpectomy. Five millimeter troughs were drilled laterally in the C6 body just medial to the uncovertebral joints. This allowed the body to be freed and removed en bloc. The vertebral body was cleaned of soft tissue in the preparation for use as a structural autograft. The autograft was then rotated 90 degrees, affixed to an appropriate 37.5 mm anterior cervical plate with 11 mm variable screws, and secured to the cephalad C5 and caudal C7 vertebral bodies with 14 mm variable screws [
Postoperative course
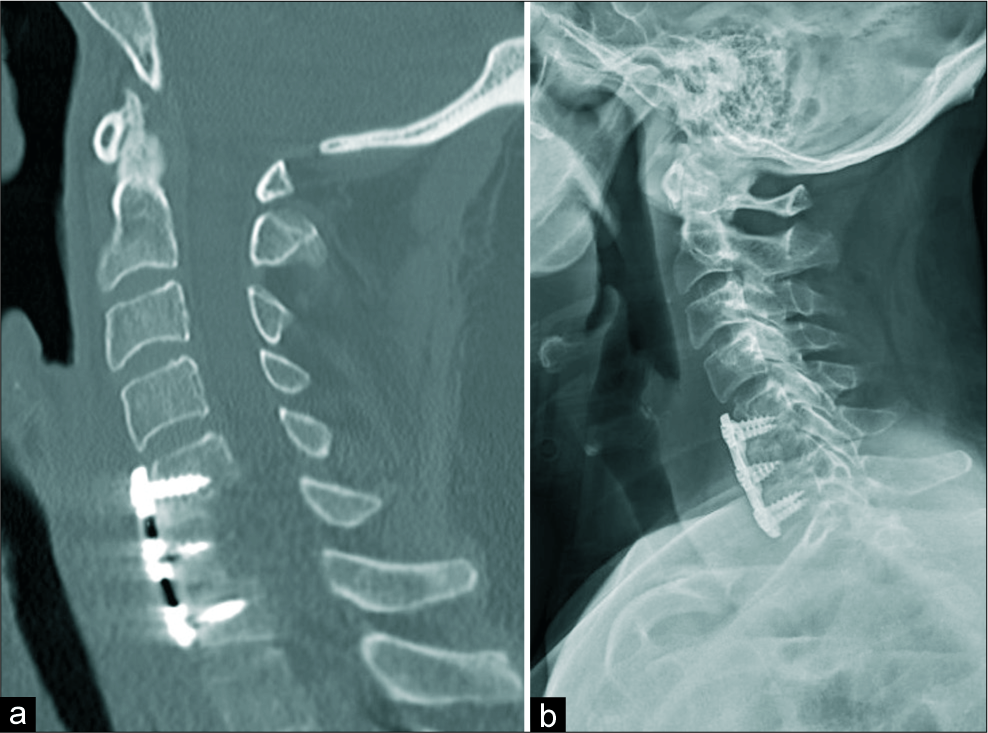
The postoperative computed tomography (CT) demonstrated adequate fixation of the corpectomy graft [

DISCUSSION
Among the several options for reconstructing the anterior cervical spine, autologous iliac crest or fibula graft is still considered the “gold standard.” High rates of autograft donor site complications have been reported (20%–53%), although some of these studies may have been influenced by industry.[
Here, we present a novel technique that uses autogenous cervical corpectomy bone graft for cervical reconstruction, which lacks the morbidity seen with other constructs. Further, removing the vertebral body en bloc preserves a larger quantity of native bone to achieve fusion, and the only instrumentation required is an anterior plate with screws. The latter makes it less expensive than other options for reconstruction, such as the use of a cage.
Technical recommendations for autograft corpectomy/ fusion
A few technical recommendations should be noted when attempting to utilize this technique. First, it is important to expose the vertebral bodies as far lateral as the uncovertebral joints so that troughs can be drilled just medial to this location. Second, when removing the vertebral body en bloc after drilling bilateral troughs, it is critical to avoid placing excess traction on the spinal cord. Third, the structural autograft is relatively shallow, necessitating short screws for affixing the ACDF plate.
Limitations of the technique
Potential limitations of this technique exist: (a) structural autograft may not provide the same degree of rigidity and biomechanical stability as other constructs; (b) in patients with osteoporosis, the autograft may not adequately support axial or rotational forces increasing the risk of collapse, displacement, or segmental kyphosis; (c) expandable cages may provide greater control over restoring the height and lordosis at the surgical level; (d) this technique is not feasible when there is osteomyelitis or tumor infiltration in the vertebral body to be removed; and (e) some patients do not have large enough vertebral bodies to function as structural autografts without sacrificing intervertebral height and lordosis.
A larger series is needed to establish the safety and efficacy of this technique. However, we feel that this novel approach has several beneficial attributes including its use of autologous bone, lack of a donor site and cage with their attendant complications, and relative inexpensiveness.
CONCLUSION
Following an anterior cervical corpectomy, the intervening vertebral body can be carefully removed en bloc and rotated 90 degrees to serve as the corpectomy construct with routine supplementation using a cervical plate. Additional cases are required to determine the technique’s safety and efficacy.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Banwart JC, Asher MA, Hassanein RS. Iliac crest bone graft harvest donor site morbidity. A statistical evaluation. Spine (Phila Pa 1976). 1995. 20: 1055-60
2. Castellvi AE, Castellvi A, Clabeaux DH. Corpectomy with titanium cage reconstruction in the cervical spine. J Clin Neurosci. 2012. 19: 517-21
3. Hartmann S, Kavakebi P, Wipplinger C, Tschugg A, Girod PP, Lener S. Retrospective analysis of cervical corpectomies: Implant-related complications of one and two-level corpectomies in 45 patients. Neurosurg Rev. 2018. 41: 285-90
4. Malloy KM, Hilibrand AS. Autograft versus allograft in degenerative cervical disease. Clin Orthop Relat Res. 2002. 394: 27-38
5. Nassr A, Khan MH, Ali MH, Espiritu MT, Hanks SE, Lee JY. Donor-site complications of autogenous nonvascularized fibula strut graft harvest for anterior cervical corpectomy and fusion surgery: Experience with 163 consecutive cases. Spine J. 2009. 9: 893-8
6. Tuchman A, Brodke DS, Youssef JA, Meisel HJ, Dettori JR, Park JB. Iliac crest bone graft versus local autograft or allograft for lumbar spinal fusion: A systematic review. Global Spine J. 2016. 6: 592-606
7. Weber MH, Fortin M, Shen J, Tay B, Hu SS, Berven S. Graft subsidence and revision rates following anterior cervical corpectomy: A clinical study comparing different interbody cages. Clin Spine Surg. 2017. 30: E1239-45
8. Zeng J, Duan Y, Yang Y, Wang B, Hong Y, Lou J. Anterior corpectomy and reconstruction using dynamic cervical plate and titanium mesh cage for cervical spondylotic myelopathy: A minimum 5-year follow-up study. Medicine (Baltimore). 2018. 97: e9724-

