

- Department of Neurosurgery, Kagawa Rosai Byoin, Marugame, Kagawa, Japan.
Correspondence Address:
Kimihiro Yoshino, Department of Neurosurgery, Kagawa Rosai Byoin, Marugame, Kagawa, Japan.
DOI:10.25259/SNI_503_2020
Copyright: © 2021 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Nobuhiko Kawai, Satoru Yabuno, Koji Hirashita, Kimihiro Yoshino. A case of transpetrosal penetrating head injury near the sigmoid sinus. 20-Sep-2021;12:468
How to cite this URL: Nobuhiko Kawai, Satoru Yabuno, Koji Hirashita, Kimihiro Yoshino. A case of transpetrosal penetrating head injury near the sigmoid sinus. 20-Sep-2021;12:468. Available from: https://surgicalneurologyint.com/surgicalint-articles/11124/
Date of Submission
09-Aug-2020
Date of Acceptance
23-Apr-2021
Date of Web Publication
20-Sep-2021
Abstract
Background: Penetrating brain injury is relatively rare, which occurs in 0.4% of all head trauma. In past reports, the orbit, nasal cavity, and oral cavity are the most common routes of entry of foreign substances into the skull. In this case report, we experienced a rare case of head trauma who injury through the petrosal bone. To the best of our knowledge, there is no similar literature.
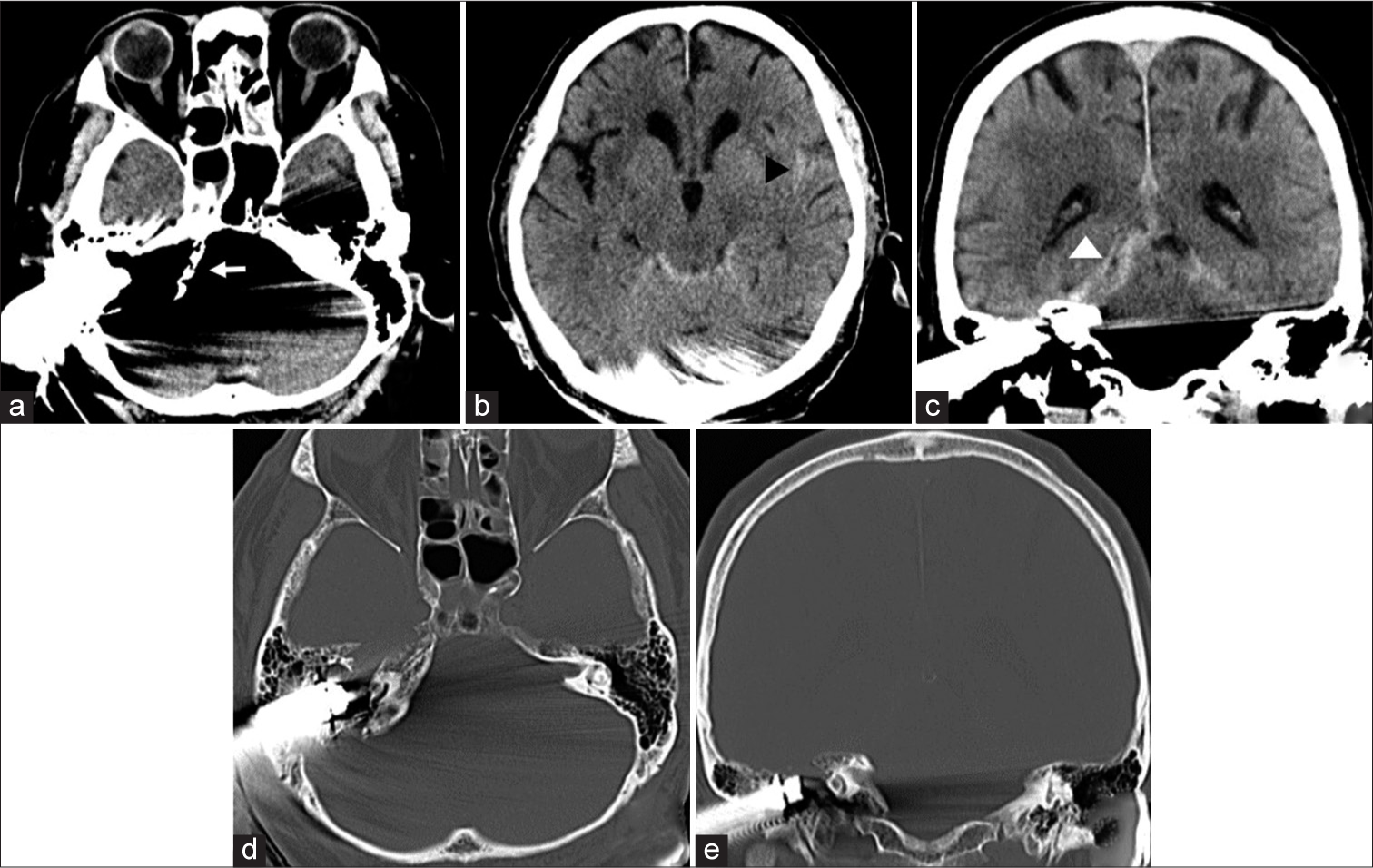
Case Description: A 69-year-old man accidentally fell from a stepladder with a height of 3 m. There was a sprinkler on the ground, and it went through his posterior part of the right auricle at the collision. He was alert on admission. However, neurological examination showed right trigeminal, abducens, and facial nerve palsy. Computed tomography was performed, and it revealed that the objects penetrated the petrosal bone. Furthermore, it caused traumatic subarachnoid hemorrhage and acute subdural hemorrhage. Fortunately, it did not reach any cerebral artery and cerebral parenchyma. Immediately it was surgically removed with a good outcome.
Conclusion: When suspected sigmoid sinus injury in head penetrating injury, craniotomy should be considered with bleeding from the sigmoid sinus during surgery.
Keywords: Penetrating head injury, Petrosal bone fracture, Sigmoid sinus
INTRODUCTION
Head penetrating injuries are relatively rare and reported to be about 0.4% of head trauma.[
We report a case in which a foreign body invaded the sigmoid sinus through the petrosal bone and suspected venous sinus injury was removed by craniotomy.
CASE PRESENTATION
A 69-year-old man fell from a stepladder with a height of about 3 m, and a sprinkler head penetrated the posterior part of the right auricle. His Glasgow Coma Scale was initially 15, and no obvious motor paralysis or sensory impairment was observed. He had abduction disorder of the right eye, paralysis of the right facial muscles, and decreased perception of the right face.
Computed tomography revealed that the body had penetrated the petrosal bone [

Operation
The operation was performed in the lower-left lateral position. The skin incision was designed in 2 pieces because we were able to rotate over a wide area to observe the vicinity of the middle fossa and sigmoid sinus [


Postoperatively, broad-spectrum antibacterial drugs (CTRX and VCM) were administered for 2 weeks to prevent meningitis. He also had continuous lumbar drainage for 1 week to prevent cerebrospinal fluid leakage. There were no apparent symptoms of it.
After surgery, the right hearing was completely lost in the examination. Three weeks after the operation, he was transferred to a rehabilitation hospital.
DISCUSSION
Petrosal bone fractures account for about 20% of all skull fractures and are classified into longitudinal fractures and transverse. It is clinical symptoms include deafness, cerebrospinal fluid effusion, and facial paralysis. About 50% of the cases involved permanent paralysis due to nerve damage.[
For head penetrating injuries, it is recommended to perform surgery within 12 h after the injury to prevent infection.[
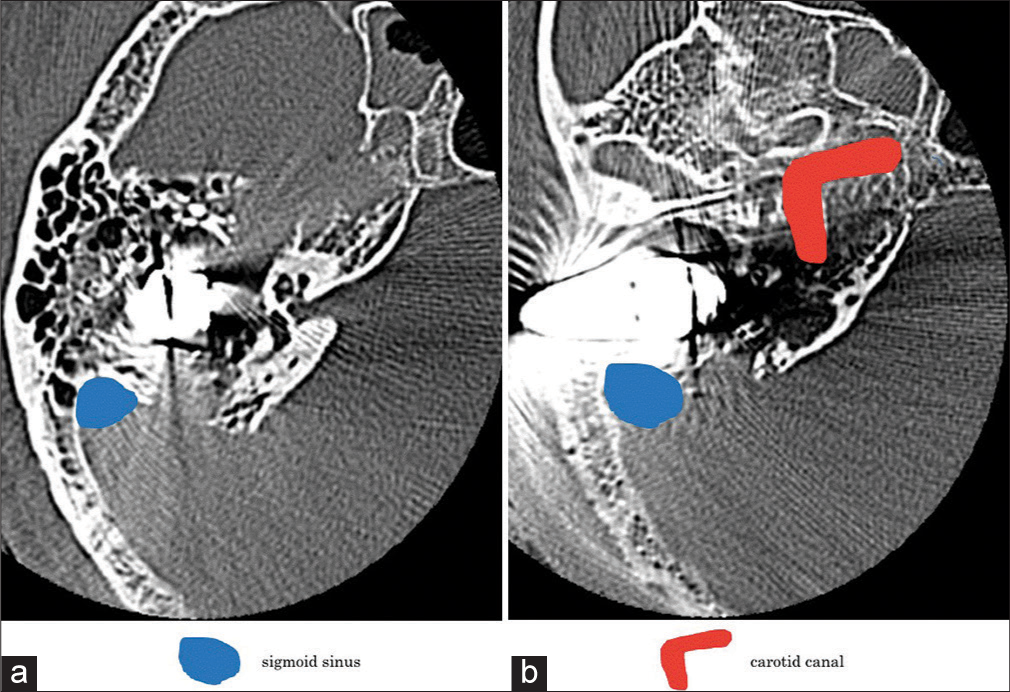
In this case, sigmoid sinus injury was suspected by DSA, so direct surgery was performed. When performing trans-petrosal head penetrating trauma, it is important that treatment is performed in conjunction with careful examinations of the microanatomy inside the petrosal bone and the positional relationships with surrounding arteries and veins.
In this case, it was suspected that a foreign substance stuck in the petrosal bone had damaged the sigmoid sinus, and angiography was performed followed by craniotomy. As already reported in the past, it is said that foreign matter in the skull is removed in the operating room in the case of head penetrating injury. In addition, in preoperative evaluation, it is necessary to evaluate not only contrast-enhanced CT but also angiography to evaluate large blood vessel damage.[
There are no case reports of suspected sigmoid sinus injury due to penetrating trauma, as far as we have searched the literature. As the point of treatment of our case, firstly, we tried to confirm the damaged site visually by excising the bone around the foreign body extensively and securing a wide surgical field, including the puncture site. We must confirm intraoperatively because foreign matter damaged the middle skull base and dural damage on CT. In addition, to secure working space for repairing the damaged part in the case of a dural injury, it was necessary to provide a relatively large craniotomy above the foreign body.
Second, when checking for damage to the sinus, exposing the sigmoid sinus unnecessarily may make it difficult to stop bleeding . For this reason, we avoided exposing the sinus intraoperatively. If the sinus was damaged while the sinus was exposed, or if there was bleeding from a damaged part due to a foreign substance, it may be difficult to stop bleeding in case the sigmoid sinus is partially exposed. Therefore, bone was removed so that only the sigmoid sinus near the foreign body could be exposed.
Third, this time we approached from the parietal side and the sigmoid sinus side of the foreign body. If the sigmoid sinus was approached first, the craniotomy field was narrow, and it was expected that hemostasis would be difficult when bleeding occurred.
CONCLUSION
In the case, if the artery or venous sinus is damaged due to a foreign substance penetrating and branching, we should consider that not only the preoperative evaluation of blood vessel damage but also the procedure to approach assuming the case of bleeding during surgery.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Ghorayab BY, Yeakley JW. Temporal bone fractures: Longitudinal or oblique? The case for oblique temporal bone fractures. Laryngoscope. 1992. 2: 129-34
2. Greenberg MS.editors. Non-missile penetrating trauma. HandBook of Neurosurgery. Greenberg, MS: Greenberg Graphics Inc; 1997. p. 743
3. 4. Huo S, Cui F, Ohno Y. Fatal penetrating head injury by bamboo fragments. Leg Med (Tokyo). 2013. 15: 99-102 5. 6. Shrader EC, Schlezinger NS. Neuro-ophthalmologic evaluation of abducens nerve paralysis. Arch Ophtal. 1960. 63: 84-91

