

- Department of Neurosurgery, Hamad Medical Corporation, Hamad General Hospital, Doha, Qatar.
- Department of Pathology, Hamad Medical Corporation, Hamad General Hospital, Doha, Qatar.
Correspondence Address:
Ahmed Taha Elsayed Shaaban
Department of Neurosurgery, Hamad Medical Corporation, Hamad General Hospital, Doha, Qatar.
DOI:10.25259/SNI_653_2020
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Ahmed Taha Elsayed Shaaban1, Mostafa Ibrahem1, Ahmed Saleh1, Abdulrazzaq Haider2, Abdulnasser Alyafai1. Brown tumor due to primary hyperparathyroidism resulting in acute paraparesis: Case report and literature review. 21-Oct-2020;11:355
How to cite this URL: Ahmed Taha Elsayed Shaaban1, Mostafa Ibrahem1, Ahmed Saleh1, Abdulrazzaq Haider2, Abdulnasser Alyafai1. Brown tumor due to primary hyperparathyroidism resulting in acute paraparesis: Case report and literature review. 21-Oct-2020;11:355. Available from: https://surgicalneurologyint.com/surgicalint-articles/10340/
Date of Submission
17-Sep-2020
Date of Acceptance
03-Oct-2020
Date of Web Publication
21-Oct-2020
Abstract
Background: Brown tumor (Osteoclastoma) is a rare benign, focal, lytic bone lesion most commonly attributed to a parathyroid adenoma; it occurs in approximately 5% of patients with primary hyperparathyroidism, and 13% of patients with secondary hyperparathyroidism. Most tumors are located in the mandible, pelvis, ribs, and large bones; only rarely is it found in the axial spine.
Case Description: A 37-year-old male with primary hyperparathyroidism presented with an MR-documented T4 and T5 brown tumor (Osteitis Fibrosa Cystica) resulting in an acute paraparesis. The patient successfully underwent excisional biopsy of an expansile, enhancing, bony destructive lesion at the T4-5 level. Subsequently, he required subtotal excision of a left upper parathyroid tumor.
Conclusion: Patient with primary hyperparathyroidism may acutely present with paraparesis attributed to brown tumors of the spine warranting emergent operative decompression.
Keywords: Osteitis fibrosa cystica, Primary hyperparathyroidism, Spine brown tumor
INTRODUCTION
Brown tumor (Osteoclastoma) is a rare, benign, and focal lytic bone lesion that is most commonly attributed to a parathyroid adenoma. It occurs in 5% of primary and 13% of secondary cases of hyperparathyroidism.[
CASE PRESENTATION
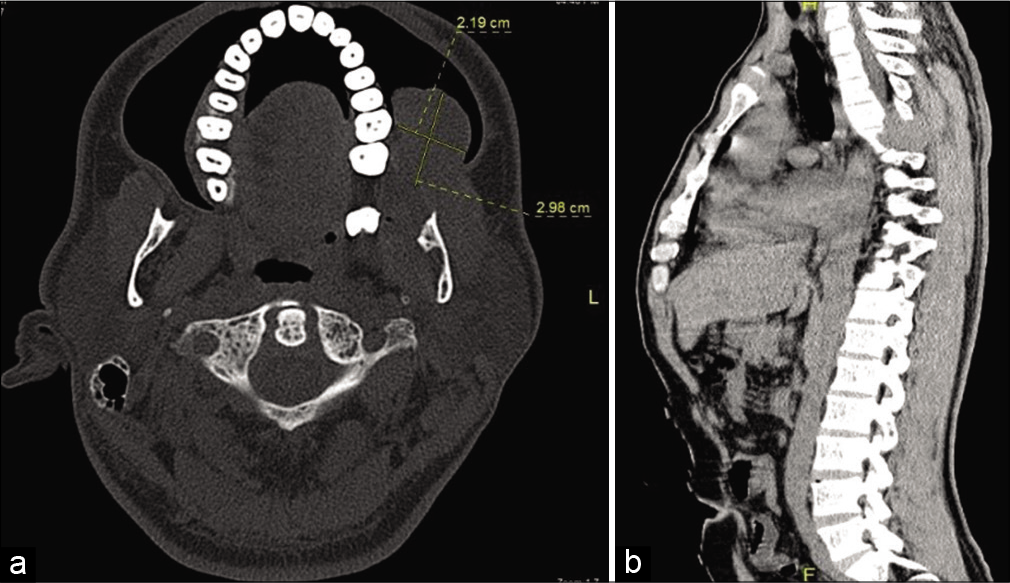
For 2 months, a 37-year-old male demonstrated a slow-growing lesion involving the dendro-alveolar segment of the left upper maxilla (rounded mass of 4 × 4 cm, nonulcerated with normal oral mucosa) [
Holospinal contrast enhanced MR
Multiple, expansile, enhancing, and bony destructive lesions were seen at many thoracic, lumbar, and sacral spinal levels (e.g., involving mainly the neural arches, and adjacent soft tissues). The largest lesions were at the T4/T5 level; the first contributed to marked central cord compression, while an additional very large, expansile, destructive bony lesion involved the left – T4-T5 ribs, and infiltrated into the adjacent paraspinal muscles. Other similar and/or smaller lesions involved multiple spinous processes, lamina, and/or vertebral bodies (e.g., of C5-6, L2-L4, S1-S2, and the left iliac bone). There was also an accompanying dorsal thoracic scoliotic deformity convex to the right side [

Figure 2:
(a) MRI thoracic spine T2 sagittal on the left and T1 sagittal on the right. (b) MRI thoracic spine T2 sagittal on the left and T1 sagittal on the right (view more lateral to the left side). (c) MRI thoracic spine T2 sagittal and axial. (d) MRI thoracic spine T1 sagittal pre and post gadolinium-based contrast. (e) MRI thoracic spine T1 with contrast sagittal and axial. (f) MRI spine with contrast T1 with contrast lumbar spine sagittal on the left side and T1 with contrast sagittal cervical spine on the right side.
Surgery
Due to significant cord compression, a T4/T5 coronal hemilaminectomy was performed with medial facetectomy/ foraminotomy; care was taken to preserve the lateral two-third of the facet joints, and thus maintain stability. The soft and highly vascular T4-T5 tumor clearly compressed the thoracic cord, and infiltrated the para spinal ribs/muscle; tumor was readily debulked. The histopathology confirmed a brown tumor attributed to primary hyperparathyroidism [
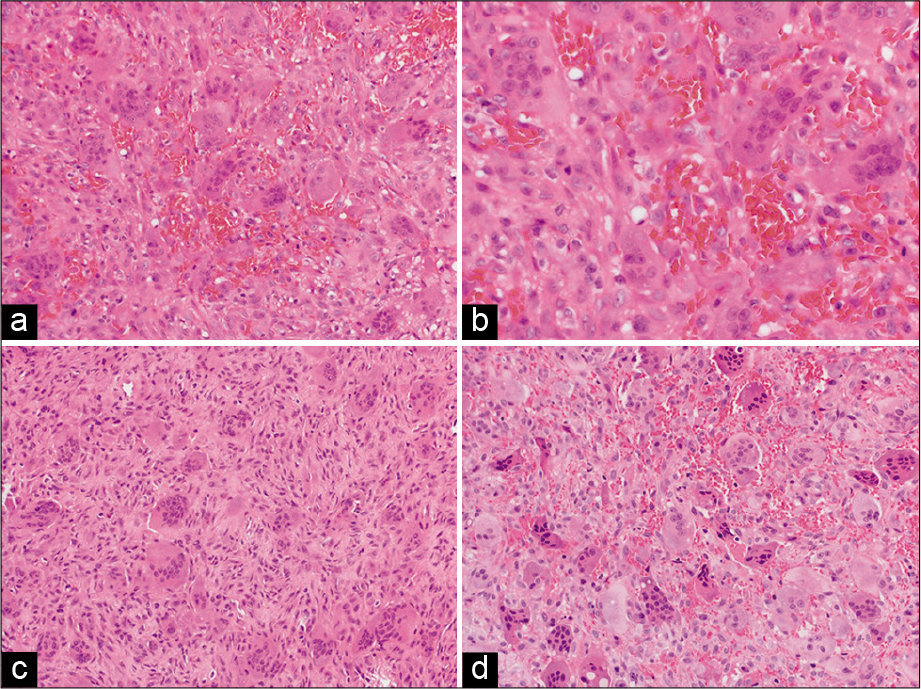
Figure 3:
(a-d) Excisional biopsy shows cellular lesion composed of plump and spindle-shaped cells admixed with numerous multinucleated osteoclast-like giant cells with areas of hemorrhage and hemosiderin-laden macrophages. It was highly suggestive of brown tumor taking in consideration multiple bone involvement.
Diagnosis of primary hyperparathyroidism
Primary hyperparathyroidism attributed to a parathyroid adenoma caused this patient’s elevated parathyroid hormone (PTH) level (e.g., 1900 phml). The patient subsequently required excision of the left upper parathyroid gland, following which calcium levels normalized [
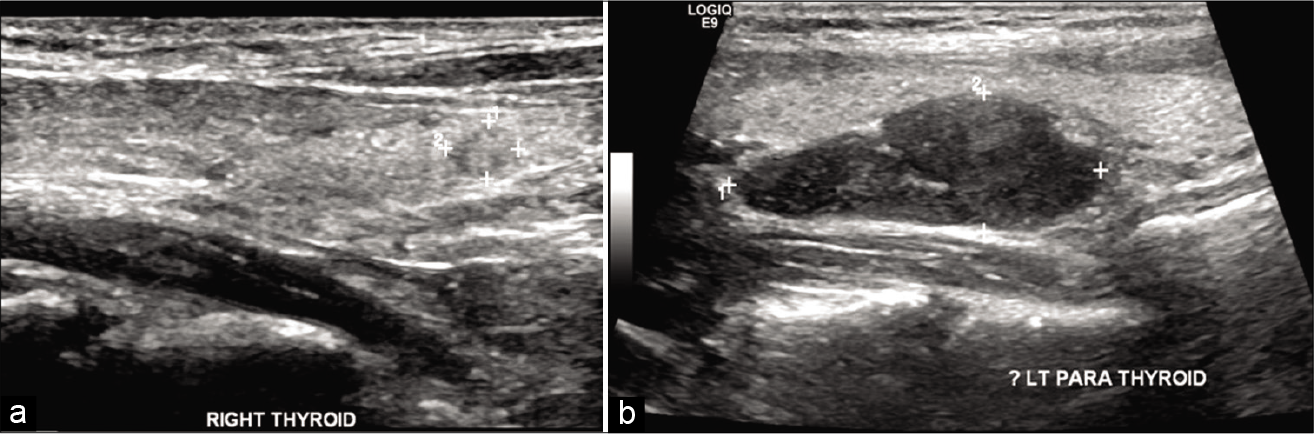
Figure 4:
(a) Thyroid ultrasound, right lobe of thyroid shows a small solid nodule measuring 4 × 5 mm noted at the lower aspect of the right lobe. Isthmus measures 2.5 mm. (b) Thyroid ultrasound, left lobe of thyroid at the region of the left parathyroid enlarged lobulated hypoechoic area noted measuring 34 × 13 mm with extremely increased vascularity, most likely representing a parathyroid adenoma.


DISCUSSION
Brown tumors are rare benign, lytic bone lesions that appear grossly as soft, red brown expansile masses within the bone. They occur due to primary, secondary, or tertiary hyperparathyroidism.[

Pathogenesis of brown tumors
Primary hyperparathyroidism and resultant spinal brown tumors are attributed to adenomas, resulting in elevated PTH, and heightened calcium levels; both contribute to abnormal bone mineralization. They also result in decreased bone density, and increased bone resorption (e.g., due to heightened osteoclastic activity that progressively thins the bony cortex, and trabeculae). Resultant microfractures/microhemorrhages increase the activity of multinucleated macrophages, contributing to the formation of fibrous tissue resulting in osteitis fibrosa cystica. Notably, the typical brown tumors reflect the accumulation of hemosiderin.[
Differential diagnosis of brown tumors
The differential diagnoses for brown tumors include: metastases, multiple myeloma, sarcomas, giant cell reparative granulomas, lymphangiomatosis, leukemia, Langerhans cell histiocytosis, multiple bone cysts, aneurysmal bone cysts, and nonossifying fibromas.[
Treatment of brown tumors: medical versus surgical management
There is an ongoing controversy regarding the comparative efficacy of parathyroidectomy with/without the need for attendant spine surgery.[
CONCLUSION
Patients with primary hyperparathyroidism may acutely present with paraparesis attributed to thoracic brown tumors warranting emergent operative decompression, followed by resection of parathyroid adenomas.
Declaration of patient consent
Institutional Review Board (IRB) permission obtained for the study.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Fargen KM, Lin CS, Jeung JA, Yachnis AT, Jacob RP, Velat GJ. Vertebral brown tumors causing neurologic compromise. World Neurosurg. 2013. 79: 208.e1-6
2. Gregoire C, Soussan M, Dumuis ML, Naggara N, Martin A, Dhote R. Contribution of multimodality imaging for positive and aetiological diagnosis of multiple brown tumours. Ann Endocrinol (Paris). 2012. 73: 43-50
3. Hammou O, Azzouzi H, Ichchou L. Spinal cord compression secondary to brown tumor as first manifestation of primary hyperparathyroidism. World Neurosurg. 2020. 137: 384-8
4. Hu J, He S, Yang J, Ye C, Yang X, Xiao J. Management of brown tumor of spine with primary hyperparathyroidism: A case report and literature review. Medicine (Baltimore). 2019. 98: e15007
5. Khalil PN, Heining SM, Huss R, Ihrler S, Siebeck M, Hallfeldt K. Natural history and surgical treatment of brown tumor lesions at various sites in refractory primary hyperparathyroidism. Eur J Med Res. 2007. 12: 222-30
6. Pavlovic S, Valyi-Nagy T, Profirovic J, David O. Fine-needle aspiration of brown tumor of bone: Cytologic features with radiologic and histologic correlation. Diagn Cytopathol. 2009. 37: 136-9
7. Sonmez E, Tezcaner T, Coven I, Terzi A. Brown tumor of the thoracic spine: First manifestation of primary hyperparathyroidism. J Korean Neurosurg Soc. 2015. 58: 389-92
8. Tayfun H, Metin O, Hakan S, Zafer B, Vardar AF. Brown tumor as an unusual but preventable cause of spinal cord compression: Case report and review of the literature. Asian J Neurosurg. 2014. 9: 40-4
9. Ullah E, Ahmad M, Ali SA, Redhu N. Primary hyperparathyroidism having multiple brown tumors mimicking malignancy. Indian J Endocrinol Metab. 2012. 16: 1040-2
10. Zaheer SN, Byrne ST, Poonnoose SI, Vrodos NJ. Brown tumour of the spine in a renal transplant patient. J Clin Neurosci. 2009. 16: 1230-2

