

- Department of Neurosurgery, All India Institute of Medical Sciences, Raipur, Chhattisgarh,
- Department of Laboratory Medicine, Sahara Hospital, Lucknow, Uttar Pradesh, India.
Correspondence Address:
Lokesh Suresh Nehete
Department of Neurosurgery, All India Institute of Medical Sciences, Raipur, Chhattisgarh,
DOI:10.25259/SNI_833_2020
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Prashant Raj Singh1, Nitish Nayak1, Surendra Kumar Gupta1, Raghavendra Kumar Sharma1, Anju Shukla2, Lokesh Suresh Nehete1. Hemorrhage in long segment cervical schwannoma; case report and literature review. 29-Dec-2020;11:476
How to cite this URL: Prashant Raj Singh1, Nitish Nayak1, Surendra Kumar Gupta1, Raghavendra Kumar Sharma1, Anju Shukla2, Lokesh Suresh Nehete1. Hemorrhage in long segment cervical schwannoma; case report and literature review. 29-Dec-2020;11:476. Available from: https://surgicalneurologyint.com/surgicalint-articles/10492/
Date of Submission
19-Nov-2020
Date of Acceptance
09-Dec-2020
Date of Web Publication
29-Dec-2020
Abstract
Background: Although hemorrhages associated with cervical and thoracic intraspinal schwannomas are typically localized to the subarachnoid hemorrhages (SAH) or subdural hemorrhages (SDH) compartments, rare intratumoral bleeds may also occur.
Methods: In the literature, we found and analyzed multiple factors for 13 cases (e.g., epidemiological, clinical, and pathological) of cervical schwannomas with intratumoral hemorrhages (ITH). We added the 14th case of a 35-year-old female with along segment cervical schwannoma with ITH who presented with acute quadriplegia and respiratory decompensation.
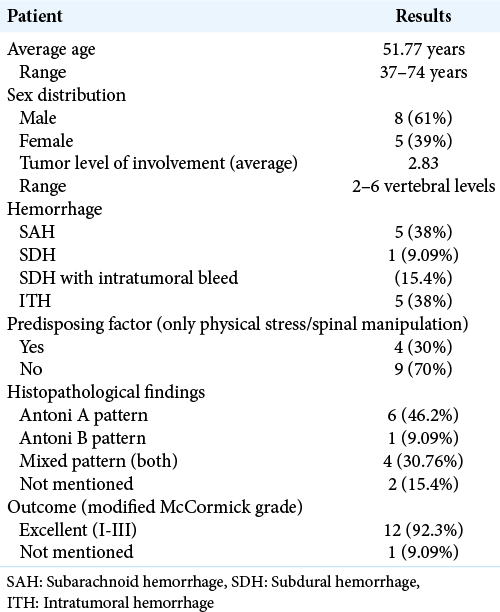
Results: These 14 patients averaged 51.77 years of age, 60% were male, and the tumor involved 2.83 segments. The incidence of SAH and ITH was noted in five cases each, while SDH’s were very rare. The pathological characteristics were consistent with the diagnosis of cellular schwannomas with S-100 positivity. The clinical outcomes were good (100%) in all the cases, including the one presented (modified McCormick score III).
Conclusion: Cervical schwannomas with ITH are rare, and the surgical outcomes in such patients are good-excellent (>90%). The histopathology is always of prime importance and decisive in establishing and confirming the etiology of such ITH.
Keywords: Cellular schwannoma, Intratumoral bleed, Schwannoma with bleed
INTRODUCTION
Schwannomas are some of the most common peripheral nerve sheath tumors.[
MATERIALS AND METHODS
We utilized (2020) two electronic databases (e.g., U.S. National Library of Medicine, National Institutes of Health [PubMed], and EMBASE) to identify studies of cervical schwannoma with ITH [

Literature review
We reviewed 13 cases from 13 articles regarding cervical ITHs attributed to spinal schwannomas, exclusive of our case. The following variables were studied: age, gender, predisposing factor, clinical presentation, size of the tumor, level of the tumor, hemorrhages, pathological tumor features, and outcomes (e.g., using the modified McCormick score).
Of the 13 previously reported cases of cervical schwannomas hemorrhages, spontaneous ITH were noted in five cases (38%), SAH in five cases (38%), and SDH with intratumoral bleed in two cases (15%), with one isolated case of SDH alone [
Case report
Case illustration
A 35-year-old female were presented with the sudden onset of quadriparesis over 1 week duration and 2 days of increased respiratory distress. On examination, she had a flaccid quadriparesis (motor 1/5 both upper extremities and 0/5 in both lower extremities) with a C7 sensory level and acute urinary retention. A contrast holo-neuraxis MRI showed a T1 hypointense, T2 heterogeneously hyperintense (e.g., with peripheral irregularity), and a non-enhancing central-large intradural extramedullary lesion from C2-T2 [
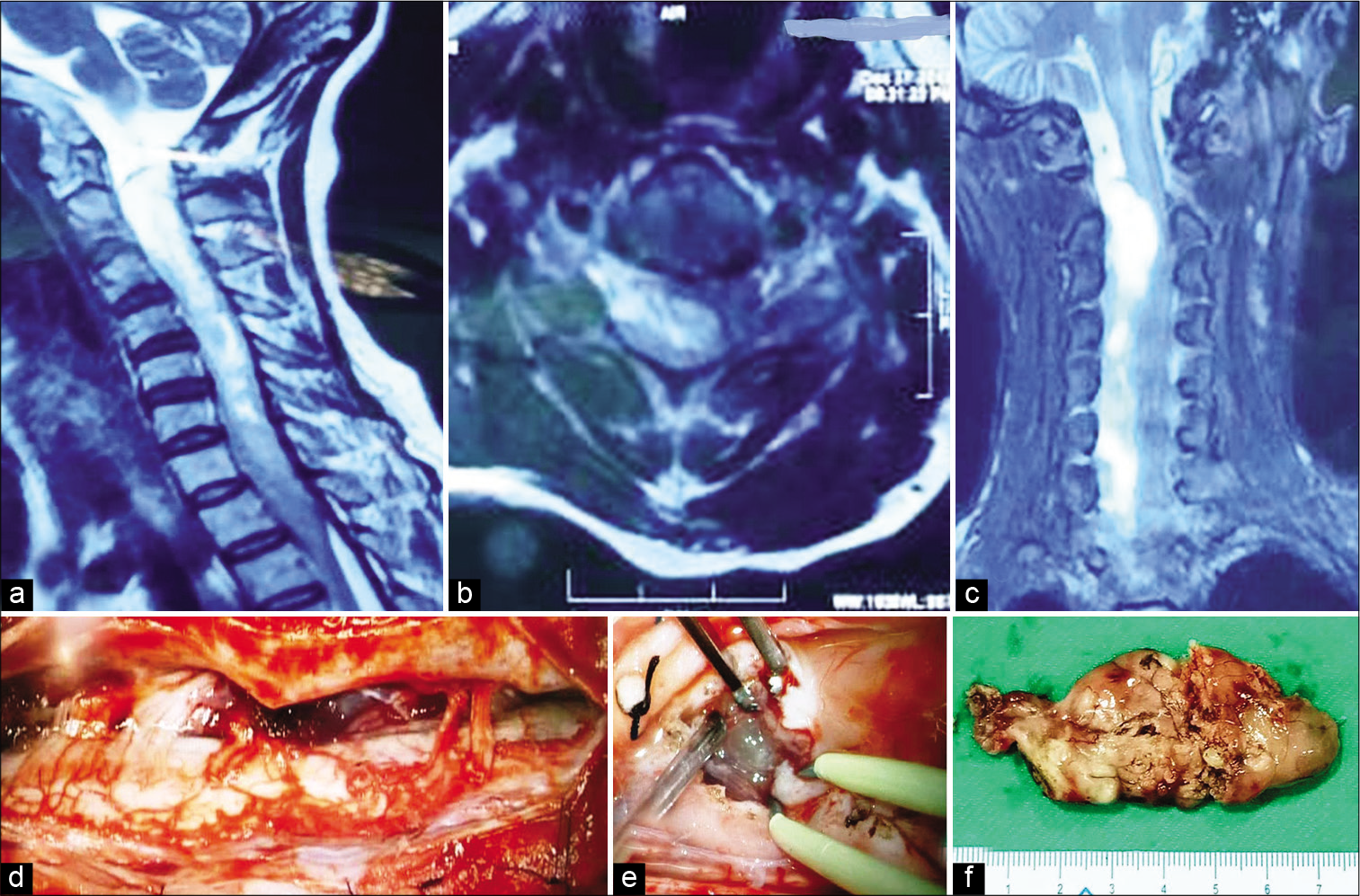
Figure 1:
T2-weighted images of magnetic resonance imaging in sagittal (a), axial (b), and coronal (c) sections – a large mixed intensity intradural extramedullary spinal cord tumor from C2-D2 location and with significant compression of the spinal cord. A large brownish tumor anterolateral to the cord and pushing it to the left side (d), with intratumoral blood clots (e), and completely excised tumor (f).
Surgery
The patient underwent a C3-T3 Laminoplasty. After opening the dura, a giant dark brown subarachnoid mass was found attached to the right C2 nerve root and the spinal cord was displaced toward the left. The tumor was soft in consistency and accompanied by a lobulated dark-brown hemorrhage (e.g., with the altered thickness of blood clots of different ages). The tumor was easily suckable, and a good cleavage plane could develop circumferentially around the tumor, which was approximately 7.5 cm in size [
Histology
The histological examination revealed a cellular schwannoma with mixed Antoni A and Antoni B cells and degenerative atypia; however, mitotic activity was not discernible [
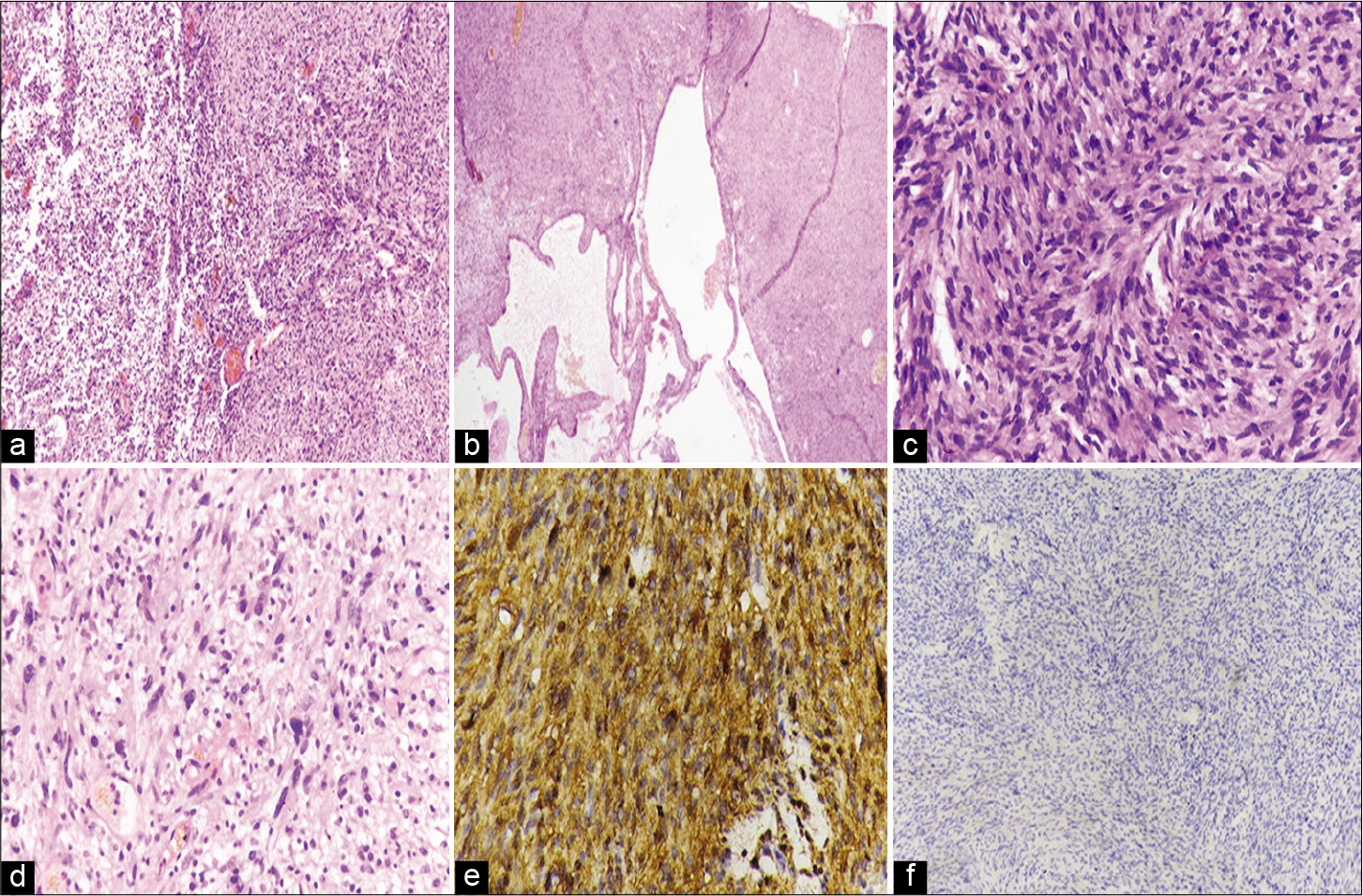
Figure 2:
Illustrated as – (a) Sections showing hypercellular Antoni Type A and hypocellular Antoni Type B areas (H and E, ×10), (b) with interspersed dilated, irregular shaped blood vessels (H and E, ×4), (c) cells are having oval to spindle shape nuclei, fibrillary cytoplasm with minimal atypia (H and E, ×40), (d) degenerative changes with smudgy chromatin, however, mitotic activity is not seen (H and E, ×40), (e) immunohistochemistry showing diffuse and strong S100 positivity and (f) While EMA is negative.
Postoperative course
The postoperative course was uneventful as the patient’s status improved; motor power became 3/5 in both upper and lower extremities, and her respiratory distress regressed. By the time of discharge, she could walk with one person’s support (e.g., motor power still 3–4/5). Her neurological status remained mostly unchanged at the 3 months follow-up (modified McCormick score III).
DISCUSSION
ITH occurring within the cervical spinal are very rare. We reviewed 13 prior cervical schwannomas, five of which were ITH. Of interest, cervical schwannomas equally present with ITH and SAH, while SDHs are rare. Outcomes of ITH within cervical schwannomas appear independent of size, age, or type of bleed, and preoperative neurological status.
The mechanism of hemorrhage in such tumors is variously reported as attributed to; ectatic hyalinized vessels undergoing spontaneous thrombosis[
CONCLUSION
The suspicion of an ITH within a cervical schwannoma must be considered when patients develop the acute onset of quadriparesis/plegia without an attendant history of coagulopathy, hypertension, or spinal manipulation/trauma. The histopathology is the final determinant of the lesion.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Hilton DA, Hanemann CO. Schwannomas and their pathogenesis. Brain Pathol. 2014. 24: 205-20
2. Jenkins AL, Ahuja A, Oliff AH, Sobotka S. Spinal schwannoma presenting due to torsion and hemorrhage: Case report and review of literature. Spine J. 2015. 15: e1-4
3. Jinnai T, Hoshimaru M, Koyama T. Clinical characteristics of spinal nerve sheath tumors: Analysis of 149 cases. Neurosurgery. 2005. 56: 510-5
4. Mills B, Marks PV, Nixon JM. Spinal subarachnoid hemorrhage from an ancient schwannoma of the cervical spine. Br J Neurosurg. 1993. 7: 557-9
5. Ng PY. Schwannoma of the cervical spine presenting with acute haemorrhage. J Clin Neurosci. 2001. 8: 277-8
6. Parmar H, Pang BC, Lim CC, Chng SM, Tan KK. Spinal schwannoma with acute subarachnoid hemorrhage: A diagnostic challenge. AJNR Am J Neuroradiol. 2004. 25: 846-50
7. Sridhar K, Ramamurthi R, Vasudevan MC, Ramamurthi B. Giant invasive spinal schwannomas: Definition and surgical management. J Neurosur. 2001. 94: 210-5

