

- Department of Neurosurgery, University of Wisconsin Hospitals and Clinics, Madison, Wisconsin, United States.
Correspondence Address:
Paul Samuel Page
Department of Neurosurgery, University of Wisconsin Hospitals and Clinics, Madison, Wisconsin, United States.
DOI:10.25259/SNI_936_2020
Copyright: © 2021 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Paul Samuel Page1, Matthew Collins1, James Andrew Stadler1. Minimally invasive resection of pediatric osteoid osteomas: A report of two cases. 08-Apr-2021;12:140
How to cite this URL: Paul Samuel Page1, Matthew Collins1, James Andrew Stadler1. Minimally invasive resection of pediatric osteoid osteomas: A report of two cases. 08-Apr-2021;12:140. Available from: https://surgicalneurologyint.com/surgicalint-articles/10703/
Date of Submission
22-Dec-2020
Date of Acceptance
28-Jan-2021
Date of Web Publication
08-Apr-2021
Abstract
Background: Spinal osteoid osteomas (OOs) are common benign bone tumors that most frequently affect the posterior elements. They occasionally (e.g., 10% of the time) necessitate surgical resection for intractable pain. Given their small size and posterior positions, many may be amenable to minimally invasive surgical approaches.
Case Description: We describe two cases of spinal OOs involving patients 11 and 17 years of age with lesions, respectively, at T7 and C4.
Conclusion: Minimally invasive approaches for resection of small bony spinal OOs are safe and technically achievable approaches.
Keywords: Minimally invasive spine, Pediatric spine, Spine tumor
INTRODUCTION
Spinal osteoid osteomas (OOs), representing 12% of all skeletal neoplasms, are benign bone tumors that most frequently involve the posterior elements (68.4–100%) of the subaxial spine. They usually appear in the second decade of life and occur 2–3-fold more frequently in males. Although other studies have demonstrated that pain attributed to these lesions may be controlled in up to 90% of patients with nonsteroidal anti-inflammatories (NSAIDs), others (10%) may warrant surgical intervention.[
CASE DESCRIPTION
Case 1
An 11-year-old male presented with thoracic back pain of 8 months duration. The MRI showed a left posterior 8 mm, round enhancing lesion involving the base of the left T7 pedicle, consistent with an OO. As his symptoms were not controlled with NSAIDs, the patient underwent a left-sided minimally invasive tubular partial resection of the T7 pedicle [
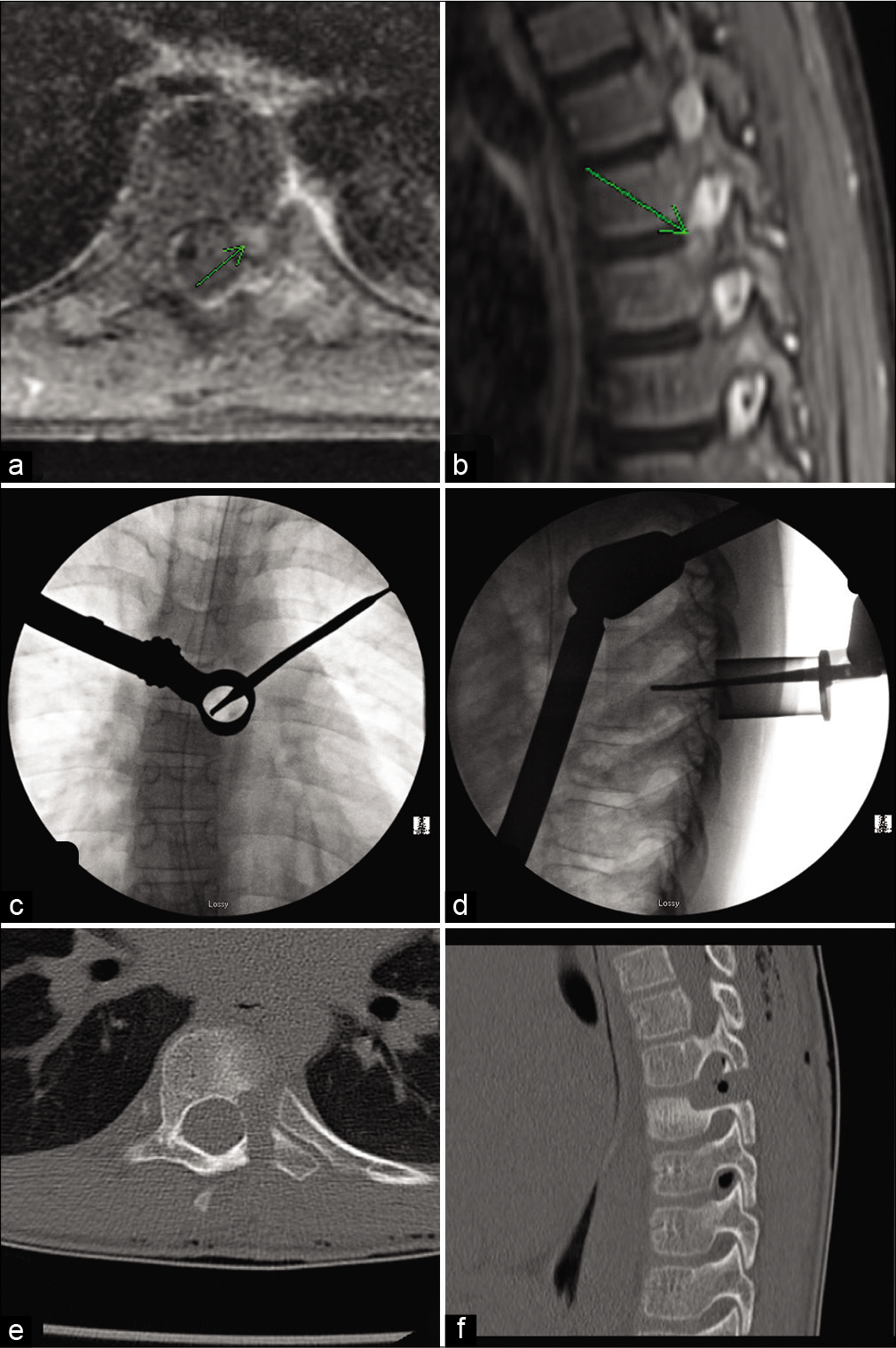
Figure 1:
MRI imaging of a T9 lesion with mild contrast enhancement on T1 (a) and hyperintensity on T2 (b) located in the left T9 pedicle (green arrow). Intraoperative fluoroscopy demonstrating tubular retractor location centered overlying the left T9 pedicle (c and d). Postoperative CT demonstrating resection of the left T9 pedicle and 54 partial T8/9 facetectomy (e and f).
Case 2
A 16-year-old female presented with 1.5 years left paracervical pain that was worse at night and frequently awakened her from sleep. A CT of the cervical spine showed an irregularity of the left C4 superior articular process and a 6 mm expansile mass consistent with an OO. Here, surgery utilized a left-sided MIS tubular retractor remove the C4 lateral mass with fluoroscopic guidance [
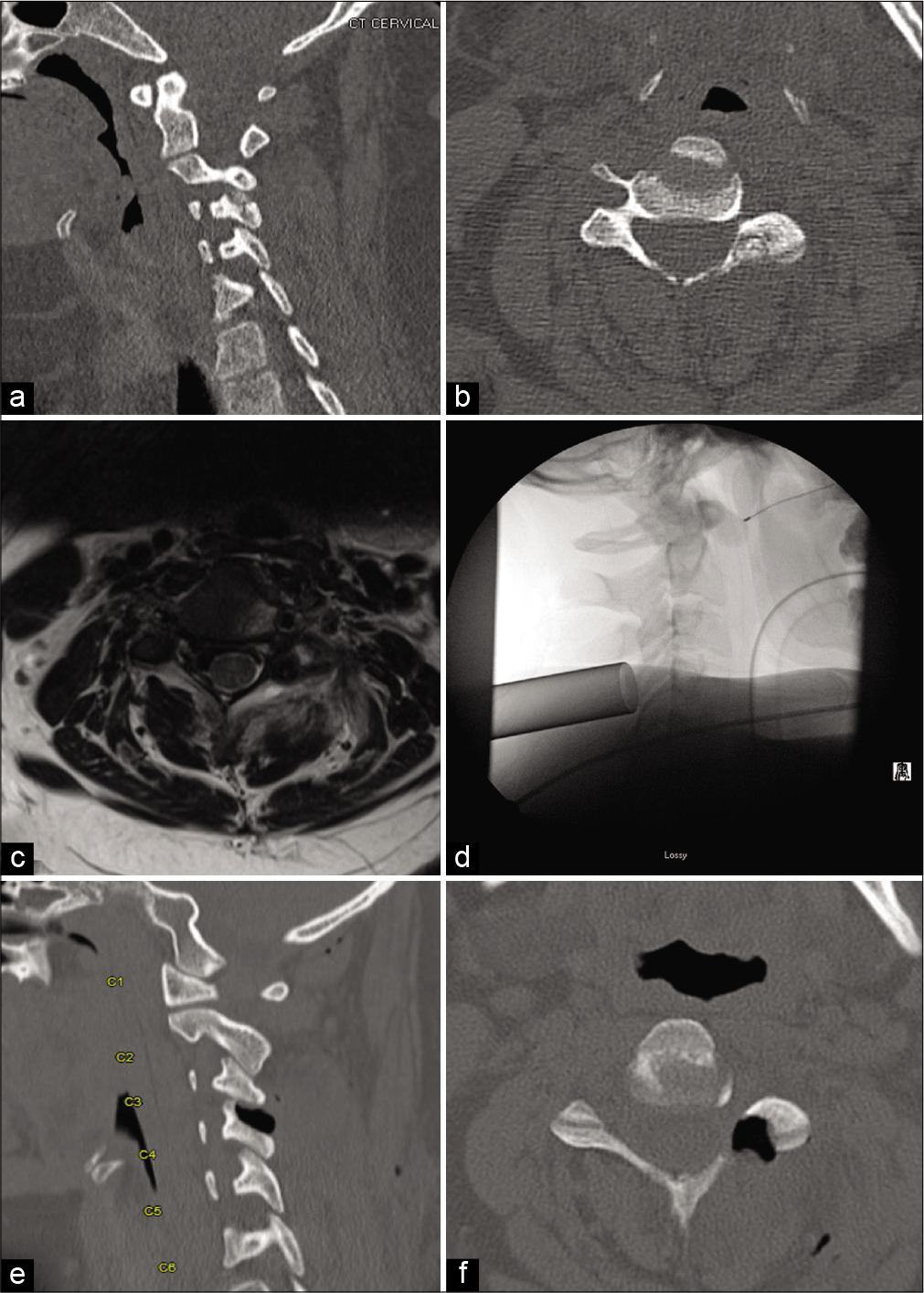
Figure 2:
AP and lateral CT images of a subcentimeter mass located in the lateral mass of the left C4 (a and b). Axial T2 MRI imaging demonstrated a T2 hyperintense lesion in the left lateral mass at C4 (c). Lateral fluoroscopy showing the tubular retractor centered on the C3/4 facet joint (d). Lateral and axial CT images demonstrated a gross total resection of the C4 mass with minimal bony resection (e and f).
DISCUSSION
There is increasing evidence that minimally invasive techniques may be utilized for many routine spinal operations.[
CONCLUSION
Minimally invasive approaches for resection of small bony spinal OOs are safe and technically achievable approaches. These approaches should be considered when considering surgical resection of osteoid osteomas in the pediatric population.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Azouz EM, Kozlowski K, Marton D, Sprague P, Zerhouni A, Asselah F. Osteoid osteoma and osteoblastoma of the spine in children. Report of 22 cases with brief literature review. Pediatr Radiol. 1986. 16: 25-31
2. Foley KT, Smith MM, Rampersaud YR. Microendoscopic approach to far-lateral lumbar disc herniation. Neurosurg Focus. 1999. 7: e5
3. McGirt MJ, Parker SL, Lerner J, Engelhart L, Knight T, Wang MY. Comparative analysis of perioperative surgical site infection after minimally invasive versus open posterior/ transforaminal lumbar interbody fusion: Analysis of hospital billing and discharge data from 5170 patients. J Neurosurg Spine. 2011. 14: 771-8
4. Menger R, Hefner MI, Savardekar AR, Nanda A, Sin A. Minimally invasive spine surgery in the pediatric and adolescent population: A case series. Surg Neurol Int. 2018. 9: 116
5. Minamide A, Yoshida M, Yamada H, Nakagawa Y, Kawai M, Maio K. Endoscope-assisted spinal decompression surgery for lumbar spinal stenosis. J Neurosurg Spine. 2013. 19: 664-71
6. Smith ZA, Fessler RG. Paradigm changes in spine surgery: Evolution of minimally invasive techniques. Nat Rev Neurol. 2012. 8: 443-50
7. Yasuoka S, Peterson HA, Laws ER, MacCarty CS. Pathogenesis and prophylaxis of postlaminectomy deformity of the spine after multiple level laminectomy: Difference between children and adults. Neurosurgery. 1981. 9: 145-52

