

- Department of Neurosurgery, Henry Ford Hospital, Detroit, MI, USA
- Department of Neurosurgery, Hartford Hospital, Hartford, CT, USA
Correspondence Address:
Aqueel Hussain Pabaney
Department of Neurosurgery, Henry Ford Hospital, Detroit, MI, USA
DOI:10.4103/2152-7806.161239
Copyright: © 2015 Pabaney AH. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.How to cite this article: Pabaney AH, Mazaris PA, Kole MK, Reinard KA. Endovascular management of fusiform aneurysm of anterior temporal artery: Technical report. Surg Neurol Int 20-Jul-2015;6:119
How to cite this URL: Pabaney AH, Mazaris PA, Kole MK, Reinard KA. Endovascular management of fusiform aneurysm of anterior temporal artery: Technical report. Surg Neurol Int 20-Jul-2015;6:119. Available from: http://surgicalneurologyint.com/surgicalint_articles/endovascular-management-of-fusiform-aneurysm-of-anterior-temporal-artery-technical-report/
Abstract
Background:The treatment of a rare, nontraumatic, fusiform aneurysm of the anterior temporal artery (ATA) via endovascular techniques is presented, and procedural nuances are highlighted.
Methods:We performed a retrospective chart review and collected demographic and clinical data on the patient presented here; procedural details were extracted from operative notes.
Results:Following successful balloon test occlusion (BTO) of the ATA, complete coil embolization of the ATA, and its associated fusiform aneurysm was performed. Postprocedurally, the patient did not suffer any adverse neurological sequelae.
Conclusion:Selective BTO of intracranial branch vessels is safe, technically feasible, and could serve as a useful technical tool in the treatment of complex, fusiform intracranial aneurysms.
Keywords: Anterior temporal artery, balloon test occlusion, coil occlusion, fusiform aneurysm
INTRODUCTION
Approximately 20% of all clinically significant intracranial aneurysms involve the middle cerebral artery (MCA).[
CASE PRESENTATION
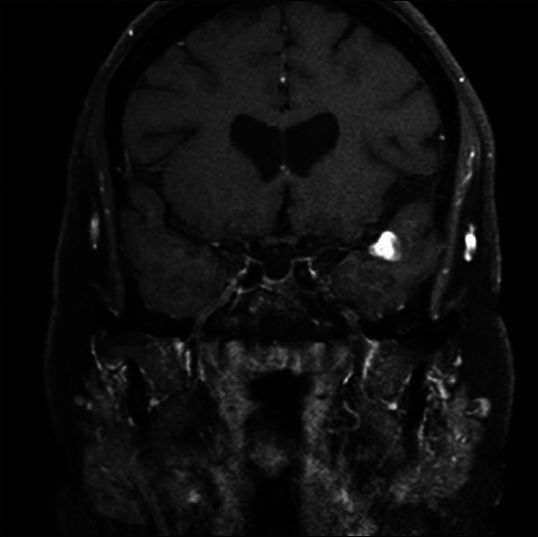
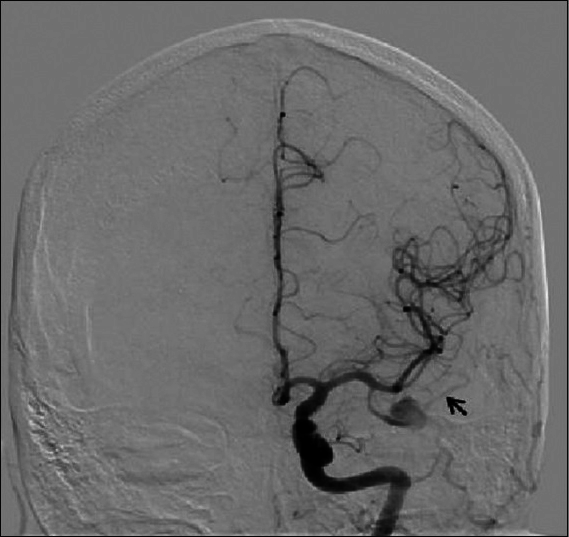
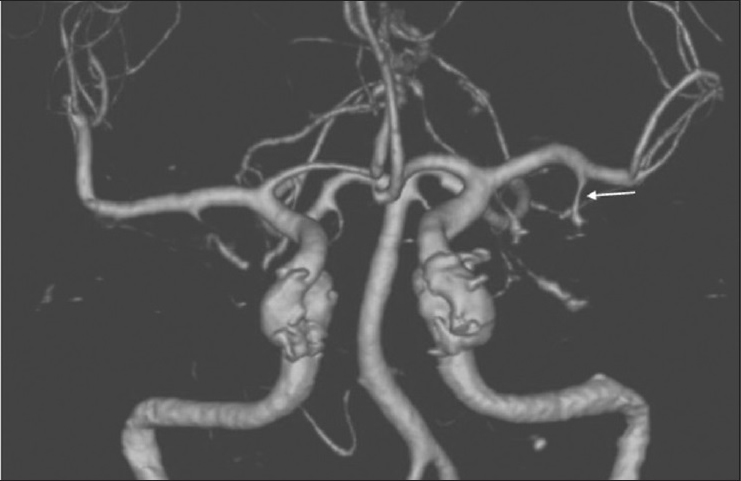
A 37-year-old, right-handed female with no significant past medical history presented to our Emergency Department with several days of holocranial headaches. Her neurological examination was benign with no evidence of meningismus. Computed tomography (CT) of the head revealed a hyperdense mass in the left temporal lobe immediately inferior to the Sylvian fissure. Magnetic resonance imaging/arteriography demonstrated a partially thrombosed aneurysm in an atypical location [

DISCUSSION
The MCA is the largest and most complex of the three major cerebral arteries.[
With the advent of sophisticated neuroimaging modalities, intracranial fusiform aneurysms are reported with increasing frequency. To date, most studies have focused on fusiform aneurysms of the vertebrobasilar system. As such, the pathogenesis, clinical features, radiographic features, and treatment options available for fusiform aneurysms of the posterior circulation are well documented.[
It has been hypothesized that spontaneous fusiform MCA aneurysms may develop as a result of arterial dissection with intramural hemorrhage between the layers of the intima and the media.[
Advancements in endovascular neurosurgery and the development of modern stents and coil material have provided clinicians with innovative and minimally invasive treatment modalities for the management of disparate and complex intracranial vascular pathologies. Given the small caliber and fragile nature of the dissected vessel involved, endovascular reconstruction techniques using flow-diverting stents were deemed not feasible. In this case, the senior author (M.K.K.) performed a BTO of the ATA prior to aneurysm occlusion and parent vessel sacrifice. BTO of the ICA has a reported positive predictive value that approaches 90%[
CONCLUSION
We present a rare case of an incidental, fusiform aneurysm of ATA that was treated by endovascular coil occlusion and resulted in no neurological sequelae after patient displayed tolerance for balloon occlusion. Superselective BTO could serve as a powerful assessment tool prior to parent vessel sacrifice. Large-scale studies are required to determine the long-term safety and applicability of superselective, intracranial BTO to diverse vascular pathologies.
References
1. Asakura K, Tasaki T, Okada K. A case of unruptured anterior temporal artery aneurysm showing pupil-sparing oculomotor palsy. No Shinkei Geka. 1986. 14: 777-82
2. Bederson JB, Spetzler RF. Anastomosis of the anterior temporal artery to a secondary trunk of the middle cerebral artery for treatment of a giant M1 segment aneurysm. Case report. J Neurosurg. 1992. 76: 863-6
3. Chuang MJ, Lu CH, Cheng MH. Management of middle cerebral artery dissecting aneurysm. Asian J Surg. 2012. 35: 42-8
4. Day AL, Gaposchkin CG, Yu CJ, Rivet DJ, Dacey RG. Spontaneous fusiform middle cerebral artery aneurysms: Characteristics and a proposed mechanism of formation. J Neurosurg. 2003. 99: 228-40
5. Eckard DA, O’Boynick PL, McPherson CM, Eckard VR, Han P, Arnold P. Coil occlusion of the parent artery for treatment of symptomatic peripheral intracranial aneurysms. AJNR Am J Neuroradiol. 2000. 21: 137-42
6. Hosoya T, Adachi M, Yamaguchi K, Haku T, Kayama T, Kato T. Clinical and neuroradiological features of intracranial vertebrobasilar artery dissection. Stroke. 1999. 30: 1083-90
7. Locksley HB, Sahs AL, Knowler L. Report on the cooperative study of intracranial aneurysms and subarachnoid hemorrhage. Section II. General survey of cases in the central registry and characteristics of the sample population. J Neurosurg. 1966. 24: 922-32
8. Narayanan S, Singer R, Abruzzo TA, Hussain MS, Powers CJ, Prestigiacomo CJ. Reporting standards for balloon test occlusion. J Neurointerv Surg. 2013. 5: 503-5
9. Qureshi AI, Suri MF, Khan J, Kim SH, Fessler RD, Ringer AJ. Endovascular treatment of intracranial aneurysms by using Guglielmi detachable coils in awake patients: Safety and feasibility. J Neurosurg. 2001. 94: 880-5
10. Rhoton AL. The supratentorial arteries. Neurosurgery. 2002. 51: 53-120
11. Senbokuya N, Kanemaru K, Kinouchi H, Horikoshi T. Giant serpentine aneurysm of the distal anterior cerebral artery. J Stroke Cerebrovasc Dis. 2012. 21: e7-11
12. Tanriover N, Kawashima M, Rhoton AL Jr, Ulm AJ, Mericle RA. Microsurgical anatomy of the early branches of the middle cerebral artery: Morphometric analysis and classification with angiographic correlation. J Neurosurg. 2003. 98: 1277-90
13. Tsapkini K, Frangakis CE, Hillis AE. The function of the left anterior temporal pole: Evidence from acute stroke and infarct volume. Brain. 2011. 134: 3094-105
14. Umeoka K, Shirokane K, Mizunari T, Kobayashi S, Teramoto A. Dissecting aneurysm of the anterior temporal artery: Case report. Neurol Med Chir (Tokyo). 2011. 51: 777-80
15. Waldron JS, Sughrue ME, Hetts SW, Wilson SP, Mills SA, McDermott MW. Embolization of skull base meningiomas and feeding vessels arising from the internal carotid circulation. Neurosurgery. 2011. 68: 162-9
16. Yonas H, Agamanolis D, Takaoka Y, White RJ. Dissecting intracranial aneurysms. Surg Neurol. 1977. 8: 407-15


