

- Pars Advanced and Minimally Invasive Medical Manners Research Center, Pars Hospital, Iran University of Medical Sciences, Tehran, Iran.
DOI:10.25259/SNI_338_2019
Copyright: © 2019 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Abolfazl Rahimizadeh, Valiollah Hassani, Nima Mohsenikabir, Ava Rahimizadeh, Mona Karimi, Naser Asgari. Intraoperative tension pneumothorax during posterior vertebral column resection in a child with congenital scoliosis. 02-Aug-2019;10:155
How to cite this URL: Abolfazl Rahimizadeh, Valiollah Hassani, Nima Mohsenikabir, Ava Rahimizadeh, Mona Karimi, Naser Asgari. Intraoperative tension pneumothorax during posterior vertebral column resection in a child with congenital scoliosis. 02-Aug-2019;10:155. Available from: http://surgicalneurologyint.com/surgicalint-articles/9552/
Date of Submission
01-Jun-2019
Date of Acceptance
15-Jun-2019
Date of Web Publication
02-Aug-2019
Abstract
Background: Intraoperative tension pneumothorax (TPT) is extremely rare in spinal surgery overall and particularly in extensive deformity procedures. Here, we report a TPT occurring in conjunction with posterior vertebral column resection (pVCR) for the treatment of congenital scoliosis.
Case Description: A 12-year-old female undergoing congenital thoracic scoliosis surgery (e.g., pVCR) developed abrupt intraoperative increases in airway pressure and compromised hemodynamics that led to a TPT. This was directly attributed to an inadvertent pleural tear. Temporary drainage of the accumulated air was accomplished with a urethral catheter inserted directly into the pleural cavity. This was later supplemented with a standard chest tube. The child quickly improved and was routinely discharged a few days later.
Conclusion: In patients undergoing pVCR, if the surgical team is faced with unexplained hemodynamic instability and increased airway resistance, a TPT should be strongly suspected and appropriately managed.
Keywords: Complications, Congenital kyphoscoliosis, Posterior vertebral column resection, Spinal deformity, Tension pneumothorax
INTRODUCTION
Suk et al. (2002), Lenke et al., and Xie et al. reported on how to manage congenital kyphoscoliosis utilizing the posterior vertebral column resection (pVCR) technique.[
CASE REPORT
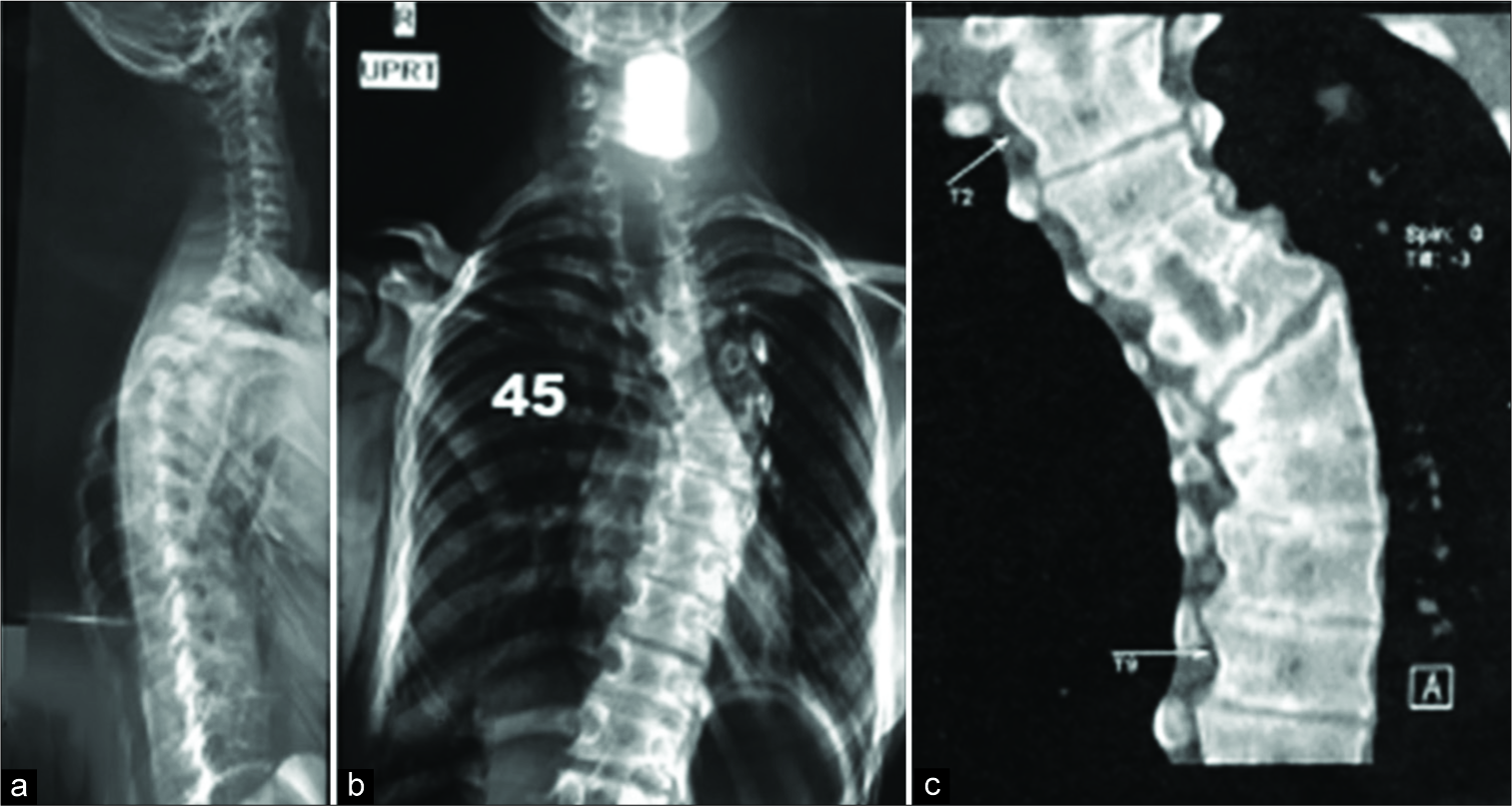
Over a 2-year period, a 12-year-old female with thoracic scoliosis failed conservative management. Dorsal spine X-rays documented thoracic scoliosis of 50° due to an abnormal T6 hemivertebra diagnosed on coronal computed tomography (CT) studies [
TPT/Chest tube
Suddenly the anesthesiologist noticed hemodynamic instability and asked us to close the wound. But, with removal of the retractor blade, we noticed a pleural tear through which the bubbles of air coming out. Using a size 14 urethral catheter, the trapped air in the pleural cavity was decompressed temporarily. As the result the ventilation improved, the blood pressure stabilized, and the cardiac status normalized., letting us the finish the job and close the wound. Then, the patient was turned to supine position and a chest radiograph was obtained showing a TPT on the right side with complete collapse of the right lung warranting chest tube placement [

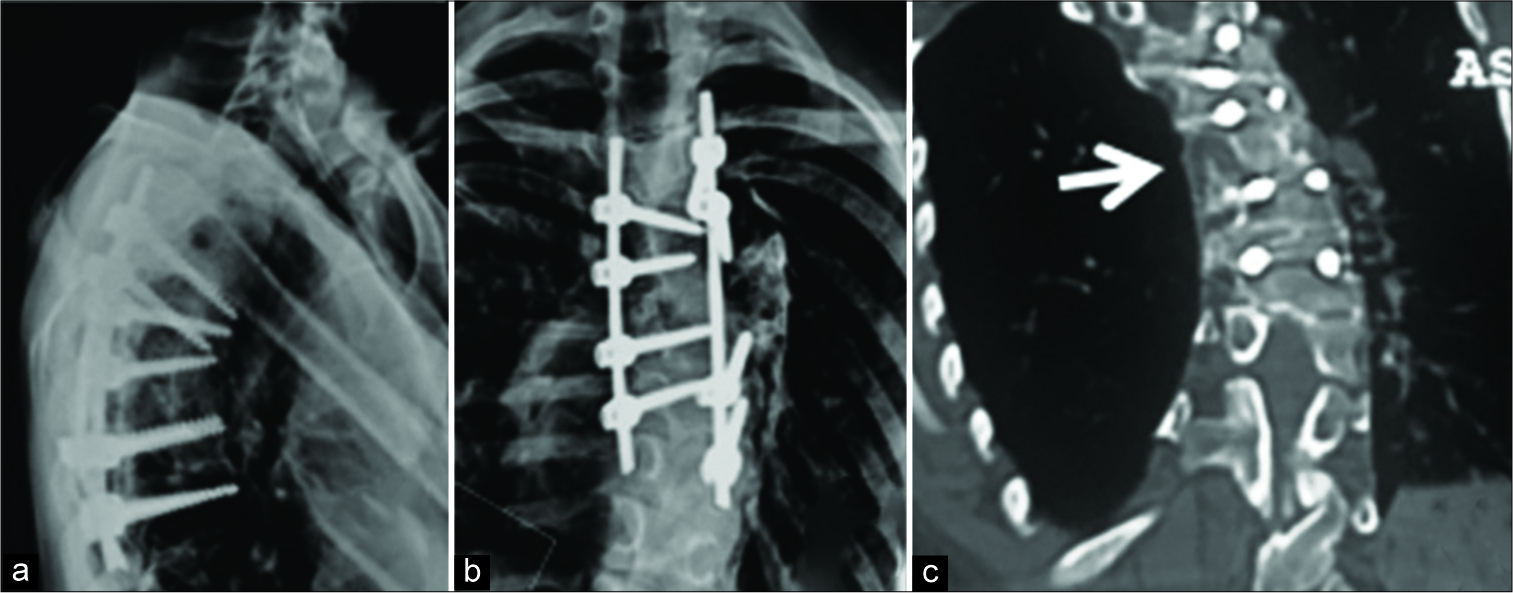
Figure 2:
Intra and post-operative portable chest X-rays; (a) OR – X-ray shows right-sided TPT and shrinkage of right lung (white arrows), (b) X-ray in OR, with a chest tube, the right lung is shrunken yet (white arrows), the tip of the chest tube is kinked, but a few minutes later, it was replaced; (c) a few days later, the lung is expanded and no pneumothorax is seen.
DISCUSSION
Pathogenesis
TPT is defined by an extensive, trapped, accumulation of air within the pleural space.[
Clinical picture
With a TPT, mediastinal shift results in acute decreased cardiac output as the venous circulation is blocked due to compression of the vena cava, atrium, and large veins.[
Diagnosis of TPT
TPT may occur with various etiologies that include airway disconnection, a plug in the airway, an allergic reaction, pulmonary emboli, an occult vascular injury, over-bleeding, and here, scoliosis surgery. The diagnosis of TPT in a patient under general anesthesia and in the prone position is challenging. TPT should be suspected by the anesthesiologist observing unexplained elevated airway pressures, the sudden fall of oxygen saturation, unilateral absence of breath sounds, and hypotension disproportionate to the intraoperative blood loss and is typically resistant to replacement therapy and inotropic drugs.[
Treatment
Emergent decompression of TPT is critical. Swift drainage of intrapleural air may utilize a large bore needle (e.g., performed through the second intercostal interspace in the midclavicular line).[
CONCLUSION
During congenital scoliosis surgery with pVCR technique, the pleura is typically exposed bilaterally. This increases the risk of TPT as pleural tearing may occur during disarticulation/ partial resection of the rib head at the corresponding costovertebral joints. Once TPT is suspected, it is imperative to immediately remove the trapped air from the lung cavity. This case report should reinforce recognition of TPT by both neurosurgeons and anesthesiologists involved in the surgical management of scoliosis.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given his consent for his images and other clinical information to be reported in the journal. The patient understands that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Auerbach JD, Lenke LG, Bridwell KH, Sehn JK, Milby AH, Bumpass D. Major complications and comparison between 3-column osteotomy techniques in 105 consecutive spinal deformity procedures. Spine (Phila Pa 1976). 2012. 37: 1198-210
2. Dalvi PN, Virkar DN. Pneumothorax in a patient posted for cervical spine surgery. Res Innov Anesth. 2016. 1: 32-4
3. Gustman P, Yerger L, Wanner A. Immediate cardiovascular effects of tension pneumothorax. Am Rev Respir Dis. 1983. 127: 171-4
4. Kim SS, Cho BC, Kim JH, Lim DJ, Park JY, Lee BJ. Complications of posterior vertebral resection for spinal deformity. Asian Spine J. 2012. 6: 257-65
5. Lee JY, Kim JU, An EH, Song E, Lee YM. Bilateral tension pneumothorax caused by an abrupt increase in airway pressure during cervical spine surgery in the prone position a case report. Korean J Anesthesiol. 2011. 60: 373-6
6. Lenke LG, O’Leary PT, Bridwell KH, Sides BA, Koester LA, Blanke KM. Posterior vertebral column resection for severe pediatric deformity: Minimum two-year follow-up of thirty-five consecutive patients. Spine (Phila Pa 1976). 2009. 34: 2213-21
7. Lenke LG, Sides BA, Koester LA, Hensley M, Blanke KM. Vertebral column resection for the treatment of severe spinal deformity. Clin Orthop Relat Res. 2010. 468: 687-99
8. Li G, Lv G, Passias P, Kozanek M, Metkar US, Liu Z. Complications associated with thoracic pedicle screws in spinal deformity. Eur Spine J. 2010. 19: 1576-84
9. Liang J, Qiu G, Shen J, Zhang J, Wang Y, Li S. Predictive factors of postoperative pulmonary complications in scoliotic patients with moderate or severe pulmonary dysfunction. J Spinal Disord Tech. 2010. 23: 388-92
10. Lonstein JE, Denis F, Perra JH, Pinto MR, Smith MD, Winter RB. Complications associated with pedicle screws. J Bone Joint Surg Am. 1999. 81: 1519-28
11. Mavarez-Martinez A, Soghomonyan S, Sandhu G, Rankin D. Intraoperative tension pneumothorax in a patient with remote trauma and previous tracheostomy. J Investig Med High Impact Case Rep. 2016. 4: 2324709616636397-
12. Rahimizadeh A, Rahimizadeh A. Management of traumatic double-level spondyloptosis of the thoracic spine with posterior spondylectomy: Case report. J Neurosurg Spine. 2015. 23: 715-20
13. Rankin D, Mathew PS, Kurnutala LN, Soghomonyan S, Bergese SD. Tension pneumothorax during surgery for thoracic spine stabilization in prone position: A case report and review of literature. J Investig Med High Impact Case Rep. 2014. 2: 2324709614537233-
14. Roush TF, Crawford AH, Berlin RE, Wolf RK. Tension pneumothorax as a complication of video-assisted thorascopic surgery for anterior correction of idiopathic scoliosis in an adolescent female. Spine (Phila Pa 1976). 2001. 26: 448-50
15. Rutherford RB, Hurt HH, Brickman RD, Tubb JM. The pathophysiology of progressive, tension pneumothorax. J Trauma. 1968. 8: 212-27
16. Schwab FJ, Hawkinson N, Lafage V, Smith JS, Hart R, Mundis G. Risk factors for major peri-operative complications in adult spinal deformity surgery: A multi-center review of 953 consecutive patients. Eur Spine J. 2012. 21: 2603-10
17. Suk SI, Kim JH, Kim WJ, Lee SM, Chung ER, Nah KH. Posterior vertebral column resection for severe spinal deformities. Spine (Phila Pa 1976). 2002. 27: 2374-82
18. Viswanathan A, Relyea K, Whitehead WE, Curry DJ, Luerssen TG, Jea AJ. Pneumothorax complicating. “in-out-in” thoracic pedicle screw placement for kyphotic deformity correction in a child: Case report. J Neursurg Pediartr. 2008. 2: 379-84
19. Weiss HR, Goodall D. Rate of complications in scoliosis surgery a systematic review of the pub med literature. Scoliosis. 2008. 3: 9-
20. Xie J, Li T, Wang Y, Zhao Z, Zhang Y, Bi N. Change in cobb angle of each segment of the major curve after posterior vertebral column resection (PVCR): A preliminary discussion of correction mechanisms of PVCR. Eur Spine J. 2012. 21: 705-10


