

- Department of Neurosurgery, Liaquat National Hospital and Medical College, Institute of Postgraduate Studies and Medical Sciences, Karachi, Pakistan
Correspondence Address:
Salman Sharif
Department of Neurosurgery, Liaquat National Hospital and Medical College, Institute of Postgraduate Studies and Medical Sciences, Karachi, Pakistan
DOI:10.4103/sni.sni_72_17
Copyright: © 2017 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Afifa Afsar, Mohsin Qadeer, Salman Sharif. Surgically treated spinal metastases: Do prognostic scores have a role?. 25-Jul-2017;8:158
How to cite this URL: Afifa Afsar, Mohsin Qadeer, Salman Sharif. Surgically treated spinal metastases: Do prognostic scores have a role?. 25-Jul-2017;8:158. Available from: http://surgicalneurologyint.com/?post_type=surgicalint_articles&p=8508
Date of Submission
16-Feb-2017
Date of Acceptance
07-Apr-2017
Date of Web Publication
25-Jul-2017
Abstract
Background:The outcome for patients with metastatic disease in spine is difficult to predict. Multiple scoring systems were utilized in this study to determine their effectiveness in predicting long-term prognoses.
Methods:A retrospective analysis of surgically treated patients of spinal metastasis was performed between 2005 and 2016. Data were collected prospectively during which 8 patients were lost to follow-up. Ultimately, data from 63 patients were reviewed. Treatment and prognoses were analyzed utilizing various scoring systems including the SINS, the Tomita, the modified Tokouhashi and Bauer scores.
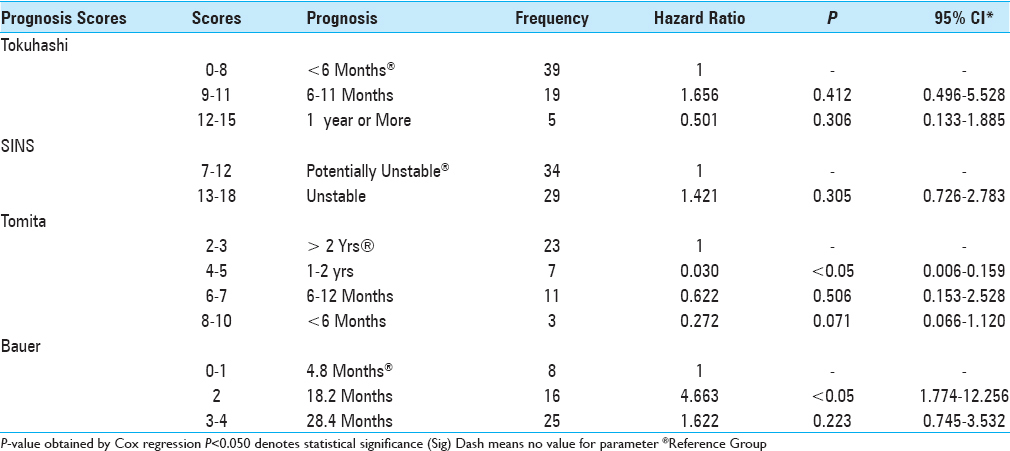
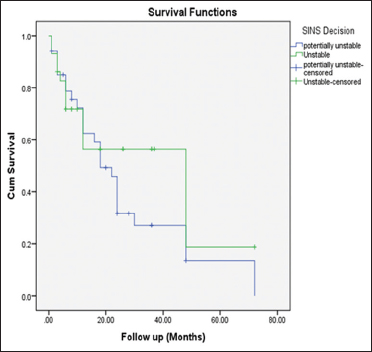
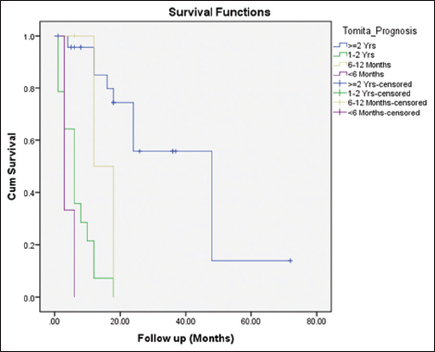
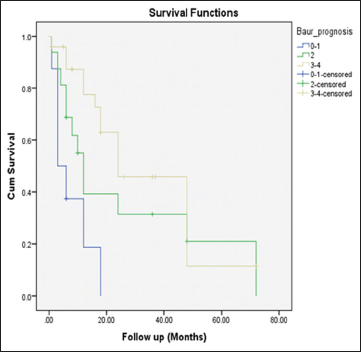
Results:Records of 63 patients, averaging 54 years of age, were analyzed. The Tomita score was applied in 44 patients, a modified Bauer score was studied in 49 patients, while SINS and modified Tokouhashi scores were calculated in all 63 patients. The hazard ratios for the Tomita score were 1, 0.030, 0.622, and 0.272, respectively. The hazard ratios for the modified Bauer scores were 1, 4.663, and 1.622, respectively. The Tokouhashi ratios were 1, 1.656, and 0.501, respectively. Of interest, the Tomita scores provided the highest statistical significance (P = 0.000) followed by the Bauer (P = 0.002) and Tokuhashi scores (P = 0.003). Notably, the SINS score showed no significant correlation in predicting patient survival.
Conclusion:For evaluating the metastatic spine disease, this study evaluated the prognostic efficacy of four widely used scores: the Tomita, score, the modified Tokouhashi and Bauer scores, and the SINS scores. The Tomita scores provided the highest statistical significance, followed by the Bauer, and Tokuhashi scores, while the SINS score showed no significant correlation in predicting patient survival.
Keywords: Bauer, metastases of spine, prognosis, scoring system, Tokouhashi, Tomita
INTRODUCTION
Spine is the most common site of bone metastases. Knowledge of survival of the individual can help predict the subsequent disease course. Patients with a predicted survival of 3 to 6 months may not be suitable candidates for surgical intervention.[

MATERIALS AND METHODS
Database of 63 patients
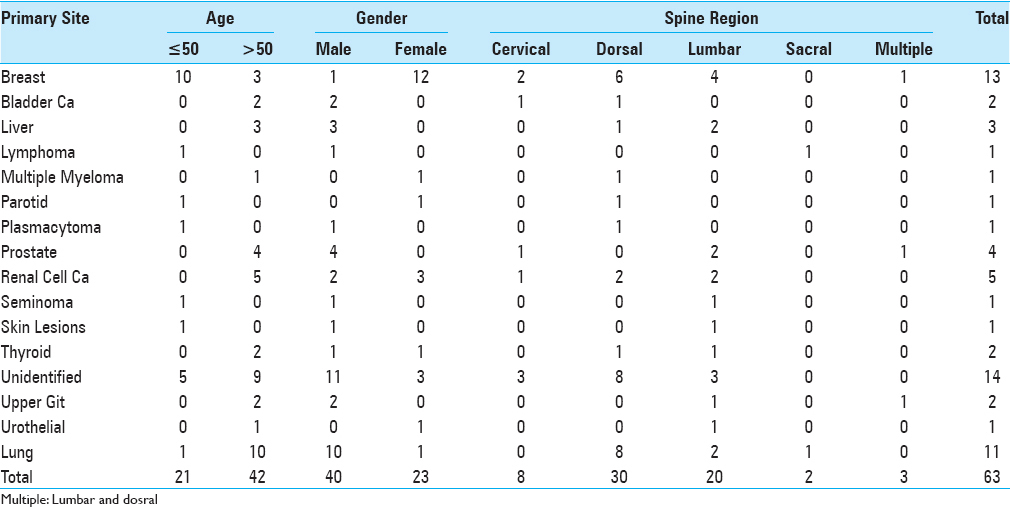
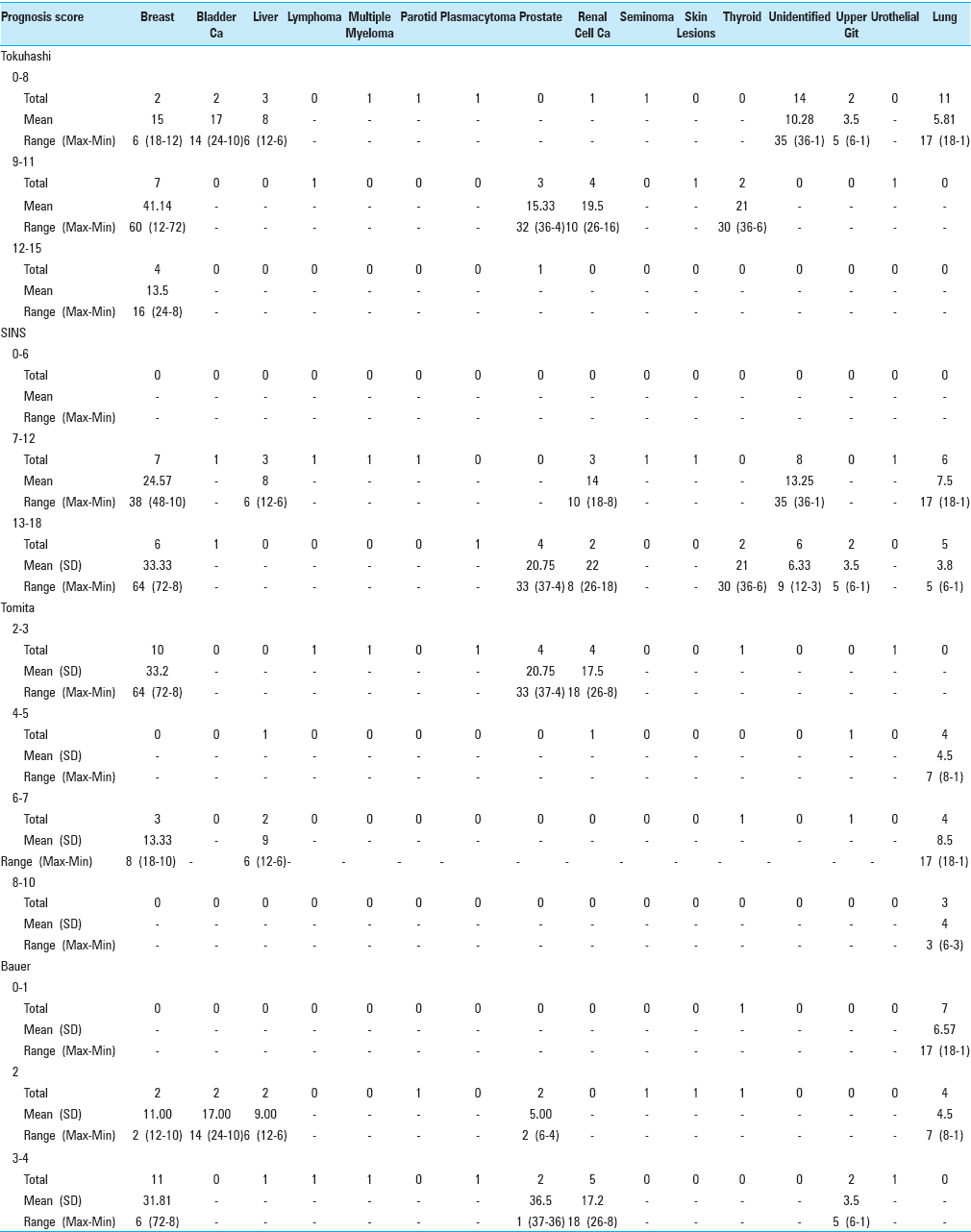
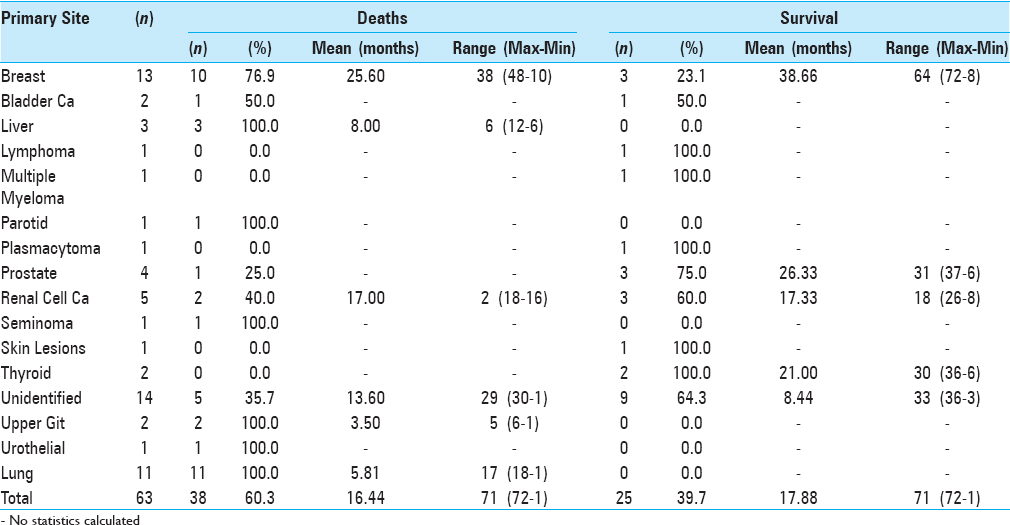
We prospectively collected data and outcomes for 63 patients with spinal metastasis who underwent surgery between 2005 and 2016. Patients, averaging 53.73 years of age, were followed for an average of 18 months (range 1–72 months), with a minimum follow-up of 6 months. Spinal metastasis were located in the cervical spine (8 patients), dorsal spine (30 patients), lumbar spine (20 patients), and sacrum (two patients). Multiple regions were involved in three patients. The most common types of primary malignancy were breast (13 patients) and lung cancers (11 patients). In 14 patients, the primary site was unidentified, of which 6 were labeled as adenocarcinomas [
Preoperative radiographic assessment
All patients were evaluated pre operatively with plain radiographs, computed tomography (CT), and magnetic resonance imaging of the spine. Bone scintigraphy and a CT of the chest and abdomen were also performed to evaluate the extent of systemic metastases. Patients were selected for surgery based on: (i) expected survival of more than 6 months, (ii) exacerbating pain, (iii) presence of neurological deficits, and (iv) instability. The authors studied multiple preoperative variables: age, gender, the type of primary malignancy, symptoms and their duration, the involved spinal level, neurological status, and the type of surgical procedure offered.
Staging of disease utilizing multiple systems
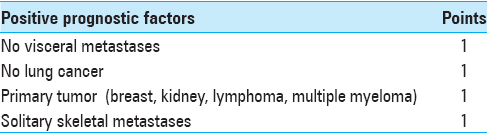
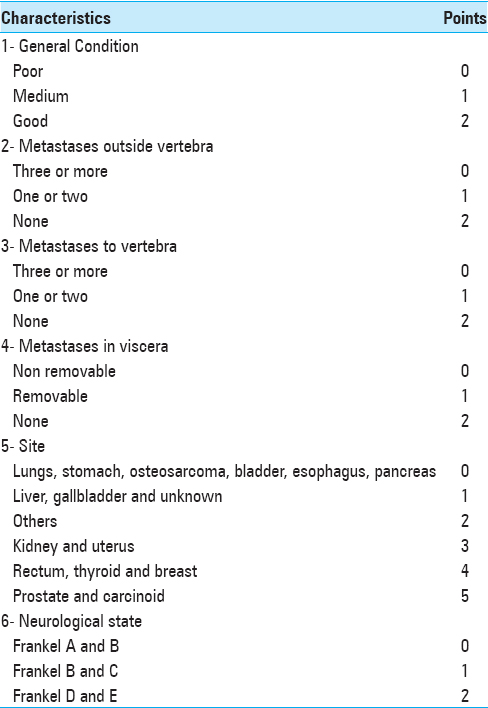
Treatment and prognosis were analyzed utilizing the SINS, Tomita, modified Tokouhashi, and modified Bauer scores. We then compared these scores with the actual documented survival (i.e., documented death or last documented hospital visit).
Statistical analysis
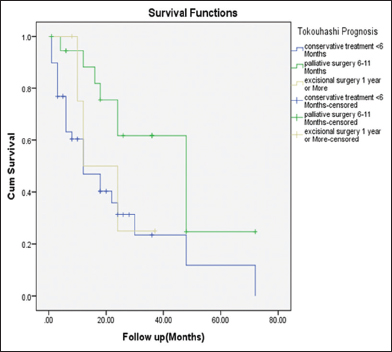
Data was examined using survival analysis. As the survival data was not uniformly distributed, the median duration of survival and its 95% confidence interval (CI) were used. Survival curves were estimated by means of the Kaplan–Meier methods. The predictive value of each scoring system was evaluated by using log-rank test. A P value of <0.050 was considered statistically significant. The log-rank test and Cox proportional hazards model were utilized to determine factor-influenced progression.
RESULTS
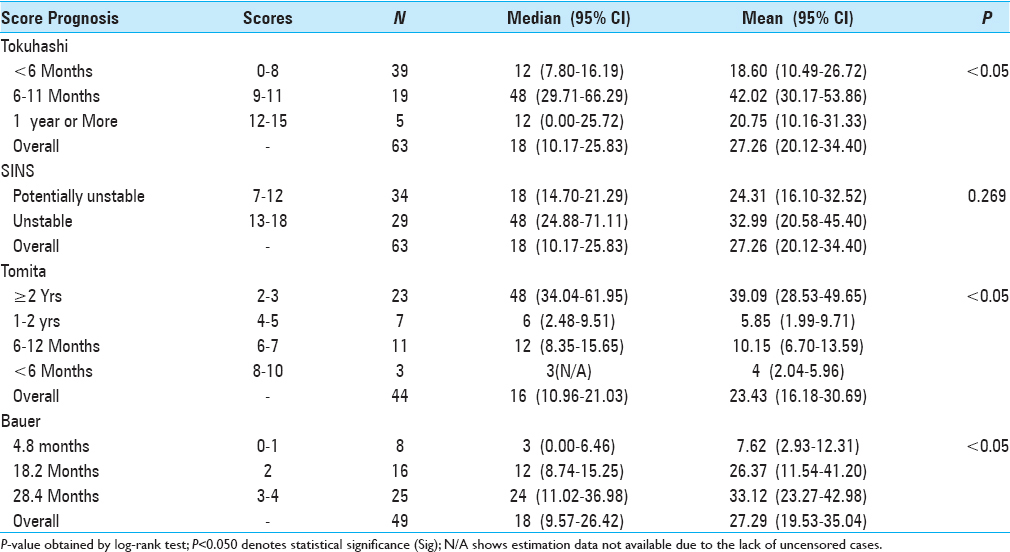
Survival analysis of each preoperative factor utilized the log rank test [

The Tokuhashi, Tomita, and Bauer scores provided statistically significant results, while those for SINS were not significant. The Tomita Score provided the highest statistical significance (P = 0.000) followed by the Bauer (P = 0.002) and Tokuhashi (P = 0.003) scores [Tables
Survival
The mean survival period was recorded according to the primary malignancy; breast correlated with a mean survival of 38.6 months, followed by prostate (26.33 months), and thyroid (21 months). Lung primaries were reported to have the worst prognosis, with a mean survival rate of only 5.81 months. [Tables
DISCUSSION
Estimating life expectancy in patients afflicted with spinal metastases is important. Management requires a multidisciplinary approach utilizing multimodality treatments options to address spinal metastases. It is important to evaluate these patients based upon universally accepted scientific criteria that can be replicable. Various prognostic scoring systems have been recommended[
Various surgical procedures can be performed in patients with spinal metastasis. Surgery should be reserved for patients with good or moderate prognosis, but not for prognoses of less than 3–6 months.[
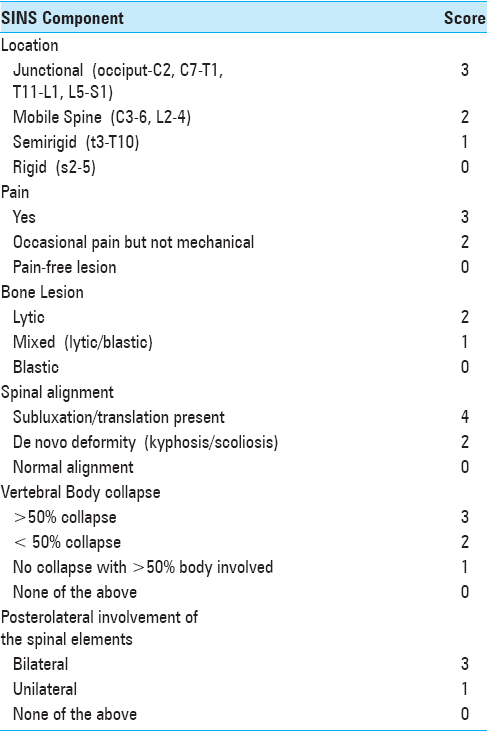
Metastases of the spine can cause significant instability, resulting in severe pain, progressive deformity and/or neurological compromise. SINS classification identifies patients with impending or existing spinal instability, for whom surgical intervention may be beneficial;[
Tokuhashi et al. designed a scoring system based on 6 prognostic factors, whereas the Tomita system was based on three simple factors: the grade of the primary malignancy, the presence of visceral metastases, and the presence of bone metastases. In both scoring systems, the type or grade of the primary malignancy is the most important factor affecting survival.[
In our study, four prognostic scoring systems were compared in patients with spinal metastases. The Bauer and Tomita scoring systems have showed statistical significance in predicting survival vs. the other scores.[
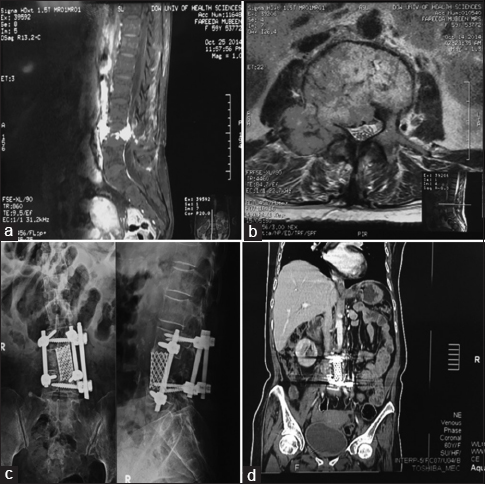
Figure 6
Case 1: A 60-year-old female presented with back pain and bilateral leg radiation for 8–9 months and unable to walk for 1 week. MRI lumbosacral spine showed a leftrenal mass involving whole of L4 vertebra. She underwent left kidney nephrectomy and L4 corpectomy, followed by L3-5 pedicle screw fixation with cage placement and anterior interbody screws. She had a Modified Tokouhashi score of 10, Modified Bauer 4, Tomita score 3 and SINS score of 14. All the scales estimated an overall survival of around 12 months for this patient, hence was surgically treated with good results. (a) MRI lumbosacral spine (sagittal view) showing contrast enhancing lesion involving L4 vertebra. (b) Axial view of the same patient showing the diseased level. (c) Postoperative X-rays lumbosacral spine (AP and lateral views) showing L3-5 pedicle and anterior interbody screws. (d) Postoperative coronal CT scan showing the same
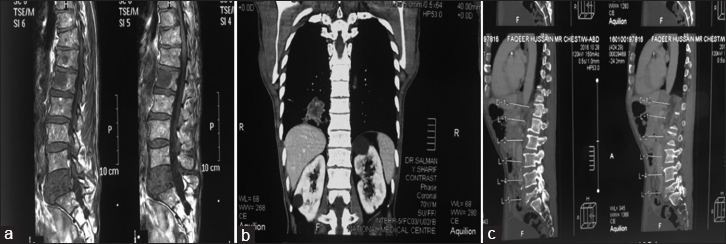
Figure 7
Case 2: A 60-year-old male with back pain and sciatica for 1 month. He had diffuse metastatic disease with Lung lesion and liver and bone metastases. He had a stable posterior column and L5 compression. This patient was managed conservatively. His Modified Tokouhashi score- 4, Tomita-10, Modified Bauer-1 and SINS score 14. The prognostic scores estimated his survival to be less than 6 months; hence this patient was managed conservatively. (a) MRI dorsolumbar spine (sagittal view) showing spinal metastases at L5 and L1. (b) Coronal CT chest showing the primary lesion involving lower zone of right lung. (c) Sagittally reconstructed CT of lumbosacral spine showing compression of L5 vertebra
Analysis of our study showed that breast lesions were most common followed by lung. Like many other series, lung cancer showed the worst prognosis.[
CONCLUSION
Of the four widely used scores to assess the extent of metastatic disease to the spine, the Tomita, the modified Tokouhashi and the Bauer, demonstrated statistically significant predictive results. Alternatively, the SINS scoring system, though a good indicator for choosing patients for surgery, lacked statistical significance in predicting survival.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Arana E, Kovacs F, Royuela A, Asenjo B, Pérez-Ramírez U, Zamora J. Agreement in the assessment of metastatic spine disease using scoring systems. Radiother Oncol. 2015. 115: 135-40
2. Aoude A, Amiot L. A comparison of the modified Tokuhashi and Tomita scores in determining prognosis for patients afflicted with spinal metastasis. Can J Surg. 2014. 57: 188-193
3. Dardic M, Wibmer C, Berghold A, Stadlmueller L, Froehlich E, Leithner A. Evaluation of prognostic scoring systems for spinal metastases in 196 patients treated during 2005–2010. Eur Spine J. 2014. 24: 2133-41
4. Goodwin C, Schoenfeld A, Abu-Bonsrah N, Garzon-Muvdi T, Sankey E, Harris M. Reliability of a spinal metastasis prognostic score to model 1-year survival. Spine J. 2016. 16: 1102-8
5. Katagiri H. Prognostic factors and a scoring system for patients with skeletal metastasis. J Bone Joint Surg. 2005. 87B: 698-703
6. Kim J, Lee S, Park S, Chung S, Kim E, Eoh W. Analysis of the predictive role and new proposal for surgical strategies based on the modified Tomita and Tokuhashi scoring systems for spinal metastasis. World J Surg Oncol. 2014. 12: 245-
7. Leithner A, Radl R, Gruber G, Hochegger M, Leithner K, Welkerling H. Predictive value of seven preoperative prognostic scoring systems for spinal metastases. Eur Spine J. 2008. 17: 1488-95
8. Tokuhashi Y, Matsuzaki H, Oda H, Oshima M, Ryu J. A revised scoring system for preoperative evaluation of metastatic spine tumor prognosis. Spine. 2005. 30: 2186-91
9. Tomita K, Kawahara N, Kobayashi T, Yoshida A, Murakami H, Akamaru T. Surgical strategy for spinal metastases. Spine. 2001. 26: 298-306
10. Wang M, Bünger C, Li H, Wu C, Høy K, Niedermann B. Predictive Value of Tokuhashi Scoring Systems in Spinal Metastases, Focusing on Various Primary Tumor Groups. Spine. 2012. 37: 573-82
11. Wibmer C, Leithner A, Hofmann G, Clar H, Kapitan M, Berghold A. Survival analysis of 254 patients after manifestation of spinal metastases: Evaluation of seven preoperative scoring systems. Spine. 2011. 36: 1977-86
12. Yilmazlar S, Dogan S, Caner B, Turkkan A, Bekar A, Korfali E. Comparison of prognostic scores and surgical approaches to treat spinal metastatic tumors: A review of 57 cases. J Orthop Surg Res. 2008. 3: 37-

