

- Faculty of Medicine, Pontifical Catholic University of Campinas, Campinas, São Paulo, Brazil
- Department of Neurosurgery of Hospital e Maternidade Celso Pierro, Pontifical Catholic University of Campinas, Campinas, São Paulo, Brazil
Correspondence Address:
Telmo Augusto Barba Belsuzarri
Department of Neurosurgery of Hospital e Maternidade Celso Pierro, Pontifical Catholic University of Campinas, Campinas, São Paulo, Brazil
DOI:10.4103/2152-7806.185778
Copyright: © 2016 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Pozetti M, Barba Belsuzarri TA, B. Belsuzarri NC, Seixas NB, João F. M. Araujo. Neurofibromatosis type 1 and Chiari type 1 malformation: A case report and literature review of a rare association. Surg Neurol Int 07-Jul-2016;7:
How to cite this URL: Pozetti M, Barba Belsuzarri TA, B. Belsuzarri NC, Seixas NB, João F. M. Araujo. Neurofibromatosis type 1 and Chiari type 1 malformation: A case report and literature review of a rare association. Surg Neurol Int 07-Jul-2016;7:. Available from: http://surgicalneurologyint.com/surgicalint_articles/neurofibromatosis-type-1-chiari-type-1-malformation-case-report-literature-review-rare-association/
Abstract
Background:The association between neurofibromatosis type 1 (NF-I) and Chiari I malformation (CMI) is rare, and not many studies are reported in the literature. Performing magnetic resonance imaging (MRI) in patients with NF-1 is essential because several cases of Chiari type I are completely asymptomatic. We emphasize the need for inclusion of Chiari I as diagnosis in association with NF-1.
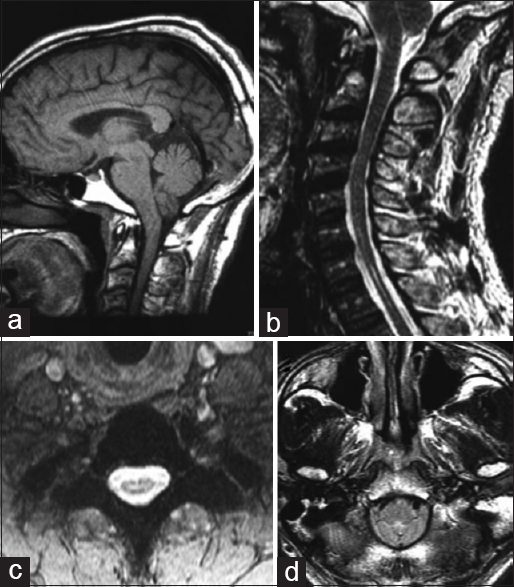
Case Description:The patient was a 51-year-old black man who presented with complaints of pain and decreased motion and sensibility of his hands, wrists, and forearms, along with progressive dysarthria. Even though the computed tomography (CT) scan of the skull did not show changes, the MRI showed hydro/syringomyelia in the cervical spine area. Midline suboccipital craniectomy with total laminectomy of c1 and partial laminectomy of c2 was performed; tonsillectomy was also performed for cistern expansion because of intense thickening and obliteration of the obex by the cerebellar tonsils. Following treatment, the patient showed remission of symptoms.
Conclusion:NF-1 in association with CMI is rare, and early diagnosis and surgical treatment are essential to slow down the myelopathy; although they prevent neurological damages, patients with NF-1 must remain under doctor's attention in case of association with CMI. Our literature review showed that symptoms can vary and include headache, gait disturbance, and sensory/motor diminution, until asymptomatic patients. Moreover, the incidence of NF-1 is considerably higher in CMI patients in comparison to the global incidence (8.6–11.8% and 0.775%, respectively). The surgical technique must be evaluated case by case according to the degree of cerebrospinal fluid obstruction.
Keywords: Chiari 1 malformation, neurofibromatosis type 1, syringomyelia
INTRODUCTION
Neurofibromatosis type 1 (NF-1) or Von Recklinghausen's disease is one of the most common neurocutaneous disorders well-known to cause skin lesions (mainly tumors, cafe-au-lait spots, and a wide variety of brain dysplasia) in affected patients.[
Chiari I malformation (CMI) causes herniation of the cerebellar tonsils through the foramen magnum, generating diverse clinical conditions, which are usually complicated by syringomyelia.[
Several theories attempt to explain the origin of the Chiari's malformations such as the hindbrain dysgenesis, development arrest, caudal traction, hydrocephalus theory/Gardner theory, small posterior fossa, and lack of embryologic ventricular distention theories. Probably, the pathophysiology of CMI and Chiari's Malformation type II (CMII) are different, but with the same impaired cerebral spinal fluid (CSF) impairment flow through the foramen magnum.[
CASE PRESENTATION
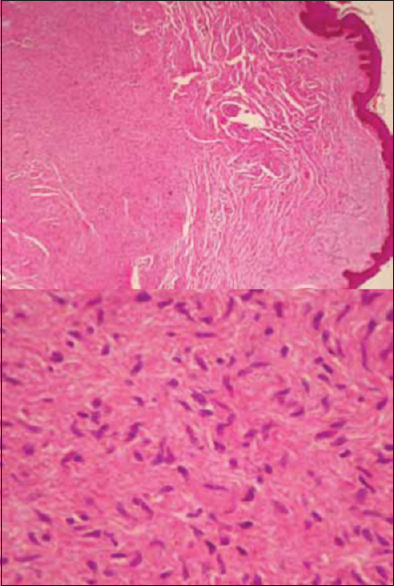
The patient was a 51-year-old black man who was previously diagnosed with NF-1, however, there was no history of cutaneous biopsy performed earlier. He sought medical attention in July 2014 with complaints of pain and decreased motion and sensation of hands, wrists, and forearms, in addition to difficulty in articulating words. Upon first checkup, the patient had several cafe-au-lait spots in variable sizes, larger than 15 mm, and several neurofibromas, in particular on his thorax, arms, and face [


DISCUSSION
NF-1 is the most common neurocutaneous syndrome characterized by various cutaneous stigma associated with neurological manifestations and a greater susceptibility to tumors.[
The patient mentioned in this study had the central cord syndrome, a condition that affects neurons in the gray matter and spinothalamic tract, causing loss of motion and sensation in arms and hands. It can also cause segmental weakness and signs of long tract (upper motor neuron lesion). The paralysis of the lower cranial nerves occurs in 11% of cases (in this case, accessory nerve and hypoglossal nerve).[
The real incidence of CMI is not known, but a study of general population who underwent brain MRI showed that, in 22591 patients, approximately 175 (0.775%) presented tonsilar herniation greater than 5 mm.[
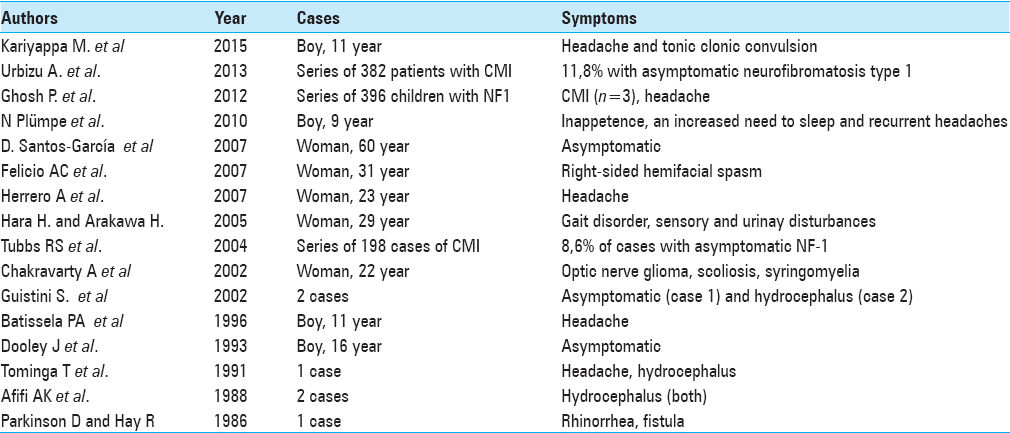
In the literature review, approximately 80 patients of both diseases were analyzed. Approximately 80% of the patients were asymptomatic, 9% only had cluster headache, and the others had various health problems such as facial spasms, tonic–clonic seizures, urinary disturbances, and sleep disorders. In the review, precocity of symptoms in males (children and teenagers mostly) was noticed compared to females (predominance in young adults)[
CONCLUSION
NF-1 in combination with CMI is rare and early diagnosis and surgical treatment are essential to slow down myelopathy as well as to prevent neurological damages. Patients with NF-1 must remain under doctor's attention in case of association with CMI. Asymptomatic patients can be monitored and operated if they become symptomatic. In patients with recommendation of surgery, the surgical technique must be evaluated case by case according to the degree of CSF obstruction and the associated clinical condition.[
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Acosta MT, Walsh KS, Kardel PG, Kutteruf RE, Bhatt RR, Bouton TC. Cognitive profiles of neurofibromatosis type 1 patients with minor brain malformations. Pediatr Neurol. 2012. 46: 231-4
2. Al-Otibi M, Rutka JT. Neurosurgical implications of neurofibromatosis type I in children. Neurosurg Focus. 2006. 20: E2-
3. Ars E, Kruyer H, Morell M, Pros E, Serra E, Ravella A. Recurrent mutations in the NF1 gene are common among neurofibromatosis type 1 patients. J Med Genet. 2003. 40: e82-
4. Battistella PA, Perilongo G, Carollo C. Neurofibromatosis type 1 and type I Chiari malformation: An unusual association. Childs Nerv Syst. 1996. 12: 336-8
5. Boyd KP, Korf BR, Theos A. Neurofibromatosis type 1. J Am Acad Dermatol. 2009. 61: 1-16
6. Felício AC, Godeiro-Junior CO, Borges V, Silva SMA, Ferraz HB. Hemifacial Spasm in a patient with neurofibromatosis and Arnold-Chiari malformation. Arq Neuropsiquiatr. 2007. 65: 855-7
7. Hara H, Arakawa H. Coexistence of neurofibromatosis 1 and Chiari type I malformation: An unusual association. J Dermatol. 2005. 32: 34-7
8. Incecık F, Ozlem HM, Altunbasak S. Optic pathway glioma, scoliosis, Chiari type 1 malformation, and syringomyelia in a patient with neurofibromatosis type 1. J Neurosci Rural Pract. 2013. 4: 141-3
9. Korf BR, Schneider G, Poussaint TY. Structural anomalies revealed by neuroimaging studies in the brains of patients with neurofibromatosis type 1 and large deletions. Genet Med. 1999. 1: 136-40
10. Loukas M, Shayota BJ, Oelhafen K, Miller JH, Chern JJ, Tubbs RS. Associated disorders of Chiari Type I malformations: A review. Neurosurg Focus. 2011. 31: E3-
11. Santos-García D, Cabanillas M, Suárez-Dono I, Monteagudo B, Fuente-Fernández RDL, Suárez-Amor O. Neurofibromatosis type 1 and Arnold-Chiari malformation. Actas Dermosifiliogr. 2009. 100: 817-32
12. Tubbs RS, Beckman J, Naftel RP, Chern JJ, Wellons JC, Rozzelle CJ. Institutional experience with 500 cases of surgically treated pediatric Chiari malformation Type I. J Neurosurg Pediatr. 2011. 7: 248-56
13. Tubbs RS, Pugh JA, Oakes WJ.editors. Chiari Malformations. Youmans Neurological Sugery. Philadelphia: Elsevier Saunders; 2011. II: 1918-27
14. Tubbs RS, Rutledge SL, Kosentka A, Bartolucci AA, Oakes WJ. Chiari I malformation and neurofibromatosis type 1. Pediatr Neurol. 2004. 30: 278-80
15. Urbizu A, Toma C, Poca MA, Sahuquillo J, Cuenca-León E, Cormand B. Chiari Malformation Type I: A Case-Control Association Study of 58 Developmental Genes. PLoS One. 2013. 8: e57241-
16. Whitehouse D. Diagnostic Value of the Café-au-lait Spot in Children. Arch Dis Child. 1966. 41: 316-9

