

- Department of Neurosurgery, Erzurum Bolge Training and Research Hospital, Erzurum, Turkey
- Department of Neurosurgery, Safa Hospital, Istanbul, Turkey
- Department of Neurosurgery, Namık Kemal University Faculty of Medicine, Tekirdag, Turkey
Correspondence Address:
Mehmet S. Gürbüz
Department of Neurosurgery, Namık Kemal University Faculty of Medicine, Tekirdag, Turkey
DOI:10.4103/2152-7806.194495
Copyright: © 2016 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Mehmet O. Yüksel, Mehmet S. Gürbüz, Numan Karaarslan, Tezcan Caliskan. Rapidly progressing interhemispheric subdural empyema showing a three-fold increase in size within 12 hours: Case report. 21-Nov-2016;7:
How to cite this URL: Mehmet O. Yüksel, Mehmet S. Gürbüz, Numan Karaarslan, Tezcan Caliskan. Rapidly progressing interhemispheric subdural empyema showing a three-fold increase in size within 12 hours: Case report. 21-Nov-2016;7:. Available from: http://surgicalneurologyint.com/surgicalint_articles/rapidly-progressing-interhemispheric-subdural-empyema-showing-a-three%e2%80%91fold-increase-in-size-within-12-hours-case-report/
Date of Submission
26-Apr-2016
Date of Acceptance
28-Jul-2016
Date of Web Publication
21-Nov-2016
Abstract
Background:Subdural empyema is a rare form of intracranial infection. It is described as accumulation of purulent infective material between the inner layer of dura mater and outer layer of arachnoid membrane.
Case Description:A 17-year-old girl was admitted to the emergency department with acute left hemiplegia and was diagnosed with interhemispheric subdural empyema that showed a three-fold increase in size within 12 hours. Complete recovery was achieved with emergency surgical evacuation and additional 3 weeks of antibiotic treatment.
Conclusion:Subdural empyema should be diagnosed and managed early in time since it may progress very rapidly and can cause high morbidity and mortality. Complete recovery can be achieved if it is diagnosed early and treated in time.
Keywords: Increase in size, interhemispheric, rapidly progressing, subdural empyema
INTRODUCTION
Subdural empyema is an intracranial infection characterized by the accumulation of infective material between the inner layer of dura mater and outer layer of arachnoid membrane.[
Timely diagnosis and treatment of subdural empyema is very essential since it can progress very rapidly and can cause severe neurological impairment. Full recovery can be achieved when it is diagnosed and treated in time.[
CASE REPORT
A 17-year-old girl was admitted to the emergency department with the complaint of rapidly progressing weakness of her left arm and leg. Her medical history was unremarkable other than a history of intermittent sessions of antibiotic treatment for sinusitis. Her physical examination revealed a temperature of 37.6°C, pulse of 96, respiratory rate of 14, blood pressure of 118/74 mmHg, and an oxygen saturation of 100% on room air. Her head and neck examination demonstrated no sign of meningeal irritation, but showed sinus tenderness. She had left hemiplegia with a Glasgow coma score of 15 and normal pupillary examination.
Laboratory examination revealed elevated erythrocyte sedimentation rate (80 mm/h), a high level of C-reactive protein (7.8 mg/L), with 16 × 109/L white blood cells and 84% neutrophils. Cranial computed tomography (CT) and cranial magnetic resonance imaging (MRI) scans of the patient revealed interhemispheric subdural empyema and accompanying frontal and paranasal sinusitis [Figure
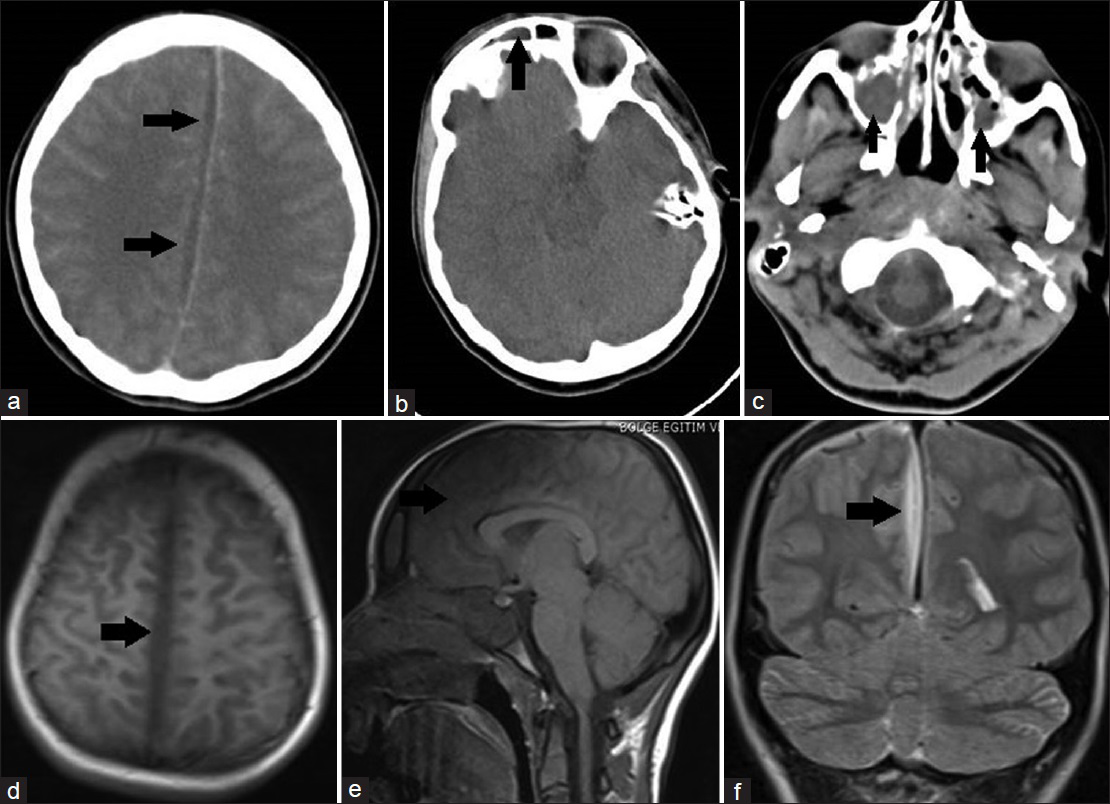
Figure 1
(a) Contrast-enhanced cranial axial computed tomography (CT) scan immediately taken on admission reveals interhemisferic subdural empyema indicated with black arrows. (b) On cranial axial CT scan immediately taken on admission, black arrow indicates frontal sinusitis. (c) On cranial axial CT scan immediately taken on admission, black arrows indicate bilateral paranasal sinusitis. (d) Cranial T-1 weighted axial magnetic resonance imaging (MRI) scan taken on admission reveals interhemisferic subdural empyema indicated with black arrow. (e) Cranial T-1 weighted sagittal MRI scan taken on admission reveals interhemisferic subdural empyema indicated with black arrow. (f) Cranial T-2 weighted coronal MRI scan taken on admission reveals interhemisferic subdural empyema indicated with black arrow
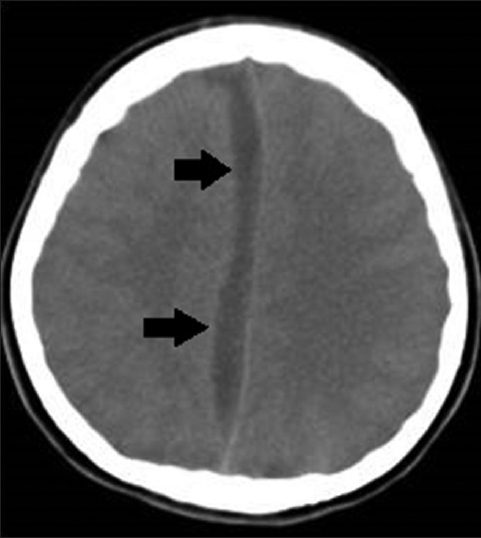
The patient was immediately taken to the operating theatre and subdural empyema was evacuated via parasagittal interhemispheric approach. Bone flap was not repositioned because it was seen to be contaminated with the infective material. Postoperative CT scan of the patient revealed that the empyema had been evacuated successfully [

DISCUSSION
The most common causes of subdural empyema are meningitis in children and otolaryngeal infections in adults.[
CT and MRI are the diagnostic tools of choice in subdural empyema.[
The goal of the treatment is the complete evacuation of the empyema and successful treatment of infection.[
Debate still exists regarding the ideal surgical technique. Though successful results with burr-hole drainage have been reported, surgical evacuation via craniotomy is still the most commonly preferred technique.[
Because of improved diagnostic tools such as CT and MRI, early diagnosis and treatment has reduced the morbidity and mortality rates.[
CONCLUSION
It should be noted that subdural empyema may have a rapidly progressive course, reaching a relatively large size in a very short time. Nonetheless, subdural empyema can be treated with excellent results in case of early diagnosis and timely management.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Alvis Miranda H, Castellar-Leones SM, Elzain MA, Moscote-Salazar LR. Brain abscess: Current management. J Neurosci Rural Pract. 2013. 4: 67-81
2. Bashir EF, Taha ZM. Challenges in the management of intracranial subdural empyema. Neurosurg Quart. 2003. 13: 198-206
3. Gordon B, Bernard W, Smith S. Treatment of subdural empyema. J Neurosurg. 1991. 55: 82-8
4. Maniglia AJ, Goodwin WJ, Arnold JE, Ganz E. Intracranial abscesses secondary to nasal, sinus, and orbital infections in adults and children. Arch Otolaryngol Head Neck Surg. 1989. 115: 1424-9
5. Mauser HW, Van Houwelingen HC, Tulleken CA. Factors affecting the outcome in subdural empyema. J Neurol Neurosurg Psychiatry. 1987. 50: 1136-41
6. Menon S, Bharadwaj R, Chowdhary A, Kaundinya DV, Palande DA. Current epidemiology of intracranial abscesses: A prospective 5 year study. J Med Microbiol. 2008. 57: 1259-68
7. Nathoo N, Nadvi SS, Narotam PK, Van Dellen JR. Brain Abscess: Management and Outcome Analysis of a Computed Tomography Era Experience with 973 Patients. World Neurosurg. 2011. 75: 716-26
8. Tewari MK, Sharma RR, Shiv VK, Lad SD. Spectrum of intracranial subdural empyemas in a series of 45 patients: Current surgical options and outcome. Neurol India. 2004. 52: 346-9
9. Tsai YD, Chang WN, Shen CC, Lin YC, Lu CH, Liliang PC. Intracranial suppuration: A clinical comparison of subdural empyemas and epidural abscesses. Surg Neurol. 2003. 59: 191-6
10. Tsou TP, Lee PI, Lu CY Chang LY, Huang LM, Chen JM. Microbiology and epidemiology of brain abscess and subdural empyema in a medical center: A 10-year experience. J Microbiol Immunol Infect. 2009. 42: 405-12
11. Tummala RP, Chu RM, Hall WA. Subdural empyema in children. Neurosurgery Quart. 2004. 14: 257-65
12. Wu TJ, Chiu NC, Huang FY. Subdural empyema in children–20-year experience in a medical center. J Microbiol Immunol Infect. 2008. 41: 62-7
13. Yilmaz N, Kiymaz N, Yilmaz C, Bay A, Yuca SA, Mumcu C. Surgical treatment outcome of subdural empyema: A clinical study. Pediatr Neurosurg. 2006. 42: 293-8

