

- Department of Clinical Neurosciences, Service of Neurosurgery, Centre Hospitalier Universitaire Vaudois,
- Department of Clinical Neurosciences, Spine Surgery Unit, Centre Hospitalier Universitaire Vaudois, Switzerland.
DOI:10.25259/SNI_376_2020
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Francois Borsotti1, Daniele Starnoni1, Timo Ecker2, Juan Barges Coll2. One-year follow-up for type II odontoid process fractures in octogenarians: Is there a place for surgical management?. 12-Sep-2020;11:285
How to cite this URL: Francois Borsotti1, Daniele Starnoni1, Timo Ecker2, Juan Barges Coll2. One-year follow-up for type II odontoid process fractures in octogenarians: Is there a place for surgical management?. 12-Sep-2020;11:285. Available from: https://surgicalneurologyint.com/?post_type=surgicalint_articles&p=10255
Date of Submission
22-Jun-2020
Date of Acceptance
20-Aug-2020
Date of Web Publication
12-Sep-2020
Abstract
Background: Type II odontoid fractures are becoming one of the most common injuries among elderly patients and are associated with increased morbidity rates. Here, we compared the safety/efficacy of conservative versus surgical treatment for type II C2 fractures and, in particular, evaluated the complications, hospital lengths of stay, and mortality rates for patients over 80 years of age.
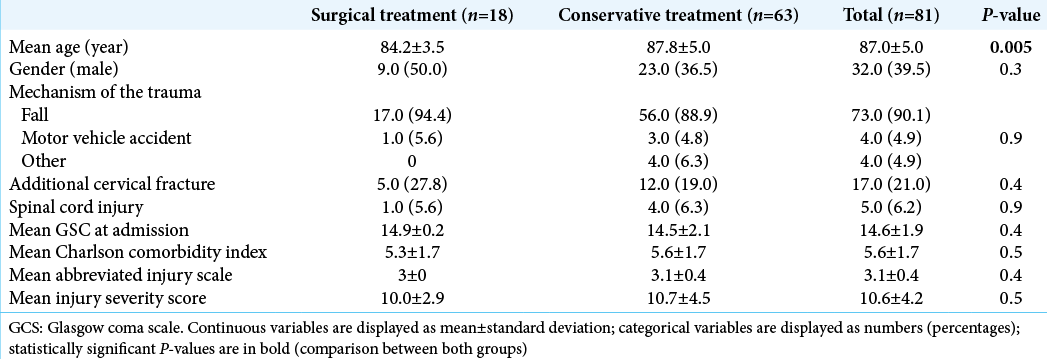
Methods: We retrospectively reviewed the records of 63 nonsurgically versus 18 surgically treated C2 fractures in patients over 80 years of age (2003–2018). Cervical computed tomography images, X-rays, and magnetic resonance images were reviewed by both a neurosurgeon and a neuroradiologist. The following patient data were included in the analysis; Glasgow Coma Scale score, injury severity score, the abbreviated injury scale scores, their comorbidities (e.g., utilizing the Charlson comorbidity index), their primary outcomes, and mortality rates (e.g., at 6 weeks and 1 year after treatment).
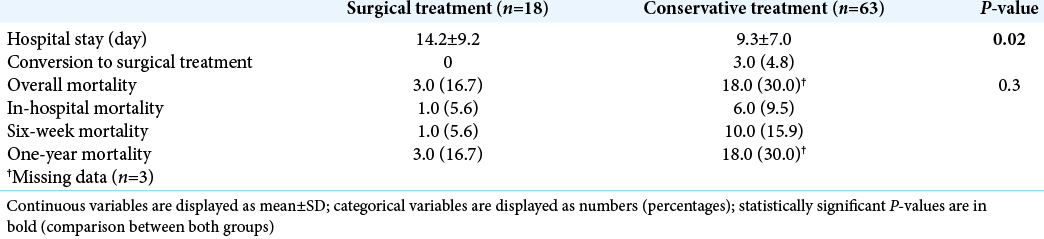
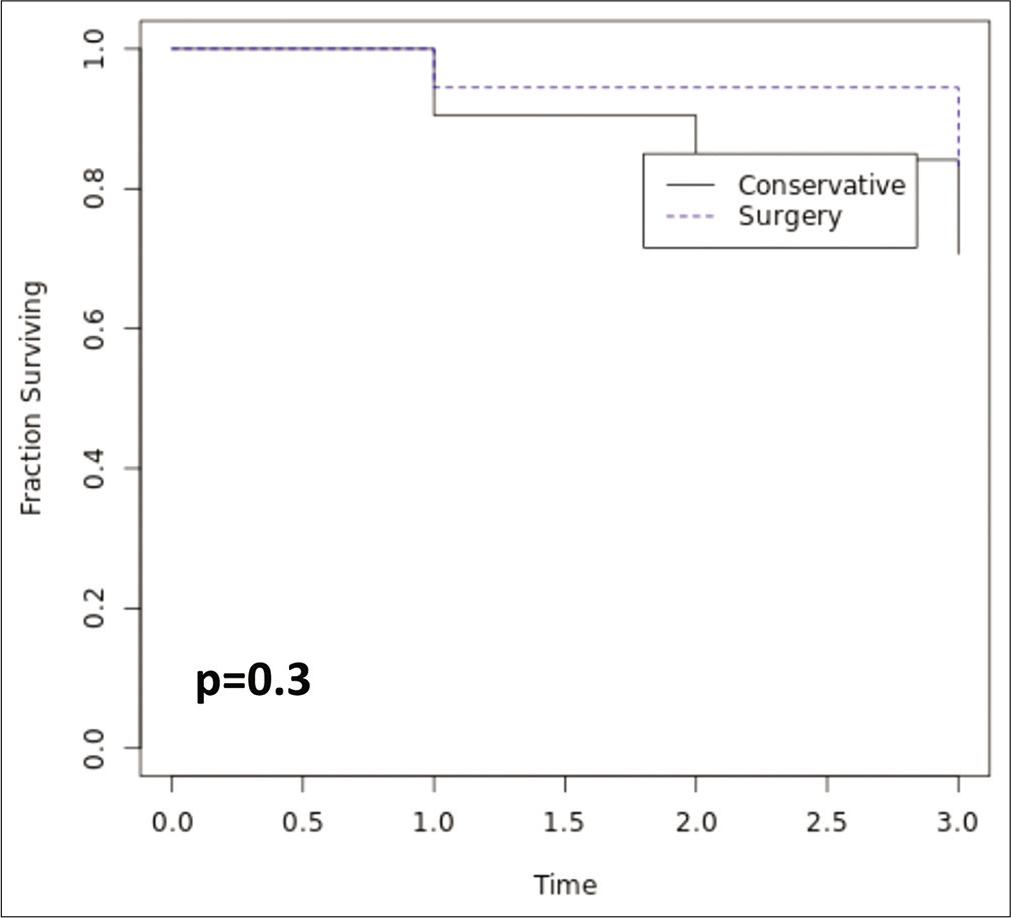
Results: Eighty-one patients were included in the study; 63 were treated conservatively and 18 underwent surgical management of type II C2 fractures. Patients averaged 87.0 ± 5.0 years of age, and their combined mortality rates were 13.6% at 6 weeks and 25.9% at 1 year. Notably, at 1 year, the mortality rates were not statistically different between the two groups: 18 (30.0%) patients from the conservatively treated group versus 3 (16.7%) patients from the surgically managed patients died indicating (e.g., using the Kaplan–Meier analysis) no survival advantage for either treatment strategy.
Conclusion: Surgical versus conservative management of type II odontoid fractures were associated with comparable high mortality rates at 1 year.
Keywords: Complications, Mortality, Nonoperative management, Octogenarians, Odontoid fractures, Surgical management
INTRODUCTION
Odontoid fractures are the most common fracture of the axis, the most common cervical spine fracture in the elderly and represent approximately 20% of all cervical fractures. Further, type II fractures (according to the classification of Anderson et D’Alonzo) represent more than 60% of all C2 fractures.[
Nonsurgical treatment using a rigid collar carries a significant risk of nonunion, fibrous union (pseudarthrosis),[
MATERIALS AND METHODS
Data acquisition
We retrospectively collected demographic data and assessed clinical scores e.g., the Glasgow Coma Scale, the abbreviated injury scale, the injury severity score (ISS), and the Charlson comorbidity index for 63 nonsurgically versus 18 surgically treated C2 fractures in patients over 80 years of age (2003–2018) [
Mortality rates were recorded at 6 weeks and 1 year in both groups and correlated with clinical scores, the type of treatment received, the length of hospital stay (LOS), and complication rates [
Patient population
We retrospectively reviewed a cohort of 81 consecutive patients older than 80 years old with type II C2 fractures (2003 and 2018); complete data were available for 96.3% of the patients [
Sixty-three patients (77.8%) were managed with a rigid cervical collar; of these, three patientsrays, and magnetic resonance imaging (MRI) were reviewed by both a neuroradiolo underwent delayed surgery an average of 199.6 days following their original presentation (range 172.0–214.0 days).
Eighteen (22.2%) patients had surgery; 14 patients underwent posterior C1-C2 fusion (Harms technique), while 4 had anterior odontoid screw fixation [

The mean age was 87 years old in both groups (range 80-99 years), but patients were significantly older in the conservative group [
Statistical analysis
Categorical variables were expressed as n (%), and continuous variables were expressed using the mean ± standard deviation. Statistical analysis included Student’s t-test and Fisher’s exact test. Long-term survival analysis was performed using the Kaplan–Meier method.
RESULTS
Data of both groups showed a longer LOS for surgical patients 14.2 ± 9.2 days versus the nonoperative group LOS of 9.3 ± 7.0 days (P = 0.02) [
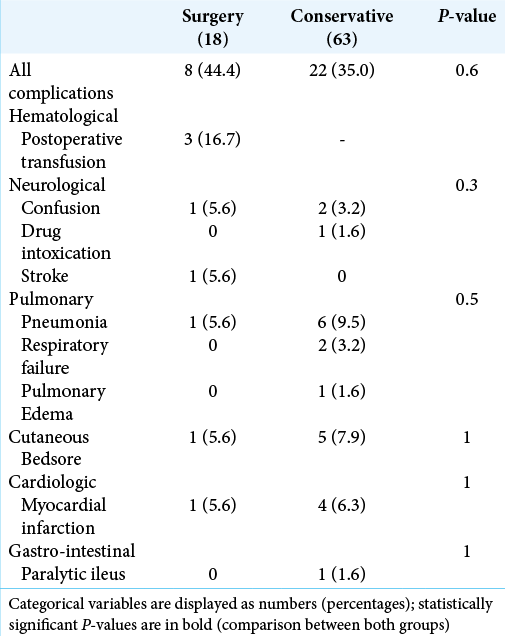
Major general complication rates were comparable for both groups; eight surgical patients (44.0%) versus 22 patients (35.0%) in the conservative group; rates were comparable for both groups: (P = 0.6) [
DISCUSSION
Odontoid type II fracture in octogenarians is associated with high mortality rates, with an overall 1-year mortality of up to 26%.[
CONCLUSION
Surgical versus conservative management of type II odontoid fractures were associated with comparable high mortality rates at 1 year. Based on our very small sample size of just 18 patients undergoing surgery for type II odontoid fractures versus 63 treated nonoperatively, we cannot offer a definitive recommendation for the optimal management of type II odontoid fractures in patients over 80 years of age.
Declaration of patient consent
Patient’s consent is not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Anderson LD, D’Alonzo RT. Fractures of the odontoid process of the axis. J Bone Joint Surg Am. 1974. 86: 2081
2. Chapman J, Smith JS, Kopjar B, Vaccaro AR, Arnold P, Shaffrey CI. The AOSpine North America geriatric odontoid fracture mortality study: A retrospective review of mortality outcomes for operative versus nonoperative treatment of 322 patients with long-term follow-up. Spine (Phila Pa 1976). 2013. 38: 1098-104
3. Gembruch O, Lemonas E, Ahmadipour Y, Sure U, El Hindy N, Dodel R. Treatment of odontoid Type II fractures in octogenarians: Balancing two different treatment strategies. Neurospine. 2019. 16: 360-7
4. Graffeo CS, Perry A, Puffer RC, Carlstrom LP, Chang W, Mallory GW. Deadly falls: Operative versus nonoperative management of Type II odontoid process fracture in octogenarians. J Neurosurg Spine. 2017. 26: 4-9
5. Hanigan WC, Powell FC, Elwood PW, Henderson JP. Odontoid fractures in elderly patients. J Neurosurg. 1993. 78: 32-5
6. Iyer S, Hurlbert RJ, Albert TJ. Management of odontoid fractures in the elderly: A review of the literature and an evidence-based treatment algorithm. Neurosurgery. 2018. 82: 419-30
7. Schoenfeld AJ, Bono CM, Reichmann WM, Warholic N, Wood KB, Losina E. Type II odontoid fractures of the cervical spine: Do treatment type and medical comorbidities affect mortality in elderly patients?. Spine (Phila Pa 1976). 2011. 36: 879-85
8. Waqar M, Van-Popta D, Barone DG, Sarsam Z. External immobilization of odontoid fractures: A systematic review to compare the halo and hard collar. World Neurosurg. 2017. 97: 513-7


