

- Department of Neurosurgery, Universidade do Estado do Rio de Janeiro,
- Department of Internal Medicine, Hospital Universitário Pedro Ernesto, Rio de Janeiro, Brazil.
- Department of Neurosurgery, Hospital Universitário Pedro Ernesto, Rio de Janeiro, Brazil.
Correspondence Address:
Domênica Baroni Coelho de Oliveira Ferreira, Department of Neurosurgery, Universidade do Estado do Rio de Janeiro, Brazil.
DOI:10.25259/SNI_822_2022
Copyright: © 2022 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Domênica Baroni Coelho de Oliveira Ferreira1, Juliana Weiler Medeiros1, Eduardo Cwajg2, Pedro Henrique Costa Ferreira-Pinto3, Leandro Ururahy de Carvalho3, Flávio Nigri3. Cavum septum pellucidum and vergae cyst: A symptomatic case with intracranial hypertension and multiple nerve involvement. 02-Dec-2022;13:564
How to cite this URL: Domênica Baroni Coelho de Oliveira Ferreira1, Juliana Weiler Medeiros1, Eduardo Cwajg2, Pedro Henrique Costa Ferreira-Pinto3, Leandro Ururahy de Carvalho3, Flávio Nigri3. Cavum septum pellucidum and vergae cyst: A symptomatic case with intracranial hypertension and multiple nerve involvement. 02-Dec-2022;13:564. Available from: https://surgicalneurologyint.com/?post_type=surgicalint_articles&p=12044
Date of Submission
07-Sep-2022
Date of Acceptance
21-Nov-2022
Date of Web Publication
02-Dec-2022
Abstract
Background: Cavum septum pellucidum (CSP) and cavum vergae (CV) are normal anatomical variations present in some children, adolescents, and adults. When the cavity is larger than normal, it is called a cyst. Symptomatic cases of CSP and CV cyst are rare, and the clinical presentation is varied. A case with multiple nerve involvement is described.
Case Description: A healthy 17-year-old female presented a sudden headache, right cervicobrachialgia, right ptosis, visual changes, and left facial paralysis over 10 days. Head magnetic resonance imaging revealed CSP and CV cyst. Inflammation, infection, and vascular disorders were ruled out. We decided to perform a right transfrontal endoscopic intraventricular septostomy and a right Monro foraminoplasty, which were successful. One month after surgery, the patient had no more signs or symptoms. She has remained asymptomatic for the past year.
Conclusion: Multiple nerve involvement was directly related to CSP and CV cyst. The cyst bilaterally occluded the foramen of Monro causing intracranial hypertension. It was possible to obtain complete resolution of the clinical features through neuroendoscopic fenestration and foraminoplasty.
Keywords: Cavum septum pellucidum, Cavum vergae, Cranial nerves palsy, Intracranial hypertension, Septum pellucidum
INTRODUCTION
The septum pellucidum (SP) is a thin, translucent, and triangular double membrane which separates the right and left frontal horns from the lateral ventricles of the brain. It extends between the anterior portion of the corpus callosum, and the body of the fornix and its width varies from 1.5 to 3.0 mm.[
The cavum septum pellucidum (CSP) and cavum vergae (CV) are persistent middle line structures of the adult brain that is formed when the proper closure of the membranous leaves of the SP does not occur completely. CV is the term used to designate the back extension of the CSP.[
It is considered a normal anatomical variation present in all premature babies and in 85% of full-term newborns, which usually disappears by 3–6 months of postnatal life. Nonetheless, 12% of children between 6 months and 16 years of age may continue to have it.[
When the cavity is larger than normal, it can be called a cyst. It is defined as a structure containing cerebrospinal fluid (CSF) between the lateral ventricles, whose walls are laterally arched rather than parallel and are 10 mm or more apart.[
In general, it is an incidental finding of imaging examinations (0.04%). However, when symptoms such as headache, behavioral disorders, cognitive impairment, convulsive syndrome, dizziness, hydrocephalus, nausea, and vomiting occur due to its presence, it is even rarer.[
The aim of this case report is to show exquisite clinical features of a symptomatic CSP and CV cyst in a young patient, successfully treated with neuroendoscopic fenestration and foraminoplasty.
CASE DESCRIPTION
A healthy 17-year-old female developed a holocranial headache, photophobia, nausea, vomiting, hypertension, and pain radiating from the right trapezius muscle to the ipsilateral wrist for 10 days. Three days later, she was hospitalized due to right eyelid ptosis, unilateral blurred vision, and worsening headache intensity. We found no abnormalities in her physiological, familial, and social history. The use of any drugs or medications, comorbidities, surgeries, traumas, and allergies was ruled out.
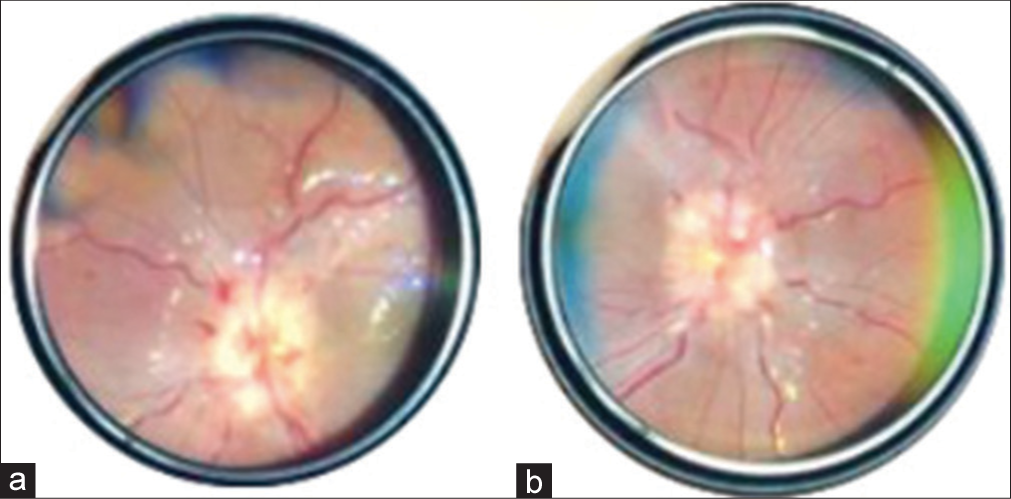
Physical examination revealed palsy of the right third nerve with the right eyelid ptosis, paralysis of the right medial rectus muscle, and ipsilateral mydriasis. She also had a right sixth nerve palsy with the right lateral rectus paresis and a left seventh nerve with the left peripheral facial paralysis. Fundoscopy showed bilateral papilledema [
Lumbar puncture performed after computed tomography (CT scan) that ruled out an absolute contraindication for this procedure, showed high opening pressure, and measured in more than 30 cm of water, but no findings of CSF infection were found. Other laboratory tests were negative for autoimmune and infectious diseases.
Cranial magnetic resonance imaging (MRI) demonstrated a CSP and CV cyst measuring 2.5 cm × 2.8 cm × 6.3 cm (longitudinal × transverse × anteroposterior) and an estimated volume of 22.93 cm3, which was causing bilateral obstruction of the foramen of Monro and consequent hydrocephalus [
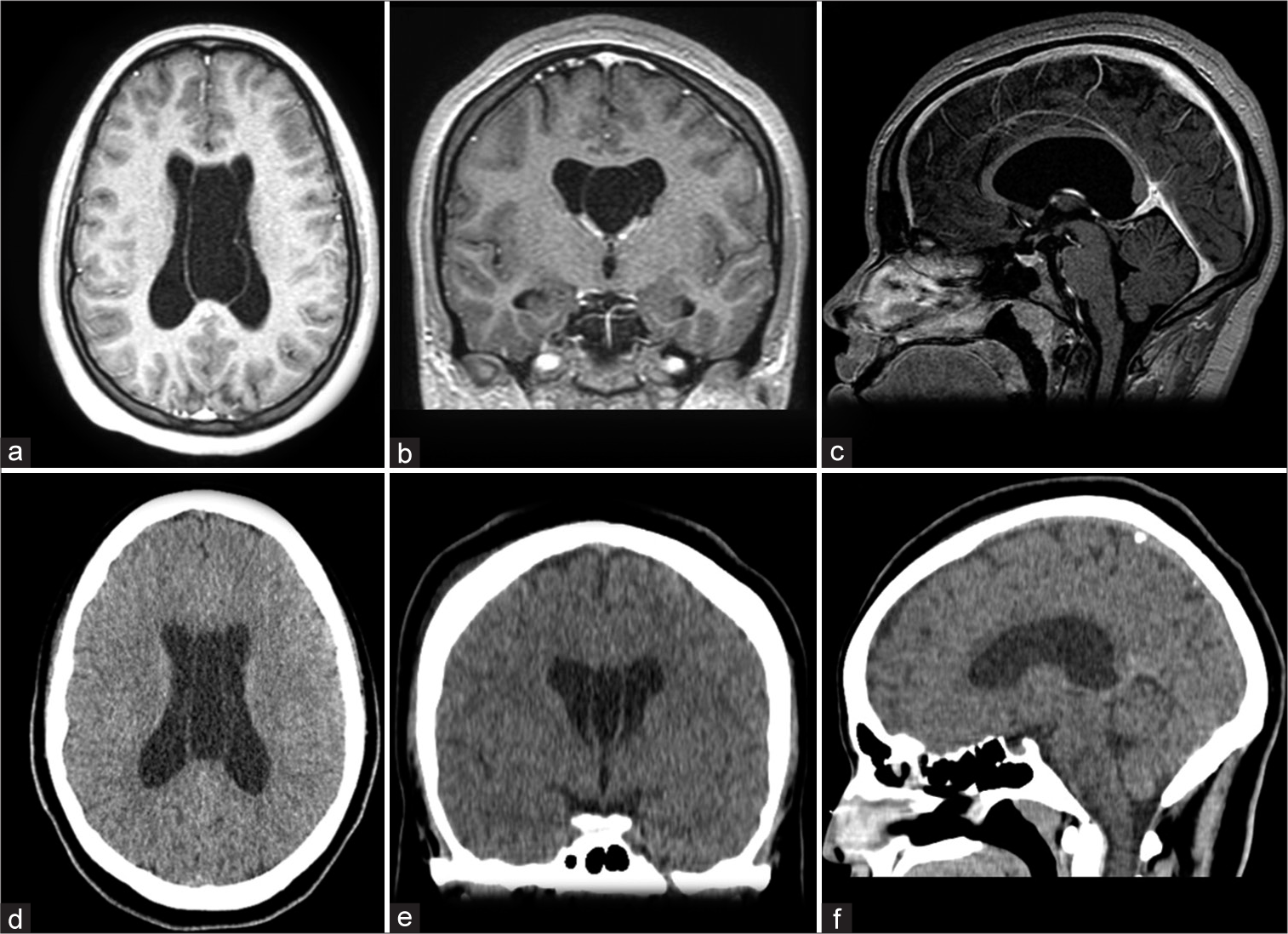
Figure 2:
Pre- and post-surgical cavum septum pellucidum (CSP) and cavum vergae (CV). (a and b) show the CSP and CV on presurgical magnetic resonance imaging. (b) shows the septate cyst. (c) it is not possible to see the cyst on presurgical sagittal plane. (d and e), from the postsurgical CT, demonstrate the cyst in smaller volume. (f) it is not possible to see the cyst on postsurgical sagittal plane.
On the 10th day after admission, a right transfrontal endoscopic intraventricular septostomy was successfully performed, communicating both lateral ventricles with the cyst, as well as a right endoscopic dilatation of the foramen of Monro (foraminoplasty) (EMF) to ensure communication between the lateral and third ventricles [
Video 1
During the following 3 days, the patient showed improvement in headaches, eyelid ptosis, and facial paralysis. On postsurgical CT scan, the cyst was smaller and there were no bleeding or other significant abnormalities [
At the 1-month follow-up appointment, she no longer had headaches, cranial nerves abnormalities, or any other neurological disorders. After 1 year, she remained asymptomatic and with normal fundoscopy.
DISCUSSION
The clinical evolution time for each patient with CSP and/or CV cyst is not specified in many articles; however, most of the cases progress from 1 month to 3 years.[
The patient and her family also had no prior knowledge about the cyst.
CSP and CV cysts are usually considered an incidental finding, although some of them may be pathological. It can be justified by some mechanisms, such as obstruction of the interventricular foramen, resulting in hydrocephalus and/or increased intracranial pressure; compression of the hypothalamic-septal triangle, leading to neuropsychiatric symptoms and/or compression of the optic chiasm and its pathways; and chronic deep venous involvement which can cause progressive focal deficits.[
In a meta-analysis performed with 368 patients, the following signs and symptoms were analyzed: headache (n = 184; 50%) and convulsive syndrome (n = 87; 23.6%); reduced intelligence/delayed psychomotor development (n = 74; 20.1%); mental disorders (n = 58;15.8%); dizziness, nausea, and vomiting (n = 40; 10.9%); impaired consciousness (n = 36; 9.8%); gait disorders (n = 33; 9%); visual impairment (n = 31; 8.4%); optic nerve swelling (n = 17; 4.6%); cranial nerve dysfunction (n = 15; 4%); and hydrocephalus (n = 61; 16.6%).[
According to Reid et al. and Sahin et al., in addition to papilledema, the sixth nerve palsy is the most common neurological disorder associated with intracranial hypertension (IH). This occurs when the brainstem moves downward, stretching the VI pair as it crosses over the petrous ridge and enters Dorello’s canal.[
The surgical approach is indicated when there is obstruction of the CSF flow in the foramen of Monro, direct compression of surrounding tissues, changes in mental status, or focal neurological deficits.[
Endoscopic fenestration involves a burr hole craniotomy, commonly performed in the right frontal region, to communicate the cyst with the lateral ventricles. It can also be executed by parietal cystostomy or direct transcavum interforniceal endoscopic fenestration. There was no statistically significant difference between these techniques, but they provide a reduction of the cyst size, with a less invasive approach, less recurrence, and better clinical outcome.[
Regarding EMF, Elkheshin and Zohdi reported three different types: dilatation (for congenital, idiopathic, or posthemorrhagic/meningitis stenosis), restoration (treating cyst wall obstruction or a membrane partially covering a nonstenotic foramen), and excision (for lesions of solid or mixed cystic components). In their study, 55 patients, who were submitted to EMF, had collapsible cyst walls.[
Our patient showed partial improvement of signs and symptoms days after endoscopic surgery and complete improvement 1 month after medical discharge, remaining asymptomatic since then.
CONCLUSION
This study provided a rare case of symptomatic enlargement of CSP and CV with IH and multiple nerves involvement. Cranial MRI was essential for the diagnosis. Neuroendoscopic fenestration and foraminoplasty provided complete resolution of the clinical features.
Declaration of patient consent
Patient’s consent not required as patient’s identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Video available on:
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Journal or its management. The information contained in this article should not be considered to be medical advice; patients should consult their own physicians for advice as to their specific medical needs.
References
1. Brazis PW. Isolated palsies of cranial nerves III, IV, and VI. Semin Neurol. 2009. 29: 14-28
2. Chen JJ, Chen CJ, Chang HF, Chen DL, Hsu YC, Chang TP. Prevalence of cavum septum pellucidum and/or cavum vergae in brain computed tomographies of Taiwanese. Acta Neurol Taiwan. 2014. 23: 49-54
3. Das JM, Dossani RH, editors. Cavum septum pellucidum. StatPearls. Treasure Island, FL: StatPearls Publishing; 2022. p. Available from: https://www.pubmed.ncbi.nlm.nih.gov/30725733 [Last accessed on 2022 Apr 13]
4. Elkheshin S, Zohdi A. Endoscopic monro foraminoplasty, types, techniques and complications avoidance. Interdiscip Neurosurg. 2022. 29: 101579
5. Fernández-Monteagudo B, Miranda-Herrero MC, ChacónPascual A, Vázquez-López M. VI and VII cranial nerve injury secondary to intracranial idiopathic hypertension in a pediatric patient. Rev Neurol. 2021. 72: 443
6. Kryukov EV, Stanishevsky AV, Gavrilov GV, Gizatullin SK. Cysts of septum pellucidum, cavum vergae and cavum veli interpositi. Meta-analysis of 368 cases. Zh Vopr Neirokhir Im N N Burdenko. 2020. 84: 111-8
7. Martins LP, Leitão AM, de Lucena JD, Gondim FA. Cavum septum pellucidum, da embriologia à clínica: Uma revisão da literatura. J Health Biol Sci. 2018. 7: 89-96
8. Oktem H, Dilli A, Kurkcuoglu A, Pelin C. Prevalence of septum pellucidum variations: A retrospective study. Open Access Libr J. 2018. 5: e5017
9. Pillai B, Farooque U, Sapkota M, Hassan SA, Mechtler LL. Symptomatic cavum septum pellucidum cyst: A rare presentation. Cureus. 2020. 12: e10395
10. Reid JE, Reem RE, Aylward SC, Rogers DL. Sixth nerve palsy in paediatric intracranial hypertension. Neuroophthalmology. 2016. 40: 23-7
11. Sahin T, Aksun ZO, Isikay CT, Sener O. Episodic oculomotor nerve palsy with intracranial hypertension and carcinomatous meningitis. Neuroophthalmology. 2020. 44: 399-402
12. Simonin A, Lind CR. Surgical management of symptomatic cavum septum pellucidum cysts: Systematic review of the literature. Neurosurg Rev. 2021. 44: 2425-32
13. Udayakumaran S, Onyia CU, Cherkil S. An analysis of outcome of endoscopic fenestration of cavum septum pellucidum cyst-more grey than black and white?. Pediatr Neurosurg. 2017. 52: 225-33
14. Wang KC, Fuh JL, Lirng JF, Huang WC, Wang SJ. Headache profiles in patients with a dilatated cyst of the cavum septi pellucidi. Cephalalgia. 2004. 24: 867-74


ahmedyahia
Posted December 7, 2022, 8:53 pm
Some patients have only headache without signs of IC hypertension. Endoscopic fenestration of both membran of cavum give good results