

- Department of Radiology, Dr. Soetomo General and Academic Hospital, Surabaya, East Java, Indonesia
- Department of Radiology, College of Medicine, University of Illinois at Chicago, Chicago, Illinois, United States
- Department of Ophthalmology, Dr. Soetomo General and Academic Hospital, Surabaya, East Java, Indonesia
Correspondence Address:
Widiana Ferriastuti, Department of Radiology, Dr. Soetomo General and Academic Hospital, Surabaya, East Java, Indonesia.
DOI:10.25259/SNI_110_2024
Copyright: © 2024 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Widiana Ferriastuti1, Suresh Kumar Mukherji2, Syahriar Muhammad1, Rozalina Loebis3. Craniosynostosis incidence with abnormalities of orbital axis on patients under 8 years old. 20-Dec-2024;15:466
How to cite this URL: Widiana Ferriastuti1, Suresh Kumar Mukherji2, Syahriar Muhammad1, Rozalina Loebis3. Craniosynostosis incidence with abnormalities of orbital axis on patients under 8 years old. 20-Dec-2024;15:466. Available from: https://surgicalneurologyint.com/?post_type=surgicalint_articles&p=13299
Date of Submission
15-Feb-2024
Date of Acceptance
30-Oct-2024
Date of Web Publication
20-Dec-2024
Abstract
Background: Craniosynostosis may result in malformations of the orbit, which can be observed in clinical presentations. Craniosynostosis impairs the normal growth of the skull, which typically occurs perpendicular to the fused suture. Craniosynostosis is classified into non-syndromic and syndromic, with an incidence of 1: 2000–2500 live births. It is commonly affects the sagittal suture (40–60%), followed by the coronal suture (20–30%), the metopic suture (
Methods: The research sample was craniosynostosis patients who were examined at the Radiology Department of Dr. Soetomo General Hospital at Surabaya, Indonesia for the period January 2017–March 2022, male or female aged
Results: A significant correlation was found between the incidence of craniosynostosis and abnormalities of OX (P-value: 0.000; OR: 22.81; R: 0.635).
Conclusion: There is a significant correlation between the incidence of craniosynostosis that has two or more sutural fusions and abnormalities of OX. Strabismus associated with craniosynostosis is typically detected in patients at an older age. Hopefully, by analyzing the eye angle through CT scans while craniosynostosis is established, abnormalities of the orbital axis can be identified. So the progression of strabismus can be prevented.
Keywords: Computed tomography scan, Craniosynostosis, Cyclorotated, Orbital anomalies, Strabismus
INTRODUCTION
Craniosynostosis is a premature and pathological fusion, either partial or complete, of one or more cranial sutures. This leads to impaired growth of the skull perpendicular to the affected suture. This condition is usually present at birth and can be associated with other anomalies.[
Craniosynostosis is classified into non-syndromic and syndromic with an incidence of 1: 2000–2,500 live births, most commonly in the sagittal suture 40–60%, coronal suture 20–30%, metopic suture <10%, and rarely in the lambdoid suture. The incidence of craniosynostosis syndrome, such as Apert and Crouzon syndrome, is 15.5/million and 16.5/ million live births, respectively.[
Radiological imaging has an important role in accurate diagnosis, surgical planning, post-treatment evaluation, and identification of coexisting anomalies and complications associated with craniosynostosis.[
Based on this background, researchers were interested in analyzing the correlation of orbital axis (OX) degrees to craniosynostosis, which has been carried out by computed tomography (CT)-Scan Head at Dr. Soetomo General Hospital, Surabaya. Through this research, we hope to detect early changes in OX, allowing for earlier intervention and better management, either surgical or non-surgical.
MATERIALS AND METHODS
The research was conducted after obtaining ethical clearance at Dr. Soetomo General Hospital, Surabaya, Indonesia from January 2017 to December 2022 (ethical number 1281/1184/ III/2022). The study was carried out with an observational retrospective approach with a case–control method. The case group consisted of patients with craniosynostosis, while the control group included patients without craniosynostosis, encompassing those with conditions such as meningoencephalitis at the radiology installation of Dr. Soetomo General Hospital for the period January 2017– March 2022. The data sources come from CT-Scan: Toshiba 128 slice type T5× – 101 A, Philips 128 slice type MRC 880, and Siemens 16 slice type M-CT-172 with data in the form of digital raw data. Raw data was measured using software on GE’s Picture Archiving and Communication System and Radiant DICOM viewer 2021.2.2. The method used is a manual tracer for each parameter to be measured. The inclusion criteria of this study were male or female craniosynostosis patients aged <8 years and who had never had head surgery. After obtaining the data, the case group and the control group (31:31) were matched, and a Chi-square correlation test was performed using the Statistical Package for the Social Sciences.
It is widely recognized that performing CT scans on children requires a different approach compared to adults. The size of a low-dose CT in children is typically set at around one-half or one-quarter of the dose of a standard head CT scan. The low-dose measurement was conducted according to the study sample, which consisted of patients under the age of 8. Pediatric CT images in this research were acquired at 100 kVp (CTDIvol 2.3 mGy; DLP 84.8 mGy*cm; scan time 6.1 s; helical pitch 0.297). This scanning method aligns with the research conducted by Nagayama et al. (2018).[
Evaluation of the position and axis of the extraocular muscles within the orbit is drawn on the coronal section, with the vertical line intersecting the nasal septum and the horizontal line intersecting the medial and lateral rectus muscles. The angles formed by these axes are then measured in degrees (°), with superior (-) indicating incyclorotation and inferior (+) indicating excyclorotation [
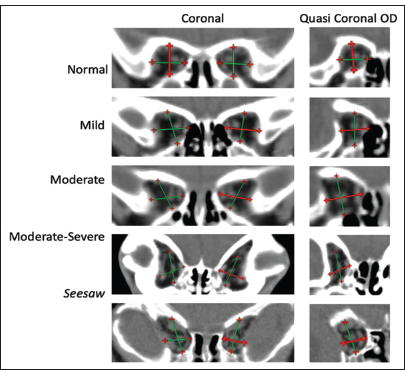
Figure 1:
Coronal and quasi coronal computed tomography scan of the posterior orbit of the right occuli. In normal, mild, and moderate criteria, the orbital wall encases the location of m. rectus at its orientation location, in moderate-severe criteria, medial bowing of the greater sphenoid wing (red & green cross arrow) causing m. rectus lateral becomes more inferior, in seesaw (Harlequin deformity), there is a temporal expansion of the orbital roof, indicating a V-pattern, causing lateral displacement of m. rectus superior.[
RESULTS
The data stated that of 31 patients with craniosynostosis, 22 (88.0%) of them experienced an abnormal axis condition. Of the 31 control groups, the majority had a normal OX degree, and only 3 (12.0%) had an abnormal axis condition [
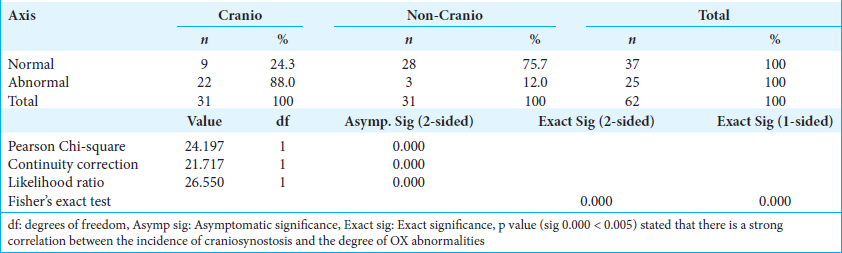
The Chi-square test was performed to determine the correlation between the incidence of craniosynostosis and the degree of OX abnormalities. The test results stated that P value (Sig 0.000 < 0.005) could mean that there was a significant relationship between the incidence of craniosynostosis and the degree of OX abnormalities [
We made several groups based on the degree of ocular tension as follows [
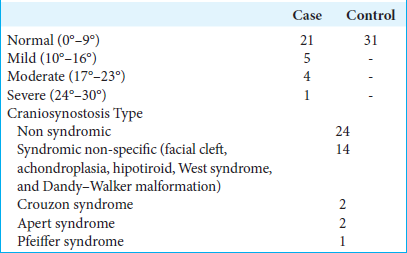
In the case group, if there are at least 2 or more sutures that fused, causing a different degree of OX. For instance, in the normal to mild group, suture closure was present in only one location. In the moderate group, suture closure occurred in two locations. In the severe group, there were more than two complex suture closures [
Based on the risk estimate test, the value 22.81 means that the sample with craniosynostosis has a 22.81 times risk of experiencing OX abnormalities compared to control samples without craniosynostosis [
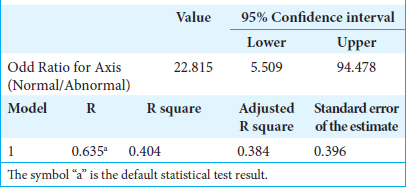
The results of the model summary are 0.635 or 63.5%. This value can be stated that the incidence of craniosynostosis affects up to 63.5% of abnormalities in the degree of OX. It can be estimated that out of 100 people with craniosynostosis, 63 of them will experience abnormal OX abnormalities [
DISCUSSION
Craniosynostosis frequency distribution
Craniosynostosis can lead to papilledema and, ultimately, optic atrophy and vision loss due to elevated intracranial pressure.[
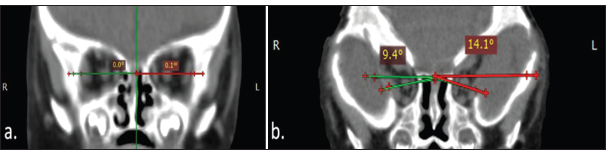
Figure 2:
(a) Normal axis in a 7-month-old boy and (b) exyclorotated in a 7-month-old boy with clover leaf skull shape in Crouzon syndrome. The angle formed respresents the intersection of the line between the lateral rectus muscle to the nasal septum and medial rectus muscle to the nasal septum. The green and red lines reveal the position and axis of the extraocular muscle; while the green line represents the right eye and the red line represents the left eye.
In the functional ophthalmic domain, strabismus was the most prevalent ocular anomaly in both non-syndromic 24% and syndromic craniosynostosis 58%. Strabismus can cause an increased risk of exocyclorotated orbits, which can lead to an incorrect insertion or even malformation of the extra-ocular muscles.[
Correlation between craniosynostosis and axis orbita
In measuring ocular torsion, we have to distinguish between subjective torsion and anatomic torsion because these measures can be very different. The one-third disc diameter of the normal torsional range actually subtends about 9° at the fovea. Thus, the torsional positions may differ by 9° from those of another and still be labeled within the normal range.[
Orbital deformity frequently accompanies the calvarial deformities of craniosynostosis. Elongation and rotation of the vertical axis of the orbital rim are present ipsilateral to coronal synostosis.[
The OX is the bisection of the line between medial and lateral orbital walls, while the visual axis is the position of the eye in primary gaze. Both the axis diverges at an angle of 23°. Normally, the equator of the globe is at or slightly anterior to the lateral orbital rim, and the spatial relationship between them is assessed by measuring the distance the globe (top of the cornea) extends over the infraorbital rim, and this distance is generally about 8 mm.[
Abnormal ocular torsion obviously occurs with palsy or paresis of a cyclovertical muscle. Extorsion occurs with paresis of a superior cyclovertical muscle and intorsion with paresis of an inferior cyclovertical muscle. Because the oblique muscles have greater torsional action than vertical action in the primary position, larger amounts of abnormal torsion are seen with oblique muscle pareses than with rectus muscle pareses. Likewise, oblique muscle surgery, whether a weakening or strengthening procedure, usually has a significant torsional effect.[
UCS has effects on ocular motility through the changes in shape and axis of the orbit on the synostotic side. The bony deformation in the frontozygomatic region can result in traction on the ocular globe.[
In this study, we found some anomaly as brachycephaly, cloverleaf skull, posterior plagiocephaly, scaphocephaly, and other similar cranial deformities. Implementation of the following CT scans in the control group was observed in patients with conditions other than craniosynostosis. These conditions included meningoencephalitis. Using some control group of patients, the patients are inevitably young, and therefore, it is difficult to diagnose and objectify ophthalmic sequelae, possibly leading to an underestimation of the prevalence of the described complications preoperatively.
Therefore, it remains important to keep young patients with UCS under precise orthoptic and ophthalmologic examinations, independent of the severity of UCS . Small manifest squints have the same inherent effect of visual loss through amblyopia as larger squints. Clinicians need to be aware that this can occur on the non-synostotic side as well as the synostotic side. The patient should be kept under close regular monitoring both pre-and postoperatively.[
Axial CT scanning augmented with coronal and longitudinal orbital reformatted images has been useful for quantitative spatial localization of the globes. Nonetheless, the slice format of these images requires imagination for surgical planning.[
CONCLUSION
The diagnosis of craniosynostosis is based on clinical features and investigations. Radiological examination is important for making an accurate diagnosis, surgery planning, evaluating therapy, and identifying accompanying anomalies and complications related to craniosynostosis surgery. This study found that there is a significant correlation between craniosynostosis and abnormalities of OX. Strabismus associated with craniosynostosis is typically detected in patients at an older age. By analyzing the OX through CT scans during the diagnosis of craniosynostosis, earlier diagnosis and treatment can be achieved, potentially preventing the progression of strabismus.
Ethical approval
The research/study approved by the Institutional Review Board at Dr. Soetomo General and Academic Hospital, number 1281/1184/III/2022, dated 2022.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Journal or its management. The information contained in this article should not be considered to be medical advice; patients should consult their own physicians for advice as to their specific medical needs.
References
1. Bagley CA, Khavkin Y, Witham TF, Wolinsky J, Gokaslan ZL. A biweekly publication for clinical neurosurgical surgical management of malignant spinal tumors: Part II. Contemp Neurosurg. 2007. 29: 1-8
2. Chawla S, Wang S, Mohan S, Nasrallah M, Verma G, Brem S. Differentiation of brain infection from necrotic glioblastoma using combined analysis of diffusion and perfusion MRI. J Magn Reson Imaging. 2019. 49: 184-94
3. Chung SA, Yun IS, Moon JW, Lee JB. Ophthalmic findings in children with nonsyndromic craniosynostosis treated by expansion cranioplasty. J Craniofac Surg. 2015. 26: 79-83
4. Dagi L, MacKinnon S, Zurakowski D, Prabhu SP. Rectus muscle excyclorotation and V-pattern strabismus: A quantitative appraisal of clinical relevance in syndromic craniosynostosis. Br J Ophthalmol. 2017. 101: 1560-5
5. Dalmas F, Pech-Gourg G, Gallucci A, Denis D, Scavarda D. Craniosynostosis and oculomotor disorders. Neurochirurgie. 2020. 66: 91-6
6. Denis D, Genitori L, Conrath J, Lena G, Choux M. Ocular findings in children operated on for plagiocephaly and trigonocephaly. Childs Nerv Syst. 1996. 12: 683-9
7. Duan M, Skoch J, Pan BS, Shah V. Neuro-ophthalmological manifestations of craniosynostosis: Current perspectives. Eye Brain. 2021. 13: 29-40
8. Gencarelli JR, Murphy A, Samargandi OA, Bezuhly M. Ophthalmologic outcomes following fronto-orbital advancement for unicoronal craniosynostosis. J Craniofac Surg. 2016. 27: 1629-35
9. Gupta S, Ghose S, Rohatgi M, Kumar A, Das A. The optic nerve in children with craniosynostosis. A pre and post surgical evaluation. Doc Opthalmol. 1993. 83: 271-8
10. Guyton DL. Clinical assessment of ocular torsion. Am Orthop J. 1983. 33: 7-15
11. Jaichandran VV. Ophthalmic regional anaesthesia: A review and update. Indian J Anaesth. 2013. 57: 7-13
12. Kalantar-Hormozi H, Abbaszadeh-Kasbi A, Sharifi G, Davai NR, Kalantar-Hormozi A. Incidence of familial craniosynostosis among patients with nonsyndromic craniosynostosis. J Craniofac Surg. 2019. 30: e514-7
13. Kim HJ, Roh HG, Lee IW. Craniosynostosis: Updates in radiologic diagnosis. J Korean Neurosurg Soc. 2016. 59: 219-26
14. Kronig SA, Kronig OD, Zurek M, Van Adrichem LN. Orbital volume, ophthalmic sequelae and severity in unilateral coronal synostosis. Childs Nerv Syst. 2021. 37: 1687-94
15. Luo WT, Chen X, Zhang YD, Liu QY, Qiao T. Ophthalmological outcomes of unilateral coronal synostosis in young children. BMC Ophthalmol. 2020. 20: 318
16. Marsh JL, Vannier MW. The anatomy of the cranio-orbital deformities of craniosynostosis: Insights from 3-D images of CT scans. Clin Plast Surg. 1987. 14: 49-60
17. Massimi L, Di Rocco C. Unilateral coornal craniosynostosis. Pediatr Neurosurg. 2017. p. 1-45
18. Nagayama Y, Oda S, Nakaura T, Tsuji A, Urata J, Furusawa M. Radiation dose reduction at pediatric CT: Use of low tube voltage and iterative reconstruction. Radiographics. 2018. 38: 1421-40
19. Rostamzad P, Arslan ZF, Mathijssen IM, Koudstaal MJ, Pleumeekers MM, Versnel SL. Prevalence of ocular anomalies in craniosynostosis: A systematic review and meta-analysis. J Clin Med. 2022. 11: 1060
20. Tuite GF, Chong WK, Evanson J, Narita A, Taylor D, Harkness W. The effectiveness of papilledema as an indicator of raised intracranial pressure in children with craniosynostosis. Neurosurgery. 1996. 38: 272-8


