

- Department of Neurology, The University of Chicago Medicine, Chicago, United States
- Department of Neurosurgery, Brown University, Warren Alpert School of Medicine, Providence, United States
- Department of Neuroradiology and Neuroendovascular Surgery, The University of Chicago Medicine, Chicago, United States
Correspondence Address:
Archit Bharathwaj Baskaran, Department of Neurology, The University of Chicago Medicine, Chicago, United States.
DOI:10.25259/SNI_1093_2024
Copyright: © 2025 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Archit Bharathwaj Baskaran1, Aditya Jhaveri1, Olivia A. Kozel2, Chibueze Ikechukwu Agwu1, Sachin Kothari1, Therese Dunne1, Michael Charles Hurley3, James E. Siegler1. A type II proatlantal artery arising from the external carotid artery: A review of neurovascular anatomy. 23-May-2025;16:198
How to cite this URL: Archit Bharathwaj Baskaran1, Aditya Jhaveri1, Olivia A. Kozel2, Chibueze Ikechukwu Agwu1, Sachin Kothari1, Therese Dunne1, Michael Charles Hurley3, James E. Siegler1. A type II proatlantal artery arising from the external carotid artery: A review of neurovascular anatomy. 23-May-2025;16:198. Available from: https://surgicalneurologyint.com/?post_type=surgicalint_articles&p=13571
Date of Submission
18-Dec-2024
Date of Acceptance
08-Apr-2025
Date of Web Publication
23-May-2025
Abstract
Background: A type II proatlantal artery is a rare congenital vascular anomaly comprised of a persistent embryologic connection between the carotid and vertebrobasilar circulations. Although generally asymptomatic and detected incidentally, its identification is of clinical importance in neurovascular assessments and interventions.
Case Description: A 70-year-old male presented with acute-onset left lower extremity weakness and numbness, out of the window for thrombolytics; computed tomography angiography of the head and neck incidentally identifying a persistent left type II proatlantal artery originating from the external carotid artery and supplying the vertebrobasilar circulation. Magnetic resonance imaging of the brain the following day was unremarkable for acute infarction or other cerebrovascular pathology.
Conclusion: This case underscores the significance of recognizing congenital vascular anomalies such as the type II proatlantal artery, particularly in the context of cerebrovascular assessment. Although these variants are often incidental and not associated with increased stroke risk, their presence has implications for neuroendovascular procedures and stroke evaluations. Understanding the anatomic and embryologic origins of these vascular anomalies facilitates accurate interpretation of cerebrovascular imaging and enhances clinical decision-making in patients with these anomalies.
Keywords: Endovascular surgical neuroradiology, Neuroanatomy, Neurovascular, Proatlantal artery, Stroke
INTRODUCTION
A type II proatlantal artery is a rare congenital vascular anomaly comprised of a persistent embryologic connection between the carotid and vertebrobasilar circulations. Although generally asymptomatic and detected incidentally, its’ identification is of clinical importance in neurovascular assessments and interventions. The following case reports describes a patient with one such rare anomaly as well as the potential implications for clinical decision making.
CASE PRESENTATION
A 70-year-old man with hypertension, diabetes, and active smoking presented with left leg weakness and numbness below the knee. On arrival, he was hypertensive and hyperglycemic, with a National Institutes of Health Stroke Scale of 4 for left leg weakness and sensory loss. He was not administered thrombolytics due to presenting out of the window. Computed tomography (CT) head non-contrast showed no hemorrhage. CT angiogram (CTA) head and neck with contrast showed no large vessel occlusion. CT perfusion (CTP) of the brain showed no perfusion mismatch deficit. CTA did, however, reveal an anatomic variant of his cervical external carotid artery – by which a left persistent type II proatlantal artery arose from the external carotid artery – which is detailed further in the next section. He was loaded with dual antiplatelet therapy consisting of aspirin 81 mg and clopidogrel 75 mg, then admitted. The following morning, his magnetic resonance imaging brain was unremarkable for acute stroke or other acute neurologic abnormality. He was found to be in opioid withdrawal with a urinary tract infection and thereafter transferred to the internal medicine service for further workup and management.
DISCUSSION OF IMAGING FINDINGS
As noted above, CTA head and neck with and without contrast demonstrated a left persistent type II proatlantal artery originating from the external carotid artery see
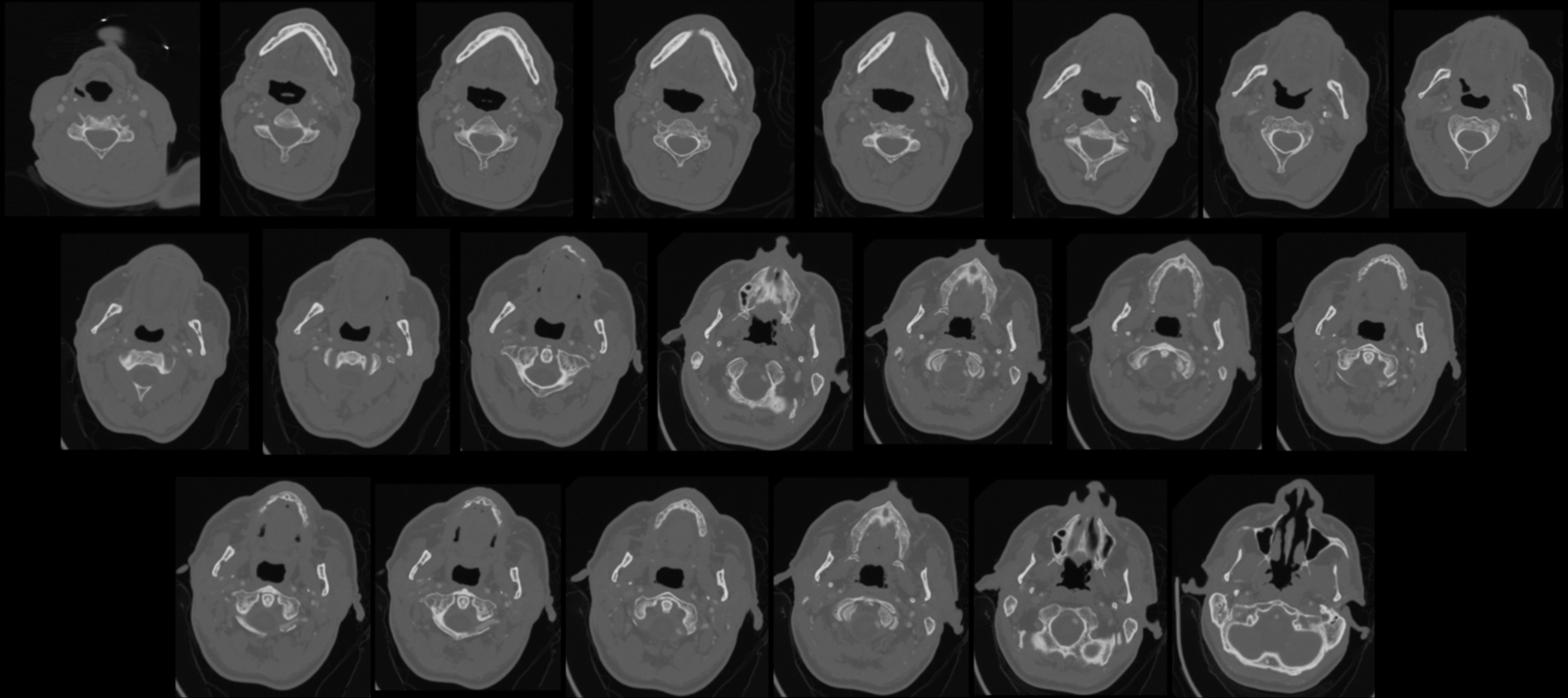
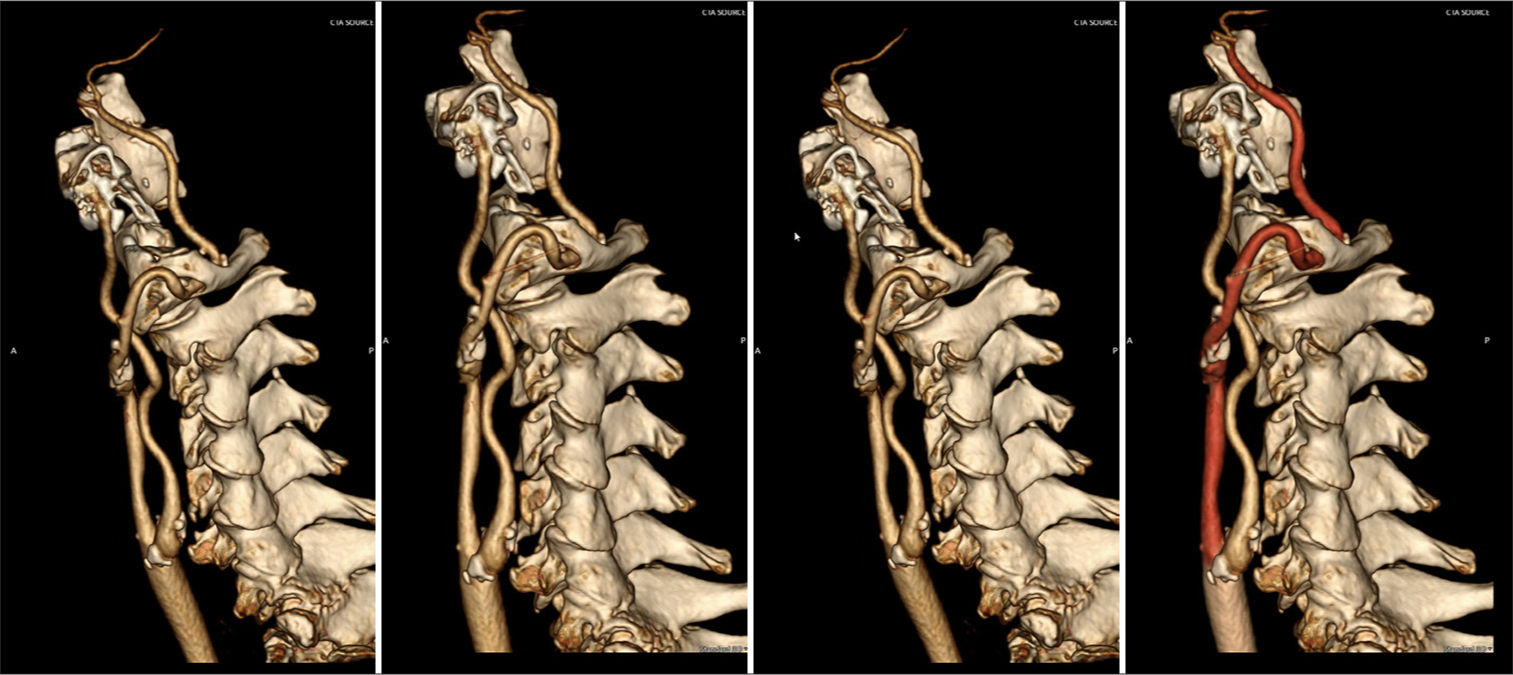
The proatlantal artery is a variant of the vertebral artery, in which the ipsilateral or bilateral vertebral arteries themselves are aplastic or hypoplastic, while the proatlantal artery arises from the internal or external carotid artery, coursing through the foramen magnum to create the main blood supply for the posterior circulation.[
REVIEW OF EMBRYOLOGY/DEVELOPMENT
Variants of the cervical vertebral arterial tree are common and may be found in approximately 1 in six patients, most commonly related to the anomalous origin of the left vertebral artery of the aortic arch, hypoplastic vertebral arteries, fenestration (which can be misinterpreted as intraluminal thrombus), duplication at the origin,[
CLINICAL IMPLICATIONS
Detection of type II proatlantal arteries is most found incidentally.[
Take home bullet points
A type II proatlantal artery refers to the persistent embryological variant of an external carotid to the vertebral arterial anastomosis. It is formed congenitally via embryological failure of involution in the developing vertebral artery system, leading to the persistence of intersegmental arteries. Cases of proatlantal artery variants have not been proven to increase susceptibility to cerebrovascular complications. Some cases have been reported with pulsatile tinnitus as a presenting feature. It holds significance anatomically for neuroendovascular procedures and stroke workups.
CONCLUSION
In this review, we discussed a case of a man with a proatlantal artery type II, an embryological derivative of expected vasculature whereby an intersegmental artery creates an anastomosis between the external carotid artery and the vertebral artery. As in this case, many are found incidentally. When found, it remains important to note that they may hold significance clinically for neuroendovascular interventions and stroke workups.
Ethical approval:
The Institutional Review Board approval is not required.
Declaration of patient consent:
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship:
Nil.
Conflicts of interest:
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation:
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Journal or its management. The information contained in this article should not be considered to be medical advice; patients should consult their own physicians for advice as to their specific medical needs.
Acknowledgments:
We would like to extend our gratitude to Dr. Michael Hurley for his time and effort in generating 3D images for this manuscript.
References
1. Babici D, Johansen PM, Sial N, Snelling B. Intracranial angioplasty via type II proatlantal intersegmental artery. Cureus. 2023. 15: e47724
2. Bahşi YZ, Uysal H, Peker S, Yurdakul M. Persistent primitive proatlantal intersegmental artery (proatlantal artery I) results in ‘top of the basilar’ syndrome. Stroke. 1993. 24: 2114-7
3. Bueno HF, Nimchinsky EA. Mapping of anatomic variants of the proximal vertebral artery in relation to embryology. AJNR Am J Neuroradiol. 2023. 44: 943-50
4. Chen CJ, Wang LJ, Wong YC. Abnormal origin of the vertebral artery from the common carotid artery. AJNR Am J Neuroradiol. 1998. 19: 1414-6
5. Choudhary G, Adhikari N, Chokr J, Gupta N. Type 2 persistent primitive proatlantal intersegmental artery, a rare variant of persistent carotid-vertebrobasilar anastomoses. Proc (Bayl Univ Med Cent). 2019. 32: 101-4
6. Kolbinger R, Heindel W, Pawlik G, Erasmi-Körber H. Right proatlantal artery type I, right internal carotid occlusion, and left internal carotid stenosis: Case report and review of the literature. J Neurol Sci. 1993. 117: 232-9
7. Peeters JB, Idriceanu T, El Hage G, Martin T, Salaud C, Champagne PO. A comprehensive review of the vertebral artery anatomy. Neurochirurgie. 2024. 70: 101518
8. Purkayastha S, Gupta AK, Varma R, Kapilamoorthy TR. Proatlantal intersegmental arteries of external carotid artery origin associated with Galen’s vein malformation. AJNR Am J Neuroradiol. 2005. 26: 2378-83
9. Tudose RC, Rusu MC, Hostiuc S. The vertebral artery: A systematic review and a meta-analysis of the current literature. Diagnostics (Basel). 2023. 13: 2036
10. Zarghouni M, Marichal D. Persistent bilateral proatlantal type II artery. Proc (Bayl Univ Med Cent). 2013. 26: 50-1

