

- Department of Neurosurgery, University Hospital Hassan II, Morocco.
- Clinical Neurosciences Laboratory, Faculty of Medicine and Pharmacy, University of Fez, Fez, Morocco.
Correspondence Address:
Mohammed Benzagmout
Department of Neurosurgery, University Hospital Hassan II, Morocco.
Clinical Neurosciences Laboratory, Faculty of Medicine and Pharmacy, University of Fez, Fez, Morocco.
DOI:10.25259/SNI_67_2019
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Meryem Himmiche, Khalid Chakour, Mohammed El Faiz Chaoui, Mohammed Benzagmout. Posterior epidural migration of a lumbar disc herniation. 03-Jan-2020;11:4
How to cite this URL: Meryem Himmiche, Khalid Chakour, Mohammed El Faiz Chaoui, Mohammed Benzagmout. Posterior epidural migration of a lumbar disc herniation. 03-Jan-2020;11:4. Available from: https://surgicalneurologyint.com/surgicalint-articles/9831/
Date of Submission
18-Feb-2019
Date of Acceptance
21-Oct-2019
Date of Web Publication
03-Jan-2020
Abstract
Background: Posterior epidural migration of a lumbar disc fragment (PEMLDF) refers to the dorsal migration of disc material around the thecal sac that can lead to radiculopathy and/or cause a cauda equina syndrome. It is rare and the diagnosis is often just established intraoperatively.
Case Description: A 50-year-old male with a chronic history of low back pain and psychosis presented with PEMLDF originating at the L4–L5 level.
Conclusion: Lumbar disc herniations rarely present as PEMLDF resulting in symptoms varying from radiculopathy to cauda equina syndrome. These should be included among the differential diagnostic considerations for dorsolateral epidural lesions.
Keywords: Disc herniation, Epidural migration, Lumbar, Posterior
INTRODUCTION
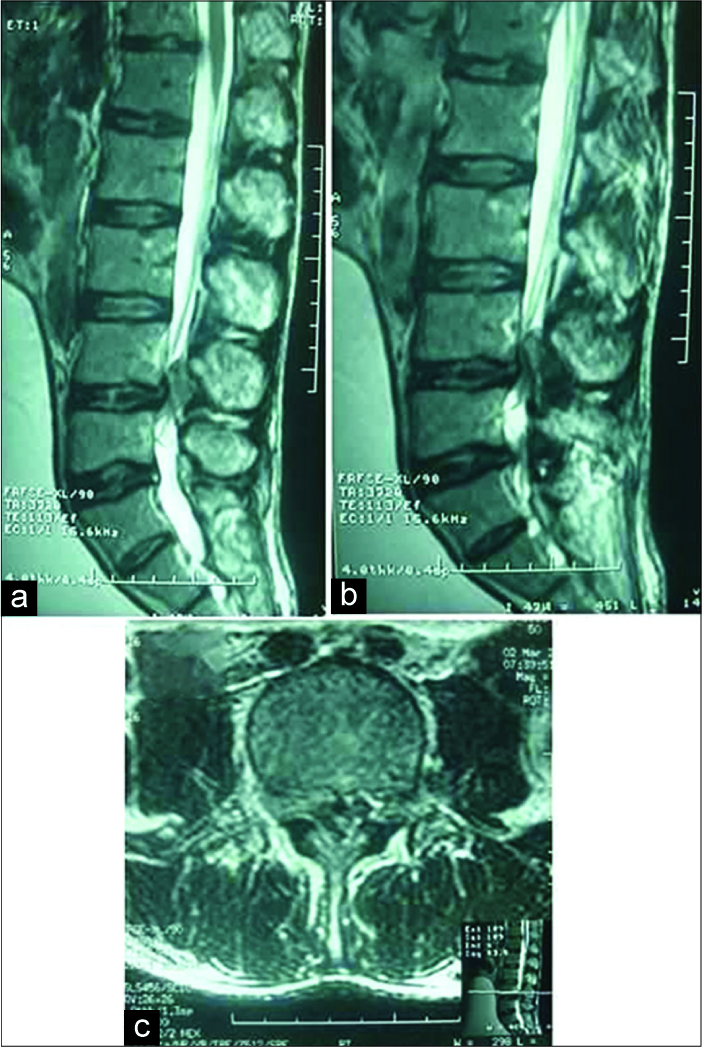
Posterior epidural migration of a lumbar disc fragment (PEMLDF) may migrate dorsolaterally around the thecal sac and contributes to symptoms and signs ranging from mild radiculopathy to flagrant cauda equina syndrome. Here, we present a 50-year-old male with a chronic history of low back pain and psychosis, who suddenly developed bilateral lower extremity paresthesias, and weakness; on examination, he was paraparetic with perineal numbness and urinary retention (i.e., Frankel Grade C), and the lumbar magnetic resonance imaging (MRI) showed severe canal stenosis at the L4–L5 level, a mild L4–L5 disc bulge, and a large hypointense dorsal-lateral epidural mass resulting in severe thecal sac/cauda equina compression [
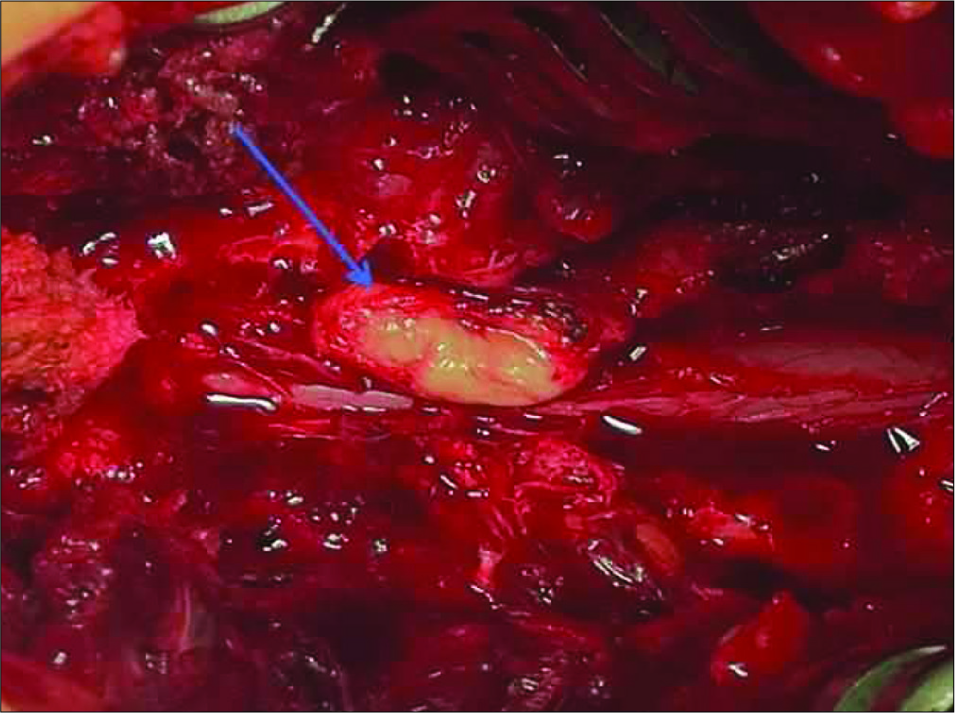
Surgery
As the patient exhibited an acute cauda equina syndrome, he underwent an emergent L4–L5 laminectomy. At surgery, a large posterior epidural disc fragment was identified; it had extruded/ sequestrated from the L4-L5 intervertebral disc, erupted through the posterior longitudinal ligament, and migrated posterolaterally, displacing the dura anterolaterally toward the left [
DISCUSSION
PEMLDF is rare and most commonly encountered in adults averaging 53 years of age; there is a clear male predominance.[
CONCLUSION
Lumbar disc herniations are rarely presenting as PEMLDF resulting in symptoms varying from radiculopathy to cauda equina syndrome. These should be included in the differential diagnosis considerations for lumbar spinal dorsolateral lesions.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Akhaddar A, El-Asri A, Boucetta M. Posterior epidural migration of a lumbar disc fragment: A series of 6 cases. J Neurosurg Spine. 2011. 15: 117-28
2. Derincek A, Ozalay M, Sen O, Pourbagher A. Posterior epidural mass: Can a posteriorly migrated lumbar disc fragment mimic tumour, haematoma or abscess?. Acta Orthop Belg. 2009. 75: 423-7
3. Lombardi V. Lumbar spinal block by posterior rotation of anulus fibrosus. Case report. J Neurosurg. 1973. 39: 642-7
4. Turan Y, Yilmaz T, Gocmez C, Ozevren H, Kemaloglu S, Teke M. Posterior epidural migration of a sequestered lumbar intervertebral disc fragment. Turk Neurosurg. 2017. 27: 85-94

