

- Department of Neurosurgery, Sapporo Teishinkai Hospital, Sapporo, Japan.
Correspondence Address:
Rokuya Tanikawa, Chief of Stroke Center, Department of Neurosurgery, Sapporo Teishinkai Hospital, Sapporo, Japan.
DOI:10.25259/SNI_995_2022
Copyright: © 2023 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Yosuke Suzuki, Kosumo Noda, Nakao Ota, Tomomasa Kondo, Kenichi Haraguchi, Norio Miyoshi, Katsunari Kiko, Kohei Yoshikawa, Shun Ono, Hiroyuki Mizuno, Yasuaki Okada, Takuma Takano, Soichiro Yasuda, Jumpei Oda, Hiroyasu Kamiyama, Sadahisa Tokuda, Rokuya Tanikawa. A case of facial nerve palsy caused by severe head injury treated by translabyrinthine approach. 10-Feb-2023;14:47
How to cite this URL: Yosuke Suzuki, Kosumo Noda, Nakao Ota, Tomomasa Kondo, Kenichi Haraguchi, Norio Miyoshi, Katsunari Kiko, Kohei Yoshikawa, Shun Ono, Hiroyuki Mizuno, Yasuaki Okada, Takuma Takano, Soichiro Yasuda, Jumpei Oda, Hiroyasu Kamiyama, Sadahisa Tokuda, Rokuya Tanikawa. A case of facial nerve palsy caused by severe head injury treated by translabyrinthine approach. 10-Feb-2023;14:47. Available from: https://surgicalneurologyint.com/surgicalint-articles/12151/
Date of Submission
30-Oct-2022
Date of Acceptance
10-Jan-2023
Date of Web Publication
10-Feb-2023
Abstract
Background: Several treatments for traumatic facial paralysis have been reported, but the role of surgery is still controversial.
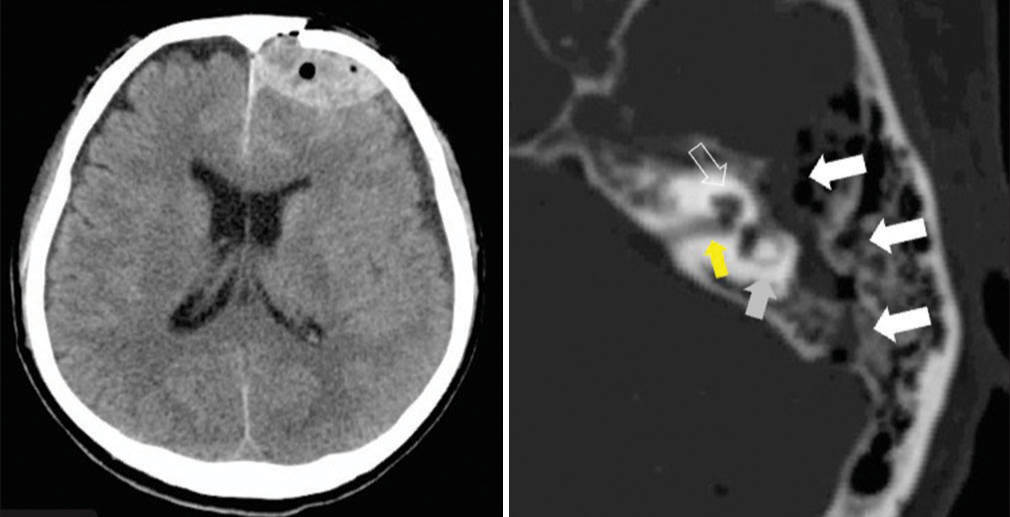
Case Description: A 57-year-old man was admitted to our hospital with head trauma due to a fall injury. A total body computed tomography (CT) scan showed a left frontal acute epidural hematoma associated with a left optic canal and petrous bone fractures with the disappearance of the light reflex. Hematoma removal and optic nerve decompression were performed immediately. The initial treatment was successful with complete recovery of consciousness and vision. The facial nerve paralysis (House and Brackmann scale grade 6) did not improve after medical therapy, and thus, surgical reconstruction was performed 3 months after the injury. The left hearing was lost entirely, and the facial nerve was surgically exposed from the internal auditory canal to the stylomastoid foramen through the translabyrinthine approach. The facial nerve’s fracture line and damaged portion were recognized intraoperatively near the geniculate ganglion. The facial nerve was reconstructed using a greater auricular nerve graft. Functional recovery was observed at the 6-months follow-up (House and Brackmann grade 4), with significant recovery in the orbicularis oris muscle.
Conclusion: Interventions tend to be delayed, but it is possible to select a treatment method of the translabyrinthine approach.
Keywords: Facial nerve reconstruction, Greater auricular nerve graft, Mastoidectomy, Severe head trauma, Translabyrinthine approach
INTRODUCTION
Several treatments for traumatic facial paralysis have been reported, but the role of surgery is still controversial.[
Here, the authors report a case of facial nerve paralysis due to infratemporal blunt trauma, which was treated by surgical decompression and reconstruction of the facial nerve using a greater auricular nerve graft through the translabyrinthine approach. We analyze and discuss intraoperative anatomy, surgical techniques, and postoperative outcome of the case.
CASE REPORT
A 57-year-old man fell from a height of 1.5 m during his work shift and was transported to our hospital’s emergency room. He had minor consciousness impairment at arrival (GCS; E4V4M6) but no remarkable facial palsy. A total body CT scan showed a thick left frontal acute epidural hematoma associated with skull fractures of the left frontal, petrous and occipital bone, the clivus, the lateral wall of the left orbit, and the maxilla. The petrous bone fracture was a mixed pattern [

Tear production was preserved, but the sense of taste at the anterior two-thirds of the tongue was reduced. The authors hypothesized that the facial nerve injury was between the geniculate ganglion and the origin of the chorda tympani and since the patient’s facial palsy is an immediate type, no improvement was observed by conservative treatment. Thus, we judged that reconstruction was indicated for the patient.
The translabyrinthine approach was utilized to expose the facial nerve from the internal auditory meatus to the stylomastoid foramen.
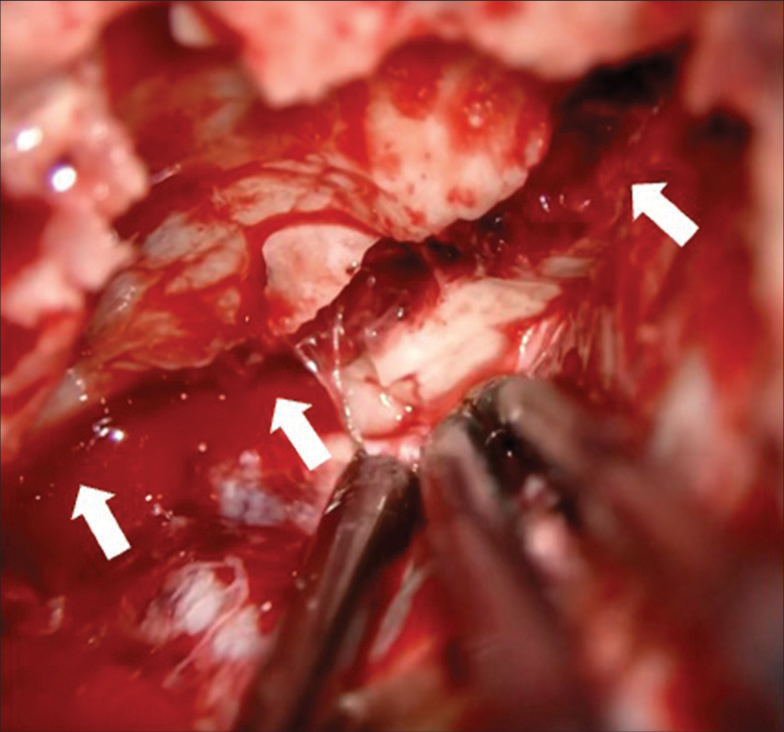
The facial nerve injury was intraoperatively confirmed along the fracture line near the distal side of the geniculate ganglion, and granulated tissues covered it. After dissecting the facial nerve, a greater auricular nerve graft was harvested, and the facial nerve was reconstructed using the greater auricular nerve as an interposition graft [
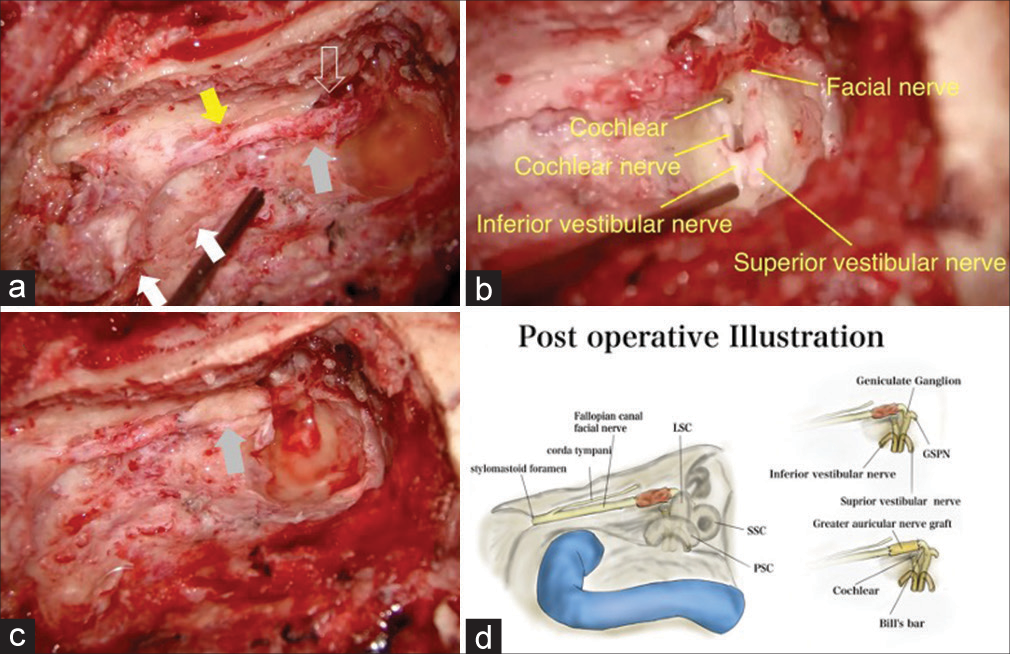
Figure 4:
Intraoperative image of the facial nerve decompressed in the mastoid (yellow arrow) and tympanic (open white arrow) segments; (left ear, mastoidectomy, and posterior tympanotomy were performed, luxated incus and head of the malleus were removed). White arrows point to the fracture line. The gray arrow indicates a granulated injured facial nerve in (a) and replaced by a greater auricular nerve in (c). Normal facial nerve was confirmed by translabyrinthine approach (b). (d) A schematic image of recontraction surgery.

DISCUSSION
Facial nerve paralysis associated with temporal bone fractures occurs in 7–10% of temporal bone fractures and is accountable for most traumatic facial nerve paralysis.[
There are many reports of facial nerve decompression to treat traumatic facial nerve paralysis. When the facial nerve is transected, direct cooptation is the best choice of treatment, and a nerve interposition autograft should be employed if the motor end-plates are still intact and direct end-to-end anastomosis is not feasible.[
Facial paralysis is classified as immediate paralysis if the onset is within 24 h after trauma and delayed paralysis is when the onset is after 24 h. Immediate paralysis is likely to occur when direct damage such as traction or compression by bone fragments occurs. Delayed paralysis is more likely to happen when the nerve is indirectly injured by hematoma, edema, or compressed by surrounding swollen tissues.[
Spontaneous recovery is unlikely to occur for immediate or severe paralysis, and Fisch reported that complete facial nerve palsy within 6 days of onset needs immediate decompression with other institutions adopting this surgical intervention strategy.[
However, most patients with temporal bone fractures due to severe head injury suffer from intracranial or systemic complications and present with impaired consciousness. Facial nerve function assessment is challenging for patients with impaired consciousness,[
On the other hand, facial nerve paralysis due to severe head injury is often accompanied by inner ear disorder, which allows a translabyrinthine approach that can offer wide facial nerve decompression. Wide facial nerve decompression exposes the damaged part of the nerve, allowing nerve reconstruction. Several techniques have been described for facial nerve reconstruction.[
CONCLUSION
Interventions tend to be delayed for facial paralysis associated with severe head trauma. On the other hand, it is possible to select a treatment method that exposes the facial nerve from the brain stem to the stylomastoid foramen using the translabyrinthine approach since inner ear injuries are likely to be present for these patients.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Journal or its management. The information contained in this article should not be considered to be medical advice; patients should consult their own physicians for advice as to their specific medical needs.
References
1. Alvi A, Bereliani A. Acute intracranial complications of temporal bone trauma. Otolaryngol Head Neck Surg. 1998. 119: 609-13
2. Brodsky L, Eviatar A, Daniller A. Post-traumatic facial nerve paralysis: Three cases of delayed temporal bone exploration with recovery. Laryngoscope. 1983. 93: 1560-5
3. Darrouzet V, Duclos JY, Liguoro D, Truilhe Y, De Bonfils C, Bebear JP. Management of facial paralysis resulting from temporal bone fractures: Our experience in 115 cases. Otolaryngol Head Neck Surg. 2001. 125: 77-84
4. Fisch U. Management of intratemporal facial nerve injuries. J Laryngol Otol. 1980. 94: 129-34
5. Hato N, Nota J, Hakuba N, Gyo K, Yanagihara N. Facial nerve decompression surgery in patients with temporal bone trauma: Analysis of 66 cases. J Trauma. 2011. 71: 1789-92 discussion 1792-3
6. Irugu DV, Singh A, Ch S, Panuganti A, Acharya A, Varma H. Comparison between early and delayed facial nerve decompression in traumatic facial nerve paralysis-A retrospective study. Codas. 2018. 30: e20170063
7. Kim J, Moon IS, Shim DB, Lee WS. The effect of surgical timing on functional outcomes of traumatic facial nerve paralysis. J Trauma. 2010. 68: 924-9
8. Kojiro T, Akihiro N, Masafumi H, Yu S, Yasuzo T, Haruo S. Treatment of traumatic facial paralysis. Practica Otologica Pract Otol (Kyoto) Practica Oto-Rhino-Laryngologica. 1999. 45: 459-63
9. Lee SY, Seong J, Kim YH. Clinical implication of facial nerve decompression in complete bell’s palsy: A systematic review and meta-analysis. Clin Exp Otorhinolaryngol. 2019. 12: 348-59
10. Li L, Fan Z, Wang H, Han Y. Efficacy of surgical repair for the functional restoration of injured facial nerve. BMC Surg. 2021. 21: 32
11. Nash JJ, Friedland DR, Boorsma KJ, Rhee JS. Management and outcomes of facial paralysis from intratemporal blunt trauma: A systematic review. Laryngoscope. 2010. 120: 1397-404
12. Nosan DK, Benecke JE, Murr AH. Current perspective on temporal bone trauma. Otolaryngol Head Neck Surg. 1997. 117: 67-71
13. Paul P, Sabrigirish K, Choudhury B, Upadhyay K, Raina S. Facial nerve decompression via posterior tympanotomy approach in traumatic facial nerve palsy. Indian J Neurotrauma. 2010. 7: 85-7
14. Quaranta A, Campobasso G, Piazza F, Quaranta N, Salonna I. Facial nerve paralysis in temporal bone fractures: Outcomes after late decompression surgery. Acta Otolaryngol. 2001. 121: 652-5
15. Ricciardi L, Stifano V, Pucci R, Stumpo V, Montano N, Monaca MD. Comparison between VII-to-VII and XIIto-VII coaptation techniques for early facial nerve reanimation after surgical intra-cranial injuries: A systematic review and pooled analysis of the functional outcomes. Neurosurg Rev. 2021. 44: 153-61
16. Rodríguez-Lorenzo A, Tzou CH, editors. Principles of facial nerve reconstruction. Facial Palsy: Techniques for Reanimation of the Paralyzed Face. Cham: Springer International Publishing; 2021. p. 55-69
17. Sanuş GZ, Tanriöver N, Tanriverdi T, Uzan M, Akar Z. Late decompression in patients with acute facial nerve paralysis after temporal bone fracture. Turk Neurosurg. 2007. 17: 7-12
18. Ulug T, Ulubil SA. Management of facial paralysis in temporal bone fractures: A prospective study analyzing 11 operated fractures. Am J Otolaryngol. 2005. 26: 230-8
19. Xu P, Jin A, Dai B, Li R, Li Y. Surgical timing for facial paralysis after temporal bone trauma. Am J Otolaryngol. 2017. 38: 269-71
20. Yeoh TL, Mahmud R, Saim L. Surgical intervention in traumatic facial nerve paralysis. Med J Malaysia. 2003. 58: 432-6

