

- Department of Neurosurgery, Kesennuma City Hospital, Kesennuma, Miyagi, Japan
- Department of Radiological Technology, Kesennuma City Hospital, Kesennuma, Miyagi, Japan
- Department of Neurosurgery, Tohoku University Graduate School of Medicine, Sendai, Miyagi, Japan.
Correspondence Address:
Norio Narita
Department of Neurosurgery, Tohoku University Graduate School of Medicine, Sendai, Miyagi, Japan.
DOI:10.25259/SNI_874_2020
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Masahito Katsuki1, Norio Narita1, Kazuya Sugawara2, Siqi Cai1, Shinya Shimabukuro1, Ohmi Watanabe1, Naoya Ishida1, Teiji Tominaga3. A case with bilateral thalamic infarction manifesting mutism – Cerebral blood flow and neural fibers evaluation. 02-Mar-2021;12:84
How to cite this URL: Masahito Katsuki1, Norio Narita1, Kazuya Sugawara2, Siqi Cai1, Shinya Shimabukuro1, Ohmi Watanabe1, Naoya Ishida1, Teiji Tominaga3. A case with bilateral thalamic infarction manifesting mutism – Cerebral blood flow and neural fibers evaluation. 02-Mar-2021;12:84. Available from: https://surgicalneurologyint.com/surgicalint-articles/10615/
Date of Submission
04-Dec-2020
Date of Acceptance
09-Feb-2021
Date of Web Publication
02-Mar-2021
Abstract
Background: Acute bilateral thalamic infarction is rare, and occlusion of the artery of percheron (AOP) may be one of its reasons. AOP occlusion results in an acute disturbance of consciousness, but mutism due to AOP occlusion is rare. We described a mutism patient with bilateral thalamic infarction presumably due to AOP occlusion. We also performed cerebral blood flow (CBF) evaluation by N-isopropyl-p-[123I]-iodoamphetamine single-photon emission computed tomography (123I-IMP-SPECT) as well as neural fiber evaluation by diffusion tensor tractography, discussing the mechanism of mutism.
Case Description: A 92-year-old woman presented a gradual deterioration of consciousness. Diffusion-weighted images revealed high-intensity areas at the bilateral thalami, and we diagnosed AOP occlusion. We administered a recombinant tissue plasminogen activator. On day 14, her Glasgow Coma Scale score was 11 (E4V1M6), and she did not present any apparent paresis. She was mute but cognitively alert, although she could communicate by nodding or facial expression. 123I-IMP-SPECT showed CBF increase in the bilateral cerebellum and CBF decrease in the infarcted bilateral thalami and frontal lobes. Diffusion tensor tractography revealed the bilateral dentatothalamo-cortical tracts (DTCs). However, the tracts terminated at the parieto-occipital cortex, but not at the frontal cortex. She still had mutism on day 30.
Conclusion: We reported the bilateral thalamic infarction patient presumably due to AOP occlusion, who presented mutism. The discontinuity of the bilateral DTCs resulted in her mutism, and our results supported the hypothesis that the cerebellum plays a significant role in uttering, associated with the bilateral DTCs.
Keywords: Artery of Percheron, Bilateral thalamic infarction, Dentato-thalamo-cortical pathway, Diffusion tensor tractography, N-isopropyl-p-[123I]-iodoamphetamine single-photon emission computed tomography
INTRODUCTION
Acute bilateral thalamic infarction is uncommon, ranging from 0.1% to 0.3% of all ischemic strokes.[
We herein described a mutism patient with bilateral thalamic infarction presumably due to AOP occlusion. Notably, we performed CBF evaluation by N-isopropyl-p-[123I]-iodoamphetamine single-photon emission computed tomography (123I-IMP-SPECT) as well as neural fiber evaluation through the thalamus by diffusion tensor tractography,[
CASE DESCRIPTION
A 92-year-old woman presented to our emergency room with gradual deterioration of consciousness. She had been taking antihypertensive and diuretic medications for hypertension. Her blood pressure was 157/98 mmHg on admission, and her Glasgow coma scale (GCS) score was 6 (E1V1M4). The head computed tomography did not show any hemorrhagic stroke, but diffusion-weighted images (DWIs) revealed high-intensity areas at the bilateral thalami. Both the cerebellum, supplementary motor areas, and prefrontal areas were bilaterally intact on the DWIs [
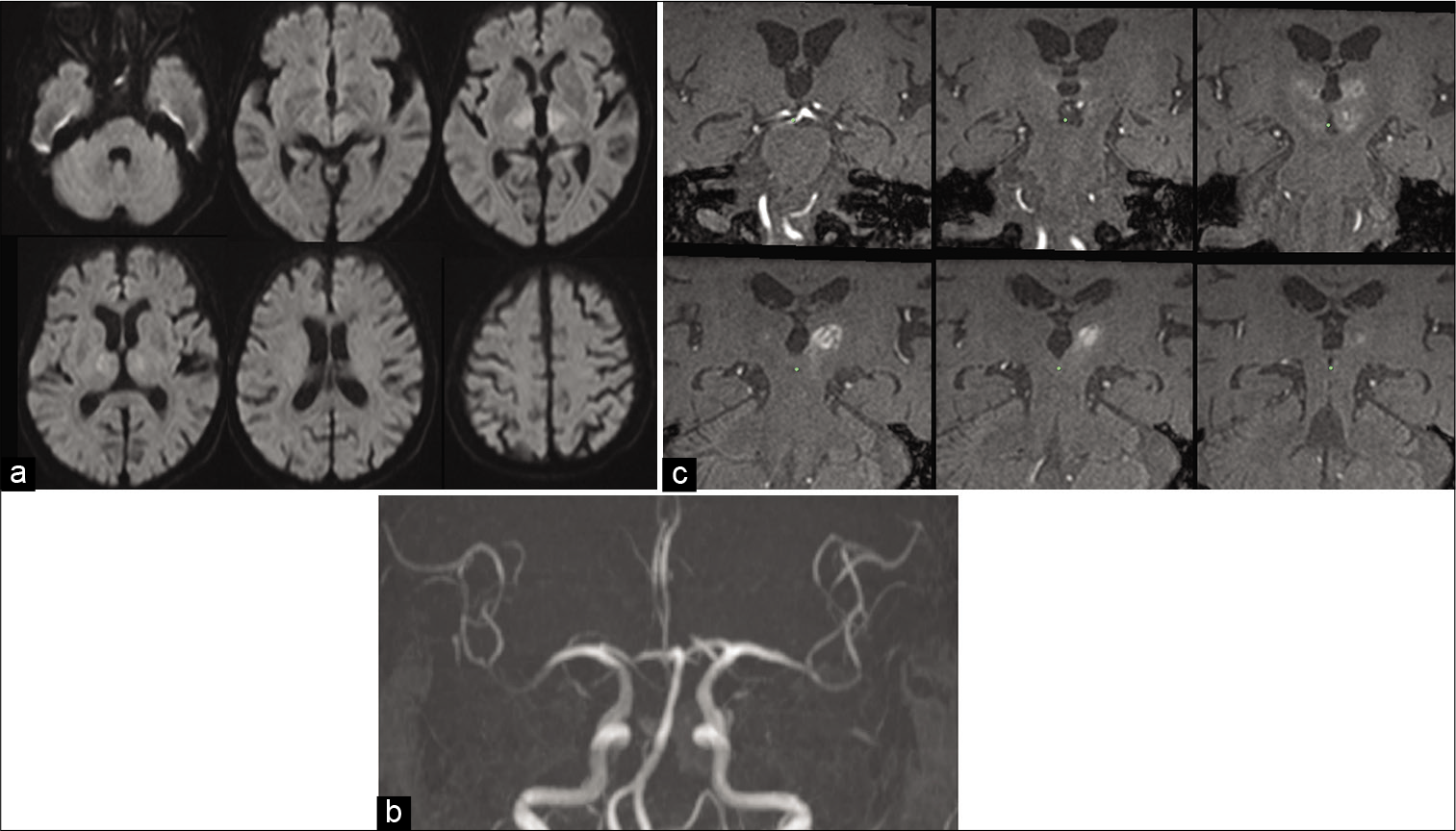
Figure 1:
Diffusion-weighted images (DWIs) revealed high-intensity areas at the bilateral thalami. Both the cerebellum, supplementary motor areas, and prefrontal areas were bilaterally intact on the DWIs (a). Magnetic resonance angiography showed a patent basilar artery, suggesting an occlusion of the artery of Percheron (b). Time-of-flight magnetic resonance imaging revealed high-intensity areas at the bilateral thalami involving the dorsolateral nuclei, dorsoposterior nuclei, central medial nuclei, parafascicular nuclei, and probably the posterior aspects of the anterior thalamic nuclear group (c).
On the following day, her consciousness was GCS score 7 (E2V1M4). The lesions did not enlarge on DWIs. Rehabilitation and tube feeding were started, and her neurological status gradually improved. On day 14, her GCS score was 11 (E4V1M6), and she did not present any apparent paresis. She was mute but cognitively alert, although she could communicate by nodding, shaking her head, or facial expression. Time-of-flight magnetic resonance imaging revealed high-intensity areas at the bilateral thalami involving the dorsolateral nuclei, dorsoposterior nuclei, central medial nuclei, parafascicular nuclei, and probably the posterior aspects of the anterior thalamic nuclear group. These infarcted lesions might compress the ventral anterior and ventral lateral nuclei [
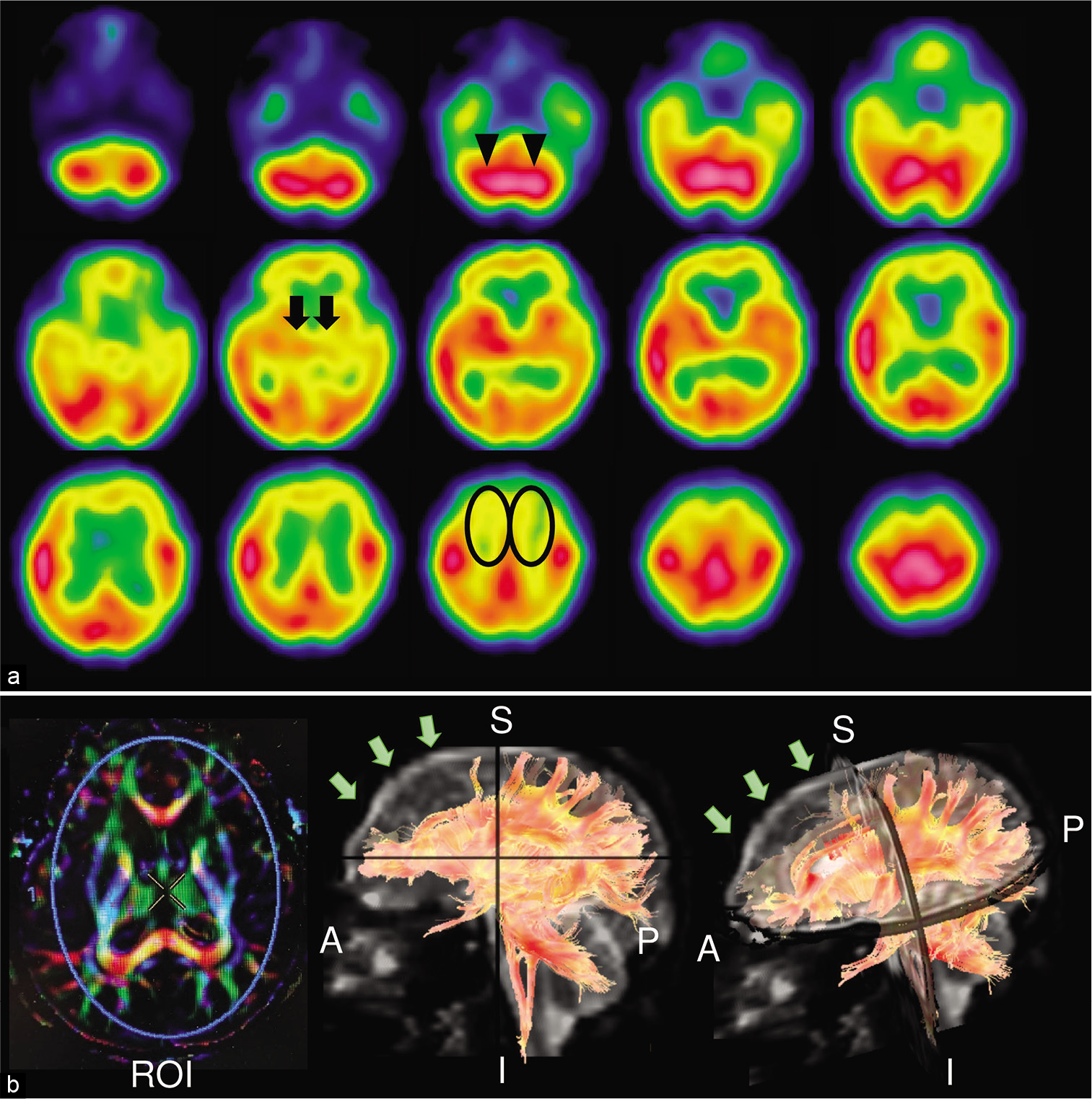
Figure 2:
N-isopropyl-p-[123I]-iodoamphetamine single-photon emission computed tomography (123I-IMP-SPECT) showed cerebral blood flow (CBF) increase in the bilateral cerebellar hemispheres (arrows heads in a). However, CBF was decreased in the infarcted bilateral thalami and frontal lobes, including bilateral supplementary motor areas and prefrontal areas (arrows and circles in a, each). Diffusion tensor tractography revealed the bilateral corticospinal tracts and the cerebello-thalamo-cortical tracts, which were obtained with the region of interest, including bilateral thalami (blue circle in b). However, the cerebello-thalamo-cortical tracts terminated at the parieto-occipital cortex, but not at the frontal cortex (arrows in b). Three-dimensional anisotropy contrast is left in (b). Lateral and oblique views of the tractography are middle and right in (b). A: Anterior, I: Inferior, P: Posterior, ROI: Region of interest, S: Superior.
DISCUSSION
Projections of thalamic nuclei and epithalamus
The thalamus is an important relay station in the brain and subcortical integrator. All of the principal sensory paths except the olfactory system send fibers to the thalamic nuclei. Furthermore, it receives input from the basal nuclei, the hypothalamus, the cerebellum, the visual and auditory systems, and most areas of the cerebral cortex. The thalamus’ gray matter is divided into four groups; the anterior nuclei, the ventrolateral nuclei, the dorsolateral nuclei, and the medial nuclei. The various afferent and efferent connections through these nuclei have significant roles.
The anterior nuclei have afferent connections with the mammillary bodies through the mammillothalamic fibers (the bundle of Vicq-dAzyr) and bidirectional connections with the cingulate gyrus. They are related to the limbic system.
In the ventrolateral nuclei group, both the ventral anterior and ventral lateral nuclei receive input from the globus pallidus, while the ventral lateral nucleus also receives input from the cerebellum and the red nucleus. Both nuclei project to area 6 of the premotor area, so the injury of ventral anterior and ventral lateral nuclei causes motor impairment. On the other hand, the ventral posterior nuclear complex is the principal thalamic receiving area of the large ascending sensory systems. The ventral posterolateral nucleus receives somatosensory input mainly from the spinothalamic tracts. The ventral posteromedial nucleus receives input from the trigeminal and gustatory pathways. These nuclei relay the cortical projections to the primary and secondary somatosensory areas.
The dorsolateral nuclei group has the pulvinar. The pulvinar has a reciprocal projection to the parietal and occipital lobes. The pulvinar receives input from the medial and lateral geniculate bodies and the ventral posterior nucleus and receives direct input from the optic and auditory tracts. The dorsolateral nucleus, also known as the integrative nucleus group, receives input from various nuclei of the thalamus and projects to the parietal lobe.
The medial nuclei group has reciprocal connections with the frontal lobe of the cortex, areas 9, 10, 11, and 12. It also receives input from the amygdala and orbital regions of the frontal lobe. When the medial nuclei are injured, frontal lobe symptoms, mainly disinhibition, and appear.
As other essential nuclei, the intralaminar centromedian nuclei have an important role in the ascending reticular activation system, which maintains wakefulness.
Epithalamus has the habenula nucleus and pineal body. The stria medullaris from the forebrain, septal nuclei, and the tractus retroflexus of Meynert nuclei connect to the habenula. The habenula forms a distinctive rostrocaudal strip along the thalamus’ dorsomedial corner. The habenula is an important brain structure in the regulation of neurotransmission of monoamines such as dopamine and serotonin, which are related to depression. The pineal body receives information about the light-dark cycle from the environment. It conveys this information to produce and secretes the hormone melatonin related to the circadian rhythm.[
Mechanism of mutism and its speculation
Mutism is defined as the inability to speak despite cognitive alertness. It can occur due to lesions in several parts of the brain, such as Broca’s area, the supplementary motor area, thalamus, mesencephalic reticular formation regions, and bilateral hemispheric lesions.[
Our patients presented mutism due to bilateral thalamic infarction. 123I-IMP-SPECT revealed a CBF increase in the cerebellum but a decrease in the bilateral thalami and frontal lobes. This suggested that cerebellar blood flow increased to utter words by stimulating the frontal cortex through the DTCs,[
We should hypothesize other mechanisms because our radiological findings did not clearly show the injury at the ventral lateral and ventral anterior nuclei [
CONCLUSION
We reported the bilateral thalamic infarction presumably due to AOP occlusion, who presented mutism. 123I-IMP-SPECT revealed a CBF increase in the cerebellum but a decrease in the thalami and frontal lobes. Furthermore, diffusion tensor tractography showed neural fiber discontinuity from the thalamus to the frontal cortex.
Presumably, the discontinuity of the bilateral DTCs resulted in her mutism. We should consider other mechanisms causing mutism, but our case supports the hypothesis that the cerebellum plays a significant role in uttering associated with the bilateral DTCs.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Abe H, Endo H, Chiba T, Nagamine Y, Masafumi J, Fujiwara S. Clinical practice of diffusion tensor imaging in the physical therapy. J Jpn Phys Ther Assoc. 2016. 43: 349-57
2. Ackermann H, Mathiak K, Riecker A. The contribution of the cerebellum to speech production and speech perception: Clinical and functional imaging data. Cerebellum. 2007. 6: 202-13
3. Arauz A, Patiño-Rodríguez HM, Vargas-González JC, Arguelles-Morales N, Silos H, Ruiz-Franco A. Clinical spectrum of artery of percheron infarct: Clinical-radiological correlations. J Stroke Cerebrovasc Dis. 2014. 23: 1083-8
4. Castaigne P, Lhermitte F, Buge A, Escourolle R, Hauw JJ, Lyon-Caen O. Paramedian thalamic and midbrain infarcts: Clinical and neuropathological study. Ann Neurol. 1981. 10: 127-48
5. Cavanna AE, Bertero L, Cavanna S, Servo S, Strigaro G, Monaco F. Persistent akinetic mutism after bilateral paramedian thalamic infarction. J Neuropsychiatry Clin Neurosci. 2009. 21: 351
6. Kamaşak T, Sahin S, Eyüboʇlu I, Reis GP, Cansu A. Bilateral paramedian thalamic syndrome after infection. Pediatr Neurol. 2015. 52: 235-8
7. Katsuki M, Narisawa A, Karibe H, Kameyama M, Tominaga T. Mutism resulting from heterochronic bilateral cerebellar hemorrhages-a case report. Surg Neurol Int. 2019. 10: 122
8. Lazzaro NA, Wright B, Castillo M, Fischbein NJ, Glastonbury CM, Hildenbrand PG. Artery of percheron infarction: Imaging patterns and clinical spectrum. AJNR Am J Neuroradiol. 2010. 31: 1283-9
9. Naito Y, Kuzuhara S, Yamanouchi H. Complete recovery from akinetic mutism caused by bilateral thalamic infarction. Clin Neurol. 1986. 26: 817-20
10. Nishikawa M, Komiyama M, Sakamoto H, Yasui T, Nakajima H. Cerebellar mutism after basilar artery occlusion-case report. Neurol Med Chir (Tokyo). 1998. 38: 569-73
11. Palesi F, Tournier JD, Calamante F, Muhlert N, Castellazzi G, Chard D. Contralateral cerebello-thalamo-cortical pathways with prominent involvement of associative areas in humans in vivo. Brain Struct Funct. 2015. 220: 3369-84
12. Percheron G. The anatomy of the arterial supply of the human thalamus and its use for the interpretation of the thalamic vascular pathology. Z Neurol. 1973. 205: 1-13
13. Pluchon C, Jaafari N, Loiseau-Corvez MN, Parizel A, Vandermarcq P, Hankard R. A child with mutism after bilateral thalamic infarction. J Clin Neurosci. 2011. 18: 1738-40
14. Robles A, Aldrey JM, Fernández RM, Suárez C, Corredera E, Leira R. Paramedian bithalamic infarct syndrome: Report of five new cases. Rev Neurol. 1995. 23: 276-84
15. Rondot P, de Recondo J, Davous P, Bathien N, Coignet A. Bilateral thalamic infarcts with abnormal movements and permanent amnesia. Rev Neurol (Paris). 1986. 142: 398-405
16. Schunke M, Schulte E, Schumacher U, Sakai T, Kawata M.editors. Prometheus LernAtlas der Anatomie: Kopf, Hals und Neuroanatomie. Tokyo: Igaku Shoin; 2014. p.
17. Shetty AC, Morris J, O’Mahony P. Akinetic mutism-not coma. Age Ageing. 2009. 38: 350-1
18. Tanaka K, Fujishima H, Motomura S, Tamura K, Miyoshi T, Uchino A. A case of dural arteriovenous malformation with bilateral thalamic infarction. Brain Nerve. 1986. 38: 1005-10
19. van Domburg PH, ten Donkelaar HJ, Notermans SL. Akinetic mutism with bithalamic infarction, Neurophysiological correlates. J Neurol Sci. 1996. 139: 58-65
20. Wells M, Jacques R, Odasso MM. Thalamic infarct presenting as catastrophic life-threatening event in an older adult. Aging Clin Exp Res. 2011. 23: 320-2

