

- Department of Neurosurgery, Dow University of Health and Sciences,
- Department of Neurosurgery, Jinnah Postgraduate Medical Centre,
- Department of Neurosurgery, Liaquat National Hospital,
- Department of Neurosurgery, Liaquat National Hospital and Medical College,
- Department of Histopathology, Liaquat National Hospital, Karachi, Sindh, Pakistan.
Correspondence Address:
Areesha Shakeel
Department of Histopathology, Liaquat National Hospital, Karachi, Sindh, Pakistan.
DOI:10.25259/SNI_584_2019
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Nimrah Ali, Areesha Shakeel, Yousuf Shaikh, Salman Sharif, Atif Hashmi. Atypical sellar cyst: A rare case. 20-Jun-2020;11:155
How to cite this URL: Nimrah Ali, Areesha Shakeel, Yousuf Shaikh, Salman Sharif, Atif Hashmi. Atypical sellar cyst: A rare case. 20-Jun-2020;11:155. Available from: https://surgicalneurologyint.com/surgicalint-articles/10090/
Date of Submission
05-Dec-2019
Date of Acceptance
03-Jun-2020
Date of Web Publication
20-Jun-2020
Abstract
Background: Sellar cysts are common in neurosurgery. Around 90% of these are diagnosed as pituitary adenomas. The other 10% are nonadenomatous, inflammatory, infective, metastatic, or cystic in nature. Some rare cysts include dermoid, epidermoid, colloid, and arachnoid. They all have different histological features. The case we present demonstrates a unique cyst with features that are not previously documented.
Case Description: A 60-year-old female presented to the neurosurgical department complaining of blurring of vision and severe headache for more than ½ year. Imaging was done which revealed a bony erosive lesion in the region of sella. Magnetic resonance imaging with contrast showed high signals with no contrast enhancement. A clear diagnosis could not be made based on radiology. Surgery was done and sample was sent for histopathology. Based on histopathological report findings, a diagnosis of benign atypical sellar cyst was made. Post procedure, the patient recovered and was discharged.
Conclusion: Sellar cysts present similarly. They are differentiated based on their histological features. The sellar cyst we encountered had features different from the ones already described in the literature.
Keywords: Benign epithelial cyst, Endoscopy, Sellar cyst
INTRODUCTION
Sellar lesions are frequently encountered in neurosurgical clinics. The clinical presentation of sellar lesions is more or less similar. Common signs and symptoms include headaches, visual disturbances, hydrocephalus, focal neurological deficits and variable changes in mental state. Despite significant similarity in clinical features, the differential diagnoses for sellar lesions are vast. 90% of all sellar masses are pituitary adenomas.[
CASE PRESENTATION
A 60-years-old female with chronic hypertension, came to neurosurgical clinic with history of gradually progressive bilateral blurring of vision for 7 months and severe, headache for 3 months.
Neurological examination and systemic examination of this lady were normal without deficits.
Hematological and biochemical tests were within normal parameters. However, pituitary function tests revealed raised ACTH = 143 pg/ml. Rest of the pituitary hormones’, i.e., follicle stimulating, luteinizing, thyroid-stimulating hormone, prolactin, and insulin-like growth factor levels were within normal range.
On imaging, computed tomography scan bran revealed erosive lesion in region of sella causing bony destruction and remodeling [
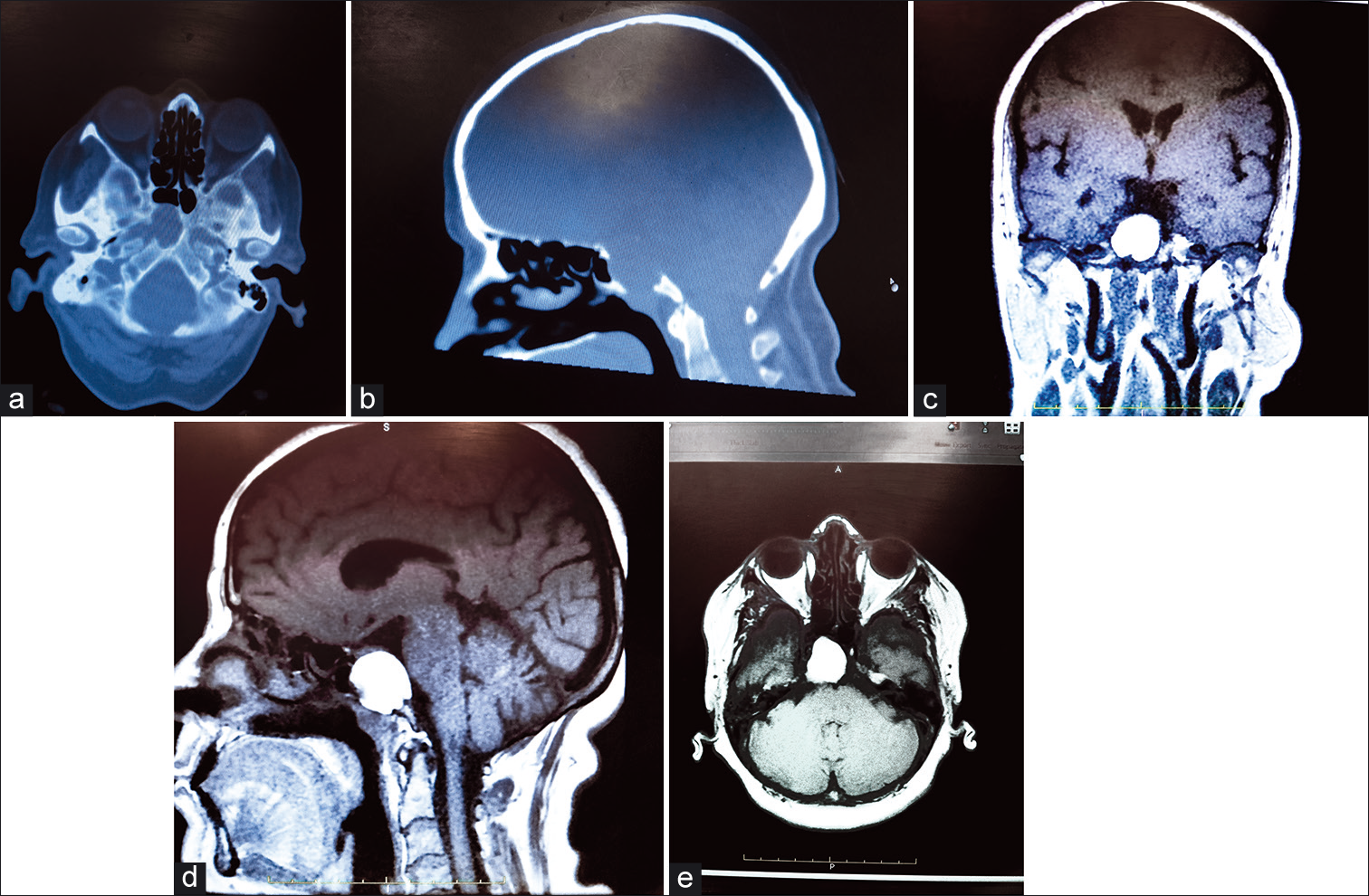
At this point, a clear diagnosis could not be made due to atypical radiological features. Hence, patient was planned for surgery + biopsy of suspected lesion.
After careful planning, the cyst was removed by a routine trans-nasal trans-spenoidal endoscopic approach. The cyst contained greenish jelly like material which was removed completely along with the cyst wall. The contents were sent for histopathological examination.
Histopathological examination revealed benign cyst lined with flattened squamous epithelium and underlying fibrous tissue. On one region, a pseudostratified ciliated epithelium was also seen. Abundant hemorrhage was seen along with few calcified fragments. There was no evidence of malignancy in the sections examined. A diagnosis of benign atypical sellar cyst was made. This pathology report was reviewed by the head of the department pathology who concurred with the findings.
Post procedure, patient recovered well and was discharged. Her initial symptoms had resolved completely on her follow-up at 4 weeks.
DISCUSSION
A wide variety of mass lesions ranging from benign cysts to malignant tumors can occur within the sellar region. Although differential diagnoses of the sellar lesions are wide, the clinical presentation of these lesions is usually similar with varying severity. It is essential to differentiate and accurately diagnose these lesions as clinical approach, treatment, and outcome for each diagnosis is different.
Among the rare sellar lesions, cystic lesions are not uncommon. Clinically, they mimic pituitary adenomas but they can be differentiated from adenomas on imaging. A wide variety of sellar cystic lesions have been identified ranging from benign Rathke’s cleft cysts to neoplastic craniopharyngiomas.[
The sellar cyst in our case could not be classified as primary or secondary cyst based on its histological diagnosis. In 1994, Harrison et al. microscopically examined 19 cases of sellar cystic lesions, 16 out which fell under distinct categories but the remaining three could not be classified according to the formal classification. They also showed that there is a significant overlap between the histological findings of sellar cysts and they all are the representative of a continuum of ectodermally derived cystic lesions. Histologically, different cysts have different characteristics but most are nonneoplastic.[
Previously many cases of symptomatic sellar Rathke’s cleft cysts[
Although histological classification of sellar cystic lesions is vast, their treatment is almost always surgical. The treatment approach for cysts depends on the symptomatology, size, pituitary function, and coexistence of pituitary adenoma.[
CONCLUSION
An elderly female presented in our neurosurgical department with a sellar mass. Radiological imaging was done which showed atypical signs that were non-diagnostic. After endoscopic resection, the specimen obtained was sent for histopathology which revealed unique and benign features. A diagnosis of simple cyst was made. This case is distinctive because the histopathological features of the cyst do not fit into any previously described category.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Publication of this article was made possible by the James I. and Carolyn R. Ausman Educational Foundation.
Conflicts of interest
There are no conflicts of interest.
References
1. Andrysiak-Mamos E, Sagan K, Sagan L, Sowińska-Przepiera E, Syrenicz A. Cystic lesions of the sellar-suprasellar region-diagnosis and treatment. Endokrynol Pol. 2018. 69: 212-28
2. Baskin D, Wilson C. Transsphenoidal treatment of non-neoplastic intrasellar cysts. A report of 38 cases. J Neurosurg. 1984. 60: 8-13
3. Glezer A, Paraiba D, Bronstein M. Rare sellar lesions. Endocrinol Metab Clin North Am. 2008. 37: 195-211
4. Güdük M, HamitAytar M, Sav A, Berkman Z. Intrasellar arachnoid cyst: A case report and review of the literature. Int J Surg Case Rep. 2016. 23: 105-8
5. Harrison M, Morgello S, Post K. Epithelial cystic lesions of the sellar and parasellar region: A continuum of ectodermal derivatives?. J Neurosurg. 1994. 80: 1018-25
6. Huang B, Castillo M. Nonadenomatous tumors of the pituitary and Sella turcica. Top Magn Reson Imaging. 2005. 16: 289-99
7. Iqbal J, Kanaan I, Homsi M. Non-neoplastic cystic lesions of the sellar region presentation, diagnosis and management of eight cases and review of the literature. Acta Neurochir (Wien). 1999. 141: 389-98
8. Naik V, Thakore N. A case of symptomatic Rathke’s cyst. Case Rep. 2013. 2013: bcr2012006943-
9. Park K, Gwak H, Hong E, Lee S. Inflamed symptomatic sellar arachnoid cyst: Case report. Brain Tumor Res Treat. 2013. 1: 28-31
10. Tanaka T, Oka H, Kawano N, Kobayashi I, Saegusa H, Fujii K. Juvenile symptomatic Rathke’s cleft cyst--case report. Neurol Med Chir (Tokyo). 1998. 38: 578-81
11. Valassi E, Biller BM, Klibanski A, Swearingen B. Clinical features of nonpituitary sellar lesions in a large surgical series. Clin Endocrinol (Oxf). 2010. 73: 798-807
12. Zada G, Lin N, Ojerholm E, Ramkissoon S, Laws E. Craniopharyngioma and other cystic epithelial lesions of the sellar region: A review of clinical, imaging, and histopathological relationships. Neurosurg Focus. 2010. 28: E4-

