

- Department of Neurosurgery, Instituto de Assistência Médica ao Servidor Público Estadual, Sao Paulo, Brazil.
Correspondence Address:
Matheus Fernandes de Oliveira, Department of Neurosurgery, Instituto de Assistência Médica ao Servidor Público Estadual, Sao Paulo, Brazil.
DOI:10.25259/SNI_1243_2021
Copyright: © 2022 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Anselmo Alves Boa Sorte, Cesar Carvalho Garcia, Mateus Reghin Neto, Matheus Fernandes de Oliveira, Jose Marcus Rotta. Brain cryptococcoma mimicking a glioblastoma in an immunocompetent patient: A rare case report and comprehensive review. Surg Neurol Int 31-Mar-2022;13:114
How to cite this URL: Anselmo Alves Boa Sorte, Cesar Carvalho Garcia, Mateus Reghin Neto, Matheus Fernandes de Oliveira, Jose Marcus Rotta. Brain cryptococcoma mimicking a glioblastoma in an immunocompetent patient: A rare case report and comprehensive review. Surg Neurol Int 31-Mar-2022;13:114. Available from: https://surgicalneurologyint.com/surgicalint-articles/11504/
Date of Submission
16-Dec-2021
Date of Acceptance
03-Mar-2022
Date of Web Publication
31-Mar-2022
Abstract
Background: Cryptococcosis is an invasive fungal infection primarily affecting lungs and potentially spreading to the central nervous. This fungal infection might be misdiagnosed as other infection diseases, such as tuberculosis; granulomatous diseases, like sarcoidosis; and even neoplastic diseases. Some previous reports described cases of cryptococcomas resembling brain tumors. In this paper, we present a very rare presentation of brain cryptococcoma mimicking a malignant glioma. To the best of our knowledge, this is the third case description in the literature.
Case Description: A 64-year-old male patient presented at the hospital with a history of progressive frontal headache for 1 month, becoming moderate to severe, associated with visual changes, without nausea or vomiting. No fever was reported. He was a heavy smoker and denied other relevant previous medical data. Neuroimage disclosed a right temporal expansive lesion initially considered a malignant glioma. The patient underwent a right temporal craniotomy and biopsy revealed a cryptococcoma.
Conclusion: Cryptococcomas characteristics in magnetic resonance are quite nonspecific. They should always be included in differential diagnosis of expansive brain lesions, both malignant and benign. Therefore, once cryptococcomas may resemble like other intracranial expansive lesions, biopsy should always be carried out to clarify diagnosis and avoid inadequate treatment and definition of prognosis only based on radiological patterns.
Keywords: Brain neoplasm, Differential diagnosis, Neurocryptococcosis, Surgery
INTRODUCTION
Cryptococcosis is an invasive fungal infection primarily affecting lungs and potentially spreading to the central nervous.[
Cryptococcosis is the most common opportunistic fungal infection in the central nervous system in patients with human immunodeficiency virus (HIV) or other immunodeficiencies.[
Diagnosis of neurocryptococcosis is usually done based on clinical picture and typical association with HIV. Cerebrospinal fluid (CSF) evaluation and neuroimage methods may also help. Once diagnosis is established, treatment is potentially successful with antifungal therapy.[
This fungal infection might be misdiagnosed as other infection diseases, such as tuberculosis; granulomatous diseases, like sarcoidosis; and even neoplastic diseases. Cryptococcoma presentation in neuroimage methods may also be indistinguishable from other mass lesions such as metastasis, malignant gliomas, and pyogenic abscesses. Thus, cryptococcoma should always be included in the differential diagnosis of expansive brain lesions, both malignant and benign.[
CASE DESCRIPTION
A 64-year-old male patient presented at the hospital assistance with a history of progressive frontal headache for 1 month, becoming moderate to severe, associated with visual changes, without nausea or vomiting. No fever was reported. He was a heavy smoker and denied other relevant previous medical data.
An outpatient investigation had carried out with a neurologist. A skull tomography computerized tomography (CT) was done and showed a right temporo-parieto-occipital hypodensity [
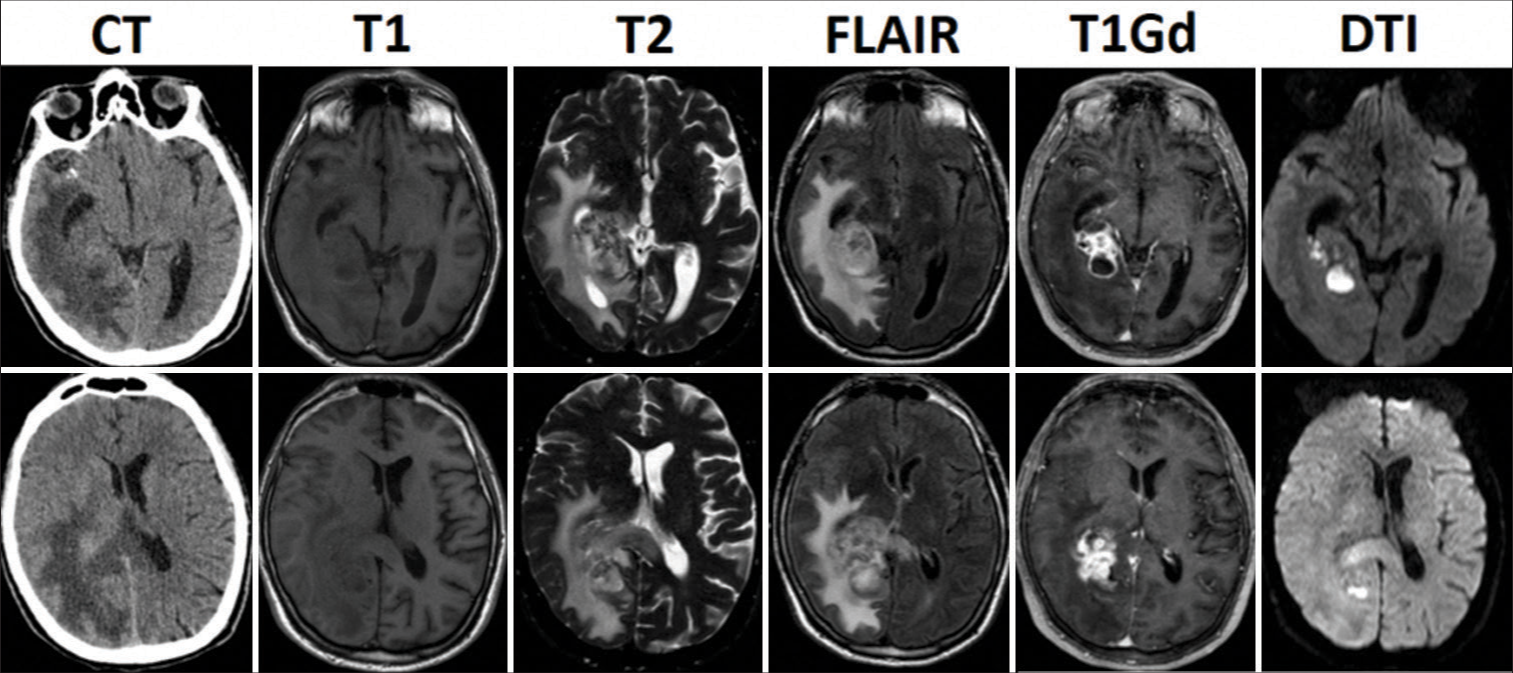
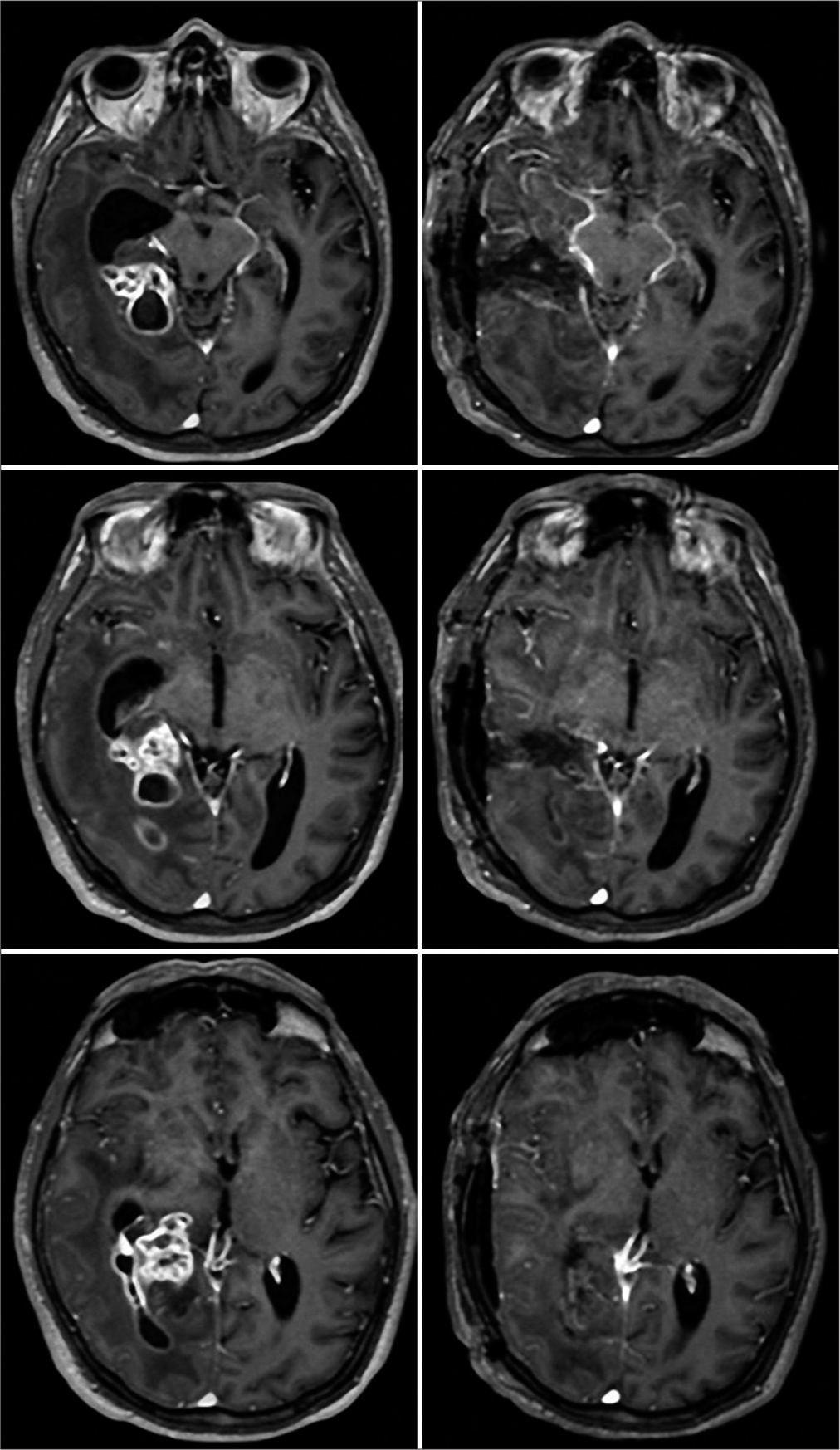
Figure 1:
Preoperative neuroimage of patient. We present preoperative computed tomography and MR in sequences T1, T2, FLAIR, and T1 with gadolinium and diffusion. MR disclosed an expansive right temporal lesion. It was solid-cystic, hyperintense at T1, and hypointense at T2, with heterogeneous enhancement after gadolinium injection.
He performed a magnetic resonance [MR-
Clinical picture and radiological findings pointed to a case of cerebral malignancy, being a malignant glioma the probable diagnosis. Therefore, microsurgical resection was planned. In the preoperative investigation, a routine thoracic and cardiological screening with a chest CT revealed an oval lesion with regular shape in the posterior segment of the upper lobe of the right lung, measuring 0.9 cm, suggestive of a lymph node. This lesion was considered unspecific and benign.
Surgery
Surgical planning and execution occurred as usual. The patient was positioned in supine position and head rotation of 90°. We routinely use neuronavigation in neuro-oncological surgeries to improve approach and decrease complications. The patient underwent a right temporal craniotomy, approaching lesion through middle temporal gyrus, to the temporal horn of the ventricle. Lesion had a hardened aspect and when it was dissected, it released a yellowish pasty content, which resembled an exudative content. In addition, the area around the lesion had an infiltrative or edematous aspect. Lesion had normal bleeding, not suggestive of malignant glioma. Main precaution during surgery was to preserve arachnoidal plane and work in an intrapial plane, especially in mesial portion of tumor.
Frozen resection was performed and partial report was of inflammatory unspecific process. Material was sent for pathological analysis.
Pathological report
Histology revealed in hematoxylin-eosin stain a moderate mixed inflammatory infiltrate with a foreign body-type giant cell reaction permeating capsulated structures. In GomoriGrocott stain, it was possible to see multiple capsulated structures, round to oval with thin cell walls of variable size [3.5–8 μm in diameter –
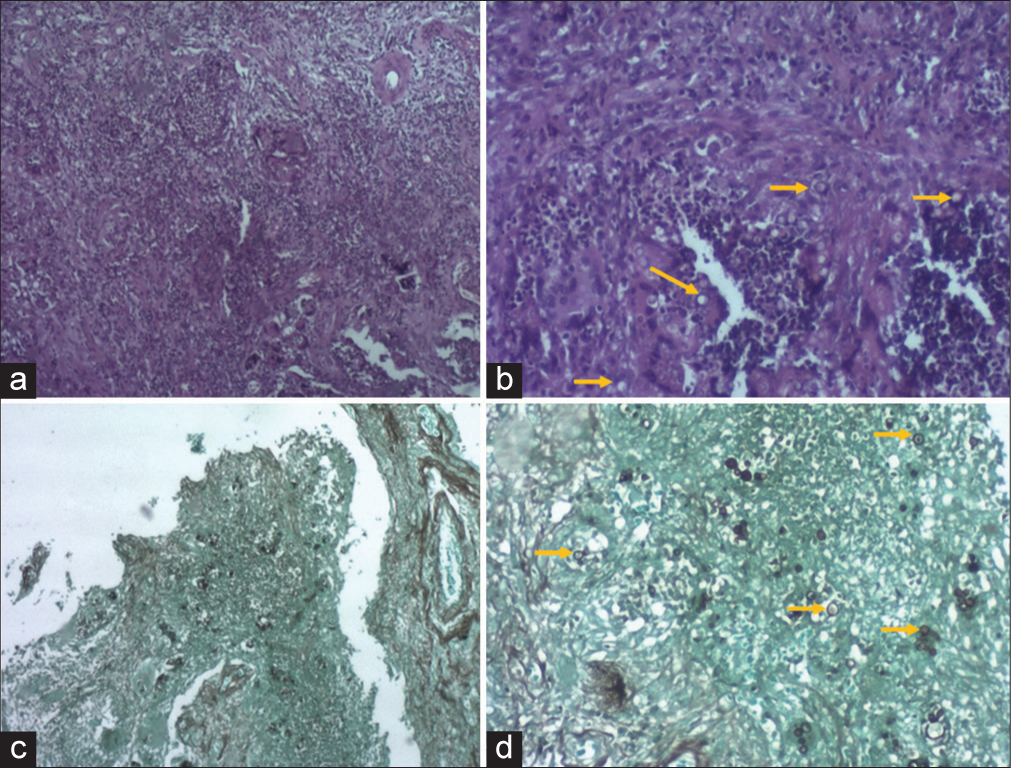
Figure 4:
Histology image. In (a), histological section stained by H and E ×40, brain parenchyma is shown, showing a moderate mixed inflammatory infiltrate with a foreign body-type giant cell reaction permeating capsulated structures. (b) This same cut, enlarged at 100×, revealing a moderate mixed inflammatory infiltrate and round to oval capsulated structures. In (c), a GomoriGrocott stain, enlarged by ×40, reveals the silver impregnation, showing multiple capsulated structures. Finally, (d), in the same coloration, at 100×, it is possible to notice capsulated structures, round to oval with thin cell walls of variable size (3.5–8 μm in diameter). Arrows show inflammatory infiltrate and round to oval capsulated structures compatible with cryptococcoma.
Treatment
After histopathological results, treatment was initiated with amphotericin B and flucytosine. The patient underwent postoperative magnetic resonance with good surgical results ([
DISCUSSION
Cryptococcosis is an invasive fungal infection primarily affecting lungs and potentially spreading to the central nervous.[
Another important factor related to presentation is the cryptococcal variety involved. C. neoformans is more prevalent in immunocompromised individuals, usually presenting with meningitis, while C. gattii has a higher incidence in immunocompetent individuals, more related to cryptococcoma.[
Radiologically, despite having a more frequent pattern of presentation, cryptococcomas characteristics in magnetic resonance end up being quite nonspecific. In general, cryptococcoma presents as an expansive lesion, hypo or isointense in T1, and hyperintense in T2. Enhancement to gadolinium is variable, generally related to the host response.[
There have been some reports of brain lesions suggestive of neoplasms (both primary and secondary) which turned to be finally diagnosed as cryptococcoma.[
Ang et al.[
Misra et al.[
Previously, only two cases in the literature mimicked high-grade glial neoplasia. Ulett et al.[
Li et al.[
There are also other cases of cryptococcomas mimicking cerebral neoplasm. Yu et al.[
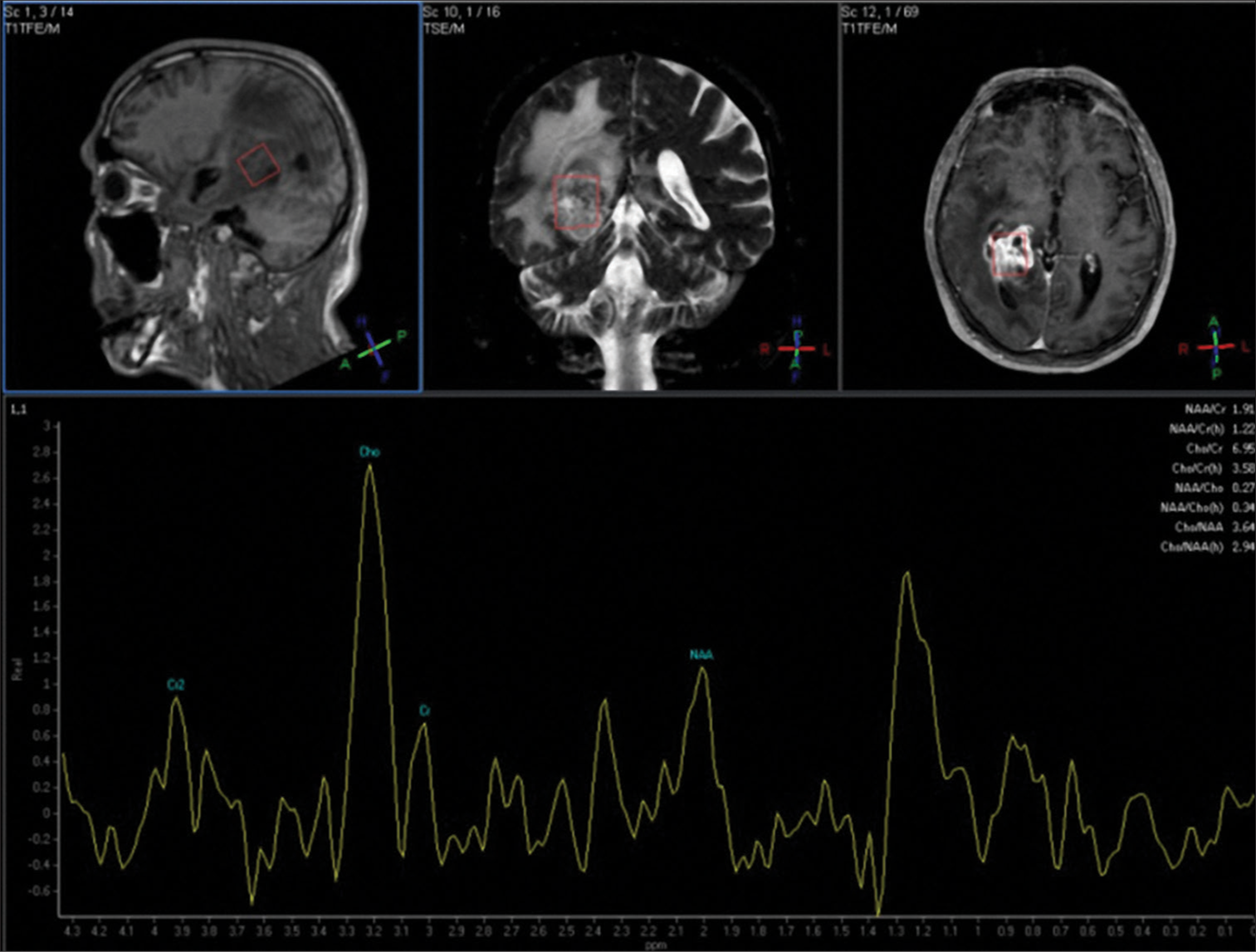
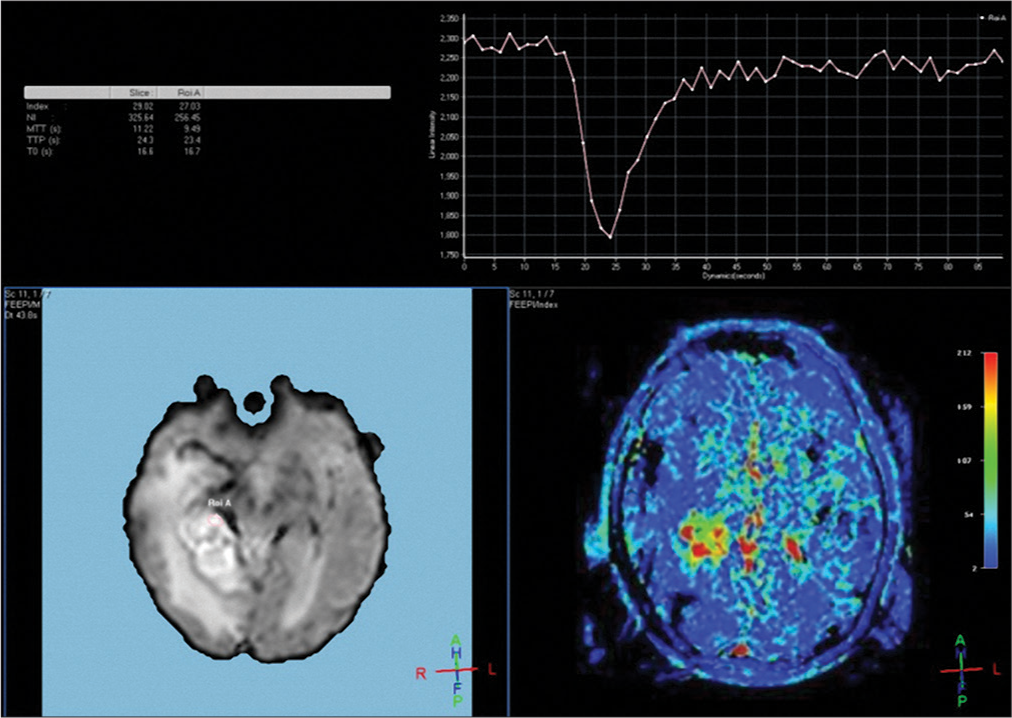
In addition, none of the reports in the literature had a description of the pattern of cryptococcoma neuroimage concerning spectroscopy, which could potentially help diagnostic differentiation. Theoretically, spectroscopy would be one of the fundamental points in differentiating other brain disorders. Classically, it presents an important increase in the lactate peak, in contrast to the reduction in N-acetyl aspartate, choline, and creatine.[
In our case, a 61-year-old man presenting with holocranial headache presented with a right temporal contrast-enhancing expansive lesion suggestive of neoplasm. MR features were indistinguishable from a malignant glioma, including spectroscopy and perfusion studies, which revealed increase in choline similarly to malignant gliomas. Only after surgical approach, it was possible to settle diagnosis of neurocryptococcoma and the preoperative chest CT image was interpreted as a lung cryptococcoma. His HIV test was negative. To the best of our knowledge, our case is the third to present cryptococcomas mimicking glioblastomas in this manner. Moreover, considering spectroscopy pattern, which was also undistinguishable to glioblastoma, it is the first description available.
Although potentially harmful and a life-threatening condition, the central nervous system cryptococcosis is amenable to treatment and cure, even in immunodeficient subjects. Meanwhile, malignant gliomas and other neoplasms including metastases are neoplastic diseases with poor prognosis, leading patient to death, despite of surgical, chemotherapy, and radiotherapy treatment.[
In some cases, including low clinical performance patients harboring malignant gliomas, biopsy may even be not considered due to low oncological benefit. In such cases, there might be a venue for intersection of oncological diagnosis with neurocryptococcoma. Thus, it is possible that a patient considered “palliative” and oncological might have a treatable diagnosis. Therefore, a proper diagnostic workout including biopsy must be posed for all patients, to properly perform diagnosis and guide treatment.
The main learning point is that once cryptococcomas may resemble like other intracranial expansive lesions, biopsy should always be carried out to clarify diagnosis and avoid inadequate treatment and definition of prognosis only based on radiological patterns.
CONCLUSION
Cryptococcomas characteristics in magnetic resonance are quite nonspecific. They should always be included in differential diagnosis of expansive brain lesions, both malignant and benign. Therefore, once cryptococcomas may resemble like other intracranial expansive lesions, biopsy should always be carried out to clarify diagnosis and avoid inadequate treatment and definition of prognosis only based in radiological patterns.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Ang SY, Ng VW, Kumar SD, Low SY. Cryptococcosis mimicking lung carcinoma with brain metastases in an immunocompetent patient. J Clin Neurosci. 2017. 35: 73-5
2. Beardsley J, Sorrell TC, Chen SC. Central nervous system cryptococcal infections in non-HIV infected patients. J Fungi (Basel). 2019. 5: 71
3. Chen S, Chen X, Zhang Z, Quan L, Kuang S, Luo X. MRI findings of cerebral cryptococcosis in immunocompetent patients. J Med Imaging Radiat Oncol. 2011. 55: 52-7
4. Goldman DL, Khine H, Abadi J, Lindenberg DJ, La P, Niang R. Serologic evidence for Cryptococcus neoformans infection in early childhood. Pediatrics. 2001. 107: e66
5. Khandelwal N, Gupta V, Singh P. Central nervous system fungal infections in tropics. Neuroimaging Clin N Am. 2011. 21: 859-66
6. Li Q, You C, Liu Q, Liu Y. Central nervous system cryptococcoma in immunocompetent patients: A short review illustrated by a new case. Acta Neurochir (Wien). 2010. 152: 129-36
7. Misra R, Kumar S, Sharma S. Cryptococcal granuloma of the frontal lobe in an immunocompromised HIV-negative patient. Egypt J Neurosurg. 2020. 35: 4
8. Oliveira FD, Severo CB, Guazzelli LS, Severo LC. Cryptococcus gattii fungemia: Report of a case with lung and brain lesions mimicking radiological features of malignancy. Rev Inst Med Trop Sao Paulo. 2007. 49: 263-5
9. Paiva AL, de Aguiar GB, Lovato RM, Zanetti AV, Panagopoulos AT, Veiga JC. Cryptococcoma mimicking a brain tumor in an immunocompetent patient: Case report of an extremely rare presentation. Sao Paulo Med J. 2018. 136: 492-6
10. Rodrigues DB, De Oliveira Lima L, Pereira EL, de Oliveira Sousa U, de Oliveira MF, Lima AM. Epidemiologia das neoplasias intracranianas no hospital do servidor público estadual de São Paulo: 2010-2012. Arq Bras Neurocirurg Braz Neurosurg. 2014. 33: 6-12
11. Rotta JM, de Oliveira MF, Reis RC, Botelho RV. Malignant transformation of low-grade gliomas in patients undergoing adjuvant therapy. Acta Neurol Belg. 2017. 117: 235-9
12. Rotta JM, Rodrigues DB, Diniz JM, de Abreu BM, Kamimura F, Sousa UO. Analysis of survival in patients with brain metastases treated surgically: Impact of age, gender, oncologic status, chemotherapy, radiotherapy, number and localization of lesions, and primary cancer site. Rev Assoc Med Bras. 2018. 64: 717-22
13. Sakamoto A, Hisaoka M. Pulmonary cryptococcosis mimicking a metastasis in a patient with ewing sarcoma. Respirol Case Rep. 2016. 4: e00181
14. Santander XA, Gutiérrez-González R, Cotúa C, Tejerina E, Rodríguez GB. Intraventricular cryptococcoma mimicking a neoplastic lesion in an immunocompetent patient with hydrocephalus: A case report. Surg Neurol Int. 2019. 10: 115
15. Ulett KB, Cockburn JW, Jeffree R, Woods ML. Cerebral cryptococcoma mimicking glioblastoma. BMJ Case Rep. 2017. 2017: bcr2016218824
16. Yu YQ, Jiang XX, Gao YJ. MRI of a pituitary cryptococcoma simulating an adenoma. Neuroradiology. 1995. 37: 449-50

