

- Department of Neurosurgery, Marche Polytechnic University Faculty of Medicine, Ancona, Marche, Italy.
DOI:10.25259/SNI_120_2020
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Davide Nasi, Mauro Dobran. Can early cranioplasty reduce the incidence of hydrocephalus after decompressive craniectomy? A meta-analysis. 02-May-2020;11:94
How to cite this URL: Davide Nasi, Mauro Dobran. Can early cranioplasty reduce the incidence of hydrocephalus after decompressive craniectomy? A meta-analysis. 02-May-2020;11:94. Available from: https://surgicalneurologyint.com/surgicalint-articles/9988/
Date of Submission
23-Mar-2020
Date of Acceptance
08-Apr-2020
Date of Web Publication
02-May-2020
Abstract
Background: Do alterations of cerebrospinal fluid dynamics secondary to decompressive craniectomy (DC) lead to hydrocephalus, and can this effect be mitigated by early cranioplasty (CP)? In this meta-analysis, we evaluated whether the timing of CP decreased the incidence of postoperative hydrocephalus.
Methods: We performed a systematic search of PubMed/MEDLINE, Scopus, and the Cochrane databases using Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines for English language articles (1990–2020). We included case series, case–control, and cohort studies, and clinical trials assessing the incidence of hydrocephalus in adult patients undergoing early CP (within 3 months) versus late CP (after 3 months) after DC.
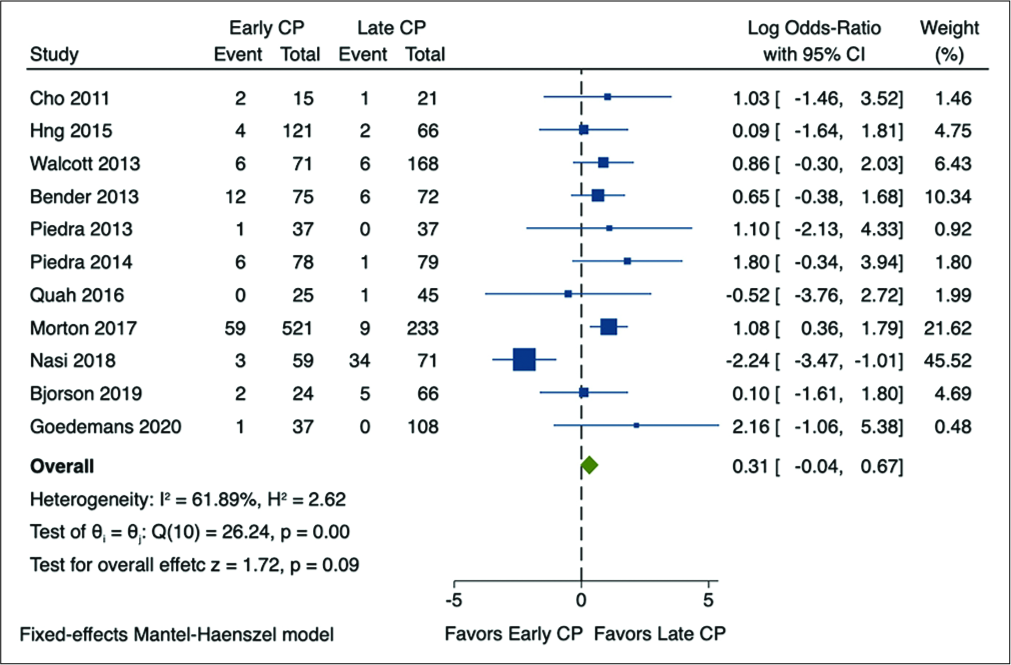
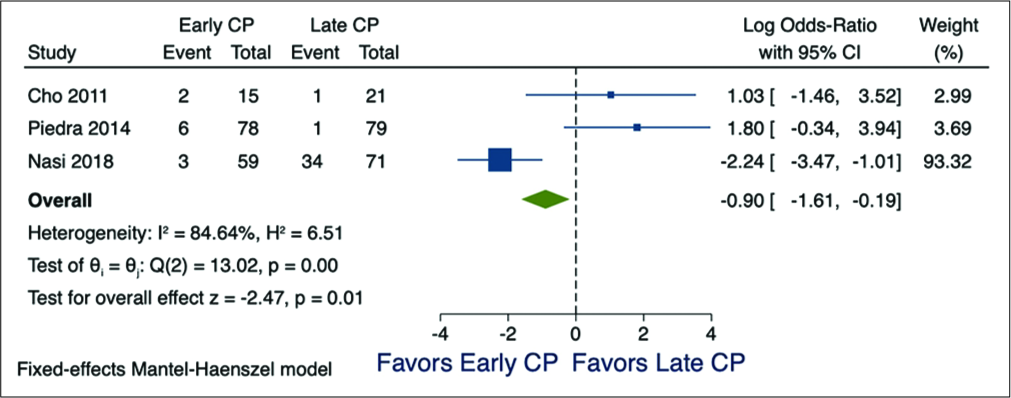
Results: Eleven studies matched the inclusion criteria. The rate of postoperative hydrocephalus was not significantly different between the early (=96/1063; 9.03%) and late CP (=65/966; 6.72%) group (P = 0.09). Only in the three studies specifically reporting on the rate of hydrocephalus after DC performed to address traumatic brain injury (TBI) alone was there a significantly lower incidence of hydrocephalus with early CP (P = 0.01).
Conclusion: Early CP (within 90 days) after DC performed in TBI patients alone was associated with a lower incidence of hydrocephalus. However, this finding was not corroborated in the remaining eight studies involving CP for pathology exclusive of TBI.
Keywords: Cranioplasty, Decompressive craniectomy, Hydrocephalus, Ventriculoperitoneal shunt
INTRODUCTION
Hydrocephalus is one of the main complications of decompressive craniectomy (DC).[
MATERIALS AND METHODS
Search strategy
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines were followed utilizing the PubMed/Medline, Scopus, and Cochrane databases from 1999 to 2020. Keywords included “Cranioplasty, early” or ‘‘cranioplasty, timing.”
Study selection and outcome
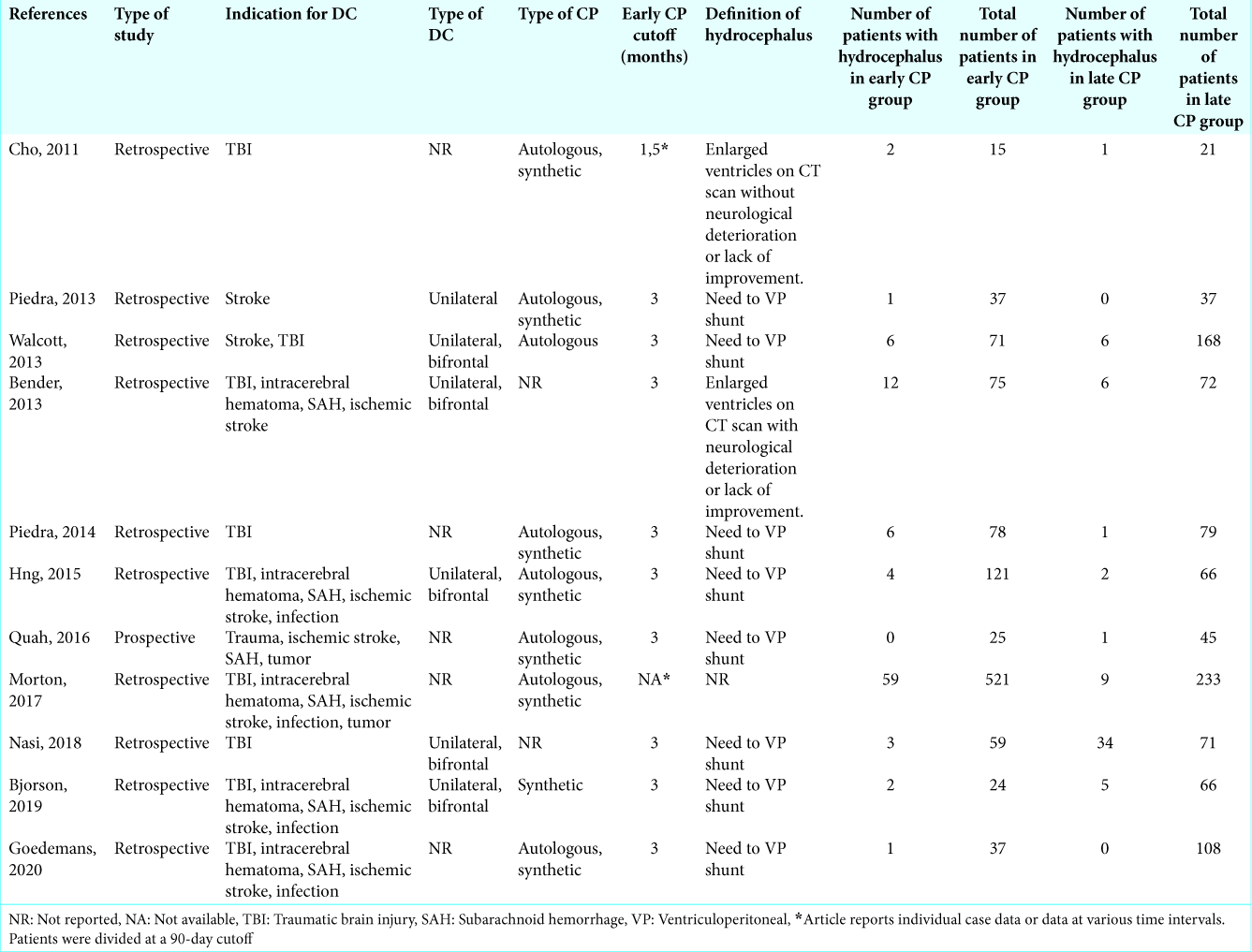
In 11 studies (comparative case control or cohort), we asked whether early CP (i.e., CP ≤3 months) versus later CP differently impacted the rate of hydrocephalus following DC [
Statistical method for meta-analysis
The meta-analysis was performed using STATA/IC 13.1 statistical package (StataCorp LP, College Station, TX, USA). The log odds ratios (LORs) and 95% confidence intervals for each outcome were then reckoned as by “early” and “late” time points. LORs were pooled using the Mantel–Haenszel method with fixed effects model. The I2 metric was reported to further quantify heterogeneity (0% = no heterogeneity, 100% = maximal heterogeneity). P < 0.05 was considered statistically significant.
RESULTS
Inclusion of eleven studies
Eleven studies met the inclusion criteria for this meta- analysis [
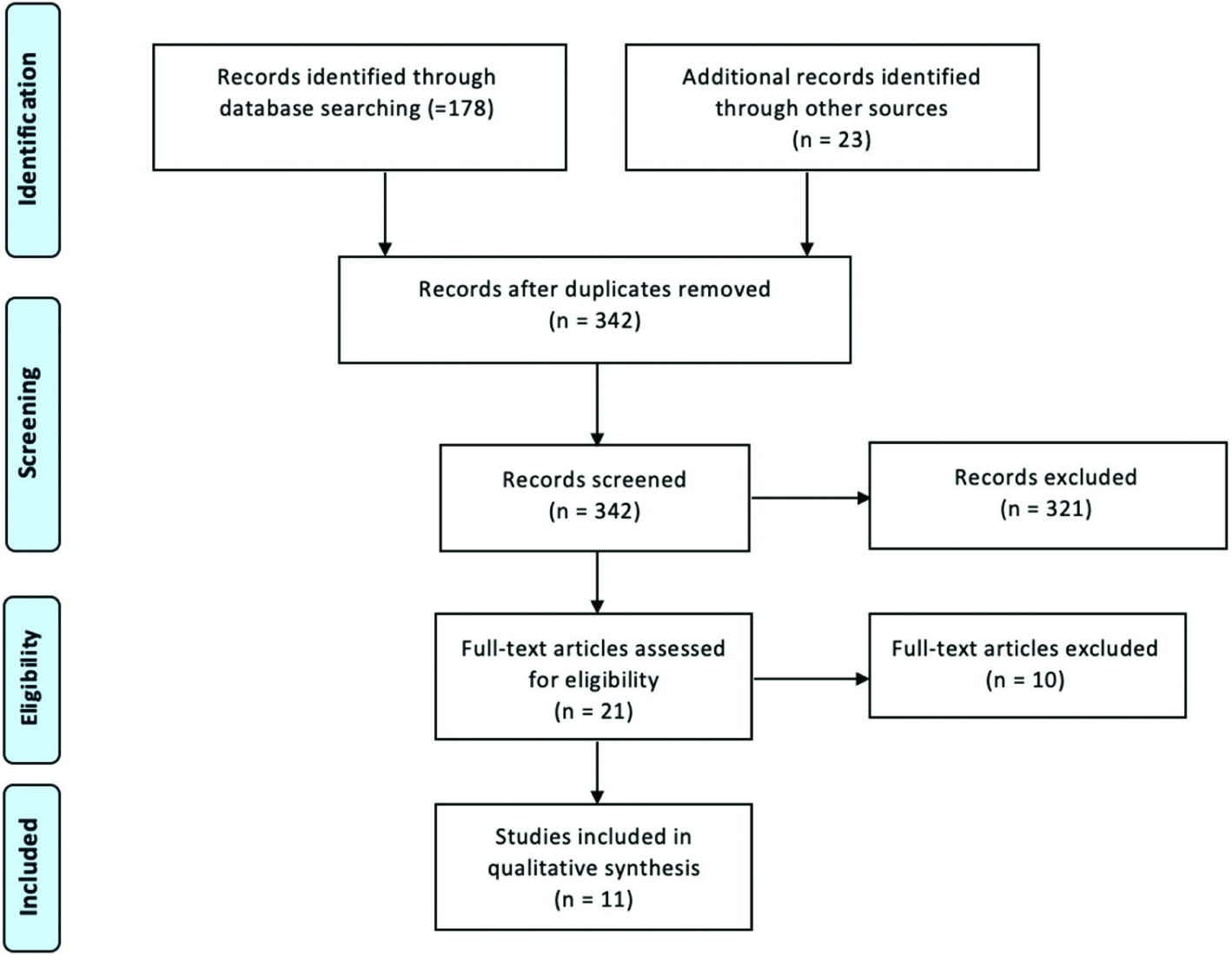
All papers were classified as level of evidence “IIIB.”
Indications for DC
Indications for initial DC included; arteriovenous malformations, ischemic or hemorrhagic stroke, infection, ruptured aneurysm, trauma (i.e., traumatic brain injury [TBI] alone – 3 studies),[
Pooled rate of hydrocephalus
The pooled rate of hydrocephalus for these 11 studies averaged 7.93% (n = 161/2029, with a range of 0.7–28.4%). The rate of postoperative hydrocephalus was not significantly different between the early (=96/1063; 9.03%) and late CP (=65/966; 6.72%) groups [
However, in three studies solely involving patients undergoing DC for TBI, there was a significantly lower incidence of hydrocephalus in the early CP patients (=11/152; 7,23%) versus late CP (=36/171; 21.05%) [
DISCUSSION
We utilized this meta-analysis to determine whether early CP decreased the rate of hydrocephalus following DC. Notably, we did not find any prospective, randomized, comparative studies to clearly answer this question.
Studies favoring early CP for DC to reduce incidence of hydrocephalus
In Xu et al. study in 2015, they reviewed three studies involving 312 patients that showed early CP following DC increased the risk of hydrocephalus.[
Rate of hydrocephalus requiring VP shunt after DC
In 2016, Malcom et al. observed in four studies their following DC that the pooled rate of hydrocephalus requiring a VP shunt was slightly lower (5.6%) than the rate in our study (7.93%).[
Why would early CP decrease rates of hydrocephalus?
Early CP may restore normal intracranial CSF pressure dynamics resulting in the spontaneous resolution of hydrocephalus and other CSF disturbances. On the contrary, delayed cranial reconstruction, by prolonging this disruption, may result in permanent dysfunction of the arachnoid granulations resulting in permanent hydrocephalus (e.g., such as the one seen in hydrocephalus induced by long- term CSF drainage).[
CONCLUSION
Early CP (within or equal to 90 days) after DC performed in TBI patients was associated with a lower incidence of hydrocephalus. However, this finding was not corroborated in other studies for patients undergoing DC attributed to other etiologies.
Ethical approval
All procedures performed in studies involving human participants were in accordance with in ethical standards.
Declaration of patient consent
Patient’s consent not required as there are no patients in this study.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Bender A, Heulin S, Röhrer S, Mehrkens JH, Heidecke V, Straube A. Early cranioplasty may improve outcome in neurological patients with decompressive craniectomy. Brain Inj. 2013. 27: 1073-9
2. Bjornson A, Tajsic T, Kolias AG, Wells A, Naushahi MJ, Anwar F. A case series of early and late cranioplasty-comparison of surgical outcomes. Acta Neurochir (Wien). 2019. 161: 467-72
3. Cho K, Park S. Safety and efficacy of early cranioplasty after decompressive craniectomy in traumatic brain injury patients. J Korean Neurotraumatol Soc. 2011. 7: 74-7
4. Goedemans T, Verbaan D, van der Veer O, Bot M, Post R, Hoogmoed J. Complications in cranioplasty after decompressive craniectomy: Timing of the intervention. J Neurol. 2020. p.
5. Hng D, Bhaskar MI, Khan FM, Budgeon C, Damodaran O, Knuckey N. Delayed cranioplasty: Outcomes using frozen autologous bone flaps. Craniomaxillofac Trauma Reconstr. 2015. 1: 190-7
6. Malcolm JG, Rindler RS, Chu JK, Grossberg JA, Pradilla G, Ahmad FU. Complications following cranioplasty and relationship to timing: A systematic review and meta-analysis. J Clin Neurosci. 2016. 33: 39-51
7. Morton RP, Abecassis IJ, Hanson JF, Barber JK, Chen M, Kelly CM. Timing of cranioplasty: A 10.75-year single-center analysis of 754 patients. J Neurosurg. 2018. 128: 1648-52
8. Nasi D, Dobran M, Iacoangeli M, Di Somma L, Gladi M, Scerrati M. Paradoxical brain herniation after decompressive craniectomy provoked by drainage of subdural hygroma. World Neurosurg. 2016. 91: 673.e1-4
9. Nasi D, Gladi M, Di Rienzo A, di Somma L, Moriconi E, Iacoangeli M. Risk factors for post-traumatic hydrocephalus following decompressive craniectomy. Acta Neurochir (Wien). 2018. 160: 1691-8
10. Piedra MP, Ragel BT, Dogan A, Coppa ND, Delashaw JB. Timing of cranioplasty after decompressive craniectomy for ischemic or hemorrhagic stroke. J Neurosurg. 2013. 118: 109-14
11. Piedra MP, Ragel BT, Dogan A, Coppa ND, Delashaw JB. Timing of cranioplasty after decompressive craniectomy for trauma. Surg Neurol Int. 2014. 25: 25-
12. Quah BL, Low HL, Wilson MH, Bimpis A, Nga VD, Lwin S. Is there an optimal time for performing cranioplasties? Results from a prospective multinational study. World Neurosurg. 2016. 94: 13-7
13. Tasiou A, Vagkopoulos K, Georgiadis I, Brotis AG, Gatos H, Fountas KN. Cranioplasty optimal timing in cases of decompressive craniectomy after severe head injury: A systematic literature review. Interdiscip Neurosurg. 2014. 1: 107-11
14. Walcott BP, Kwon CS, Sheth SA, Fehnel CR, Koffie RM, Asaad WF. Predictors of cranioplasty complications in stroke and trauma patients. J Neurosurg. 2013. 118: 757-62
15. Xu H, Niu C, Fu X, Ding W, Ling S, Jiang X. Early cranioplasty vs. Late cranioplasty for the treatment of cranial defect: A systematic review. Clin Neurol Neurosurg. 2015. 136: 33-40

