

- Department of Neurosurgery, Graduate School of Medicine and Pharmaceutical Sciences, University of Toyama, Toyama, Japan.
Correspondence Address:
Satoshi Kuroda, Department of Neurosurgery, Graduate School of Medicine and Pharmaceutical Sciences, University of Toyama, Toyama, Japan.
DOI:10.25259/SNI_659_2021
Copyright: © 2021 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Keitaro Shiraishi, Takahiro Tomita, Takuya Akai, Satoshi Kuroda. Cauda equina schwannoma presenting with subarachnoid and subdural hemorrhage: Its underlying mechanism. 13-Sep-2021;12:462
How to cite this URL: Keitaro Shiraishi, Takahiro Tomita, Takuya Akai, Satoshi Kuroda. Cauda equina schwannoma presenting with subarachnoid and subdural hemorrhage: Its underlying mechanism. 13-Sep-2021;12:462. Available from: https://surgicalneurologyint.com/surgicalint-articles/11109/
Date of Submission
01-Jul-2021
Date of Acceptance
26-Aug-2021
Date of Web Publication
13-Sep-2021
Abstract
Background: A patient presented with a spinal subarachnoid hemorrhage (SAH) and subdural hematoma (SDH) attributed to a spinal schwannoma at the T12-L1 level.
Case Description: A 67-year-old male acutely presented with severe back pain and L1 paraparesis/sensory loss, with urinary incontinence. CT/MR studies showed a spinal SAH and SDH within a likely T12-L1 schwannoma. At surgery, the hemorrhage within the tumor was continuous through the lower pole of the tumor into the subarachnoid and subdural spaces; tumor was dissected away from the surrounding tissues and totally removed. The postoperative course was uneventful, and the preoperative neurological deficits gradually resolved. Histopathologically, the lesion was a schwannoma with intratumoral hemorrhage.
Conclusion: This case demonstrates the rare acute presentation of a T12-L1 schwannoma with an accompanying intratumoral hemorrhage resulting in both a SDH/SAH.
Keywords: Cauda equina, Intratumoral hemorrhage, Mechanism, Spinal schwannoma, Subarachnoid hemorrhage
INTRODUCTION
Subarachnoid hemorrhage (SAH) originating from spinal lesions is rare, occurring in <1.5% of spinal tumors; they are typically spinal ependymomas or cavernous angiomas.[
Here, we present a hemorrhage into a T12-L1 schwannoma resulting in both a SAH and SDH.
CASE DESCRIPTION
A 67-year-old male on anticoagulants for atrial fibrillation, suddenly complained of severe back pain, an L1-level paraparesis/sensory loss with urinary incontinence. On examinations, he had 3/5 motor function loss from L1 downward and a partial sensory level to pin appreciation.
Radiological evaluation
The brain CT showed SAH clots in the posterior fossa. Cerebral angiography, however, showed no cranial vascular lesions. Notably, the lumbar MR demonstrated a T12-L1 lesion that was homogeneously enhanced with contrast consistent with a schwannoma [
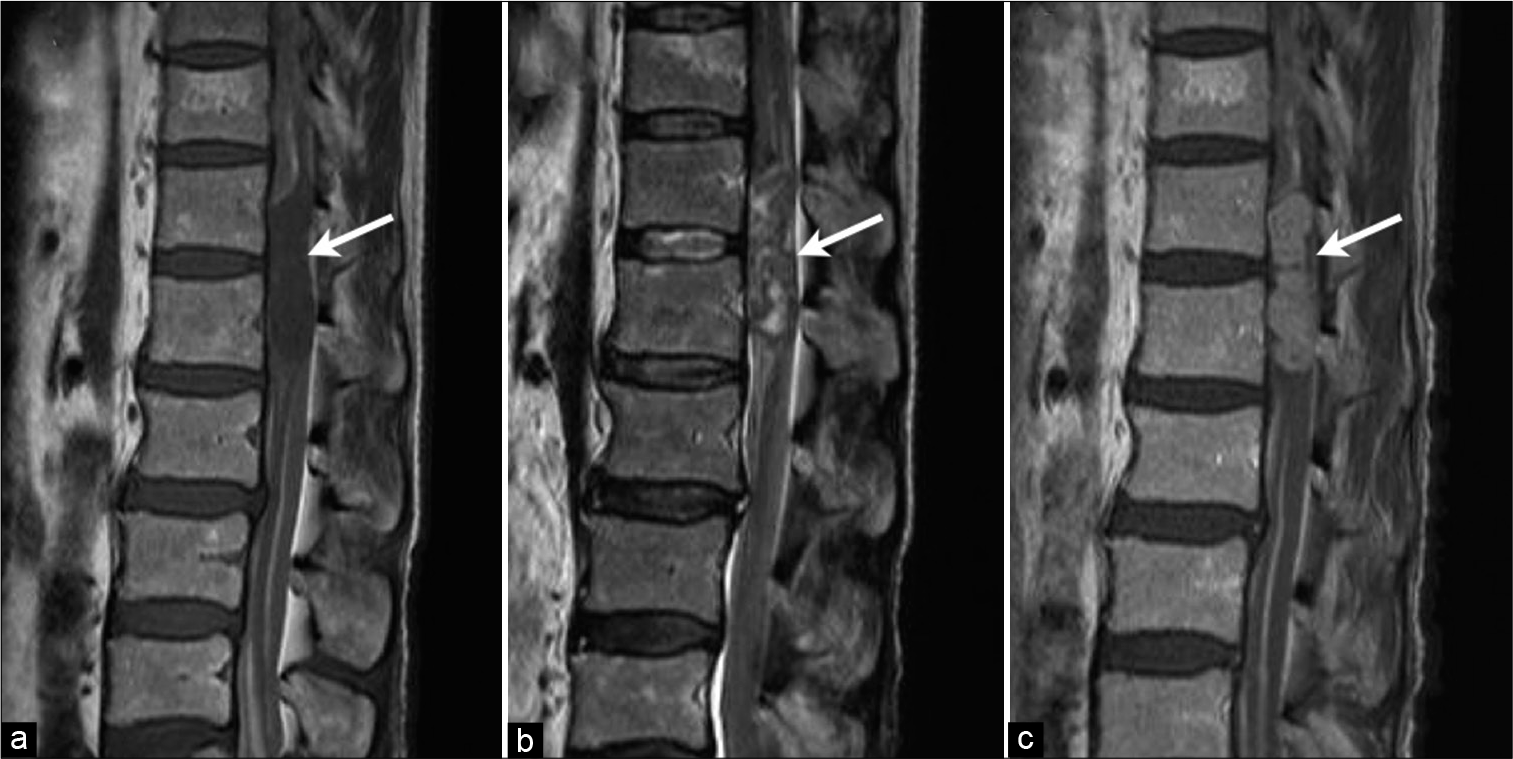
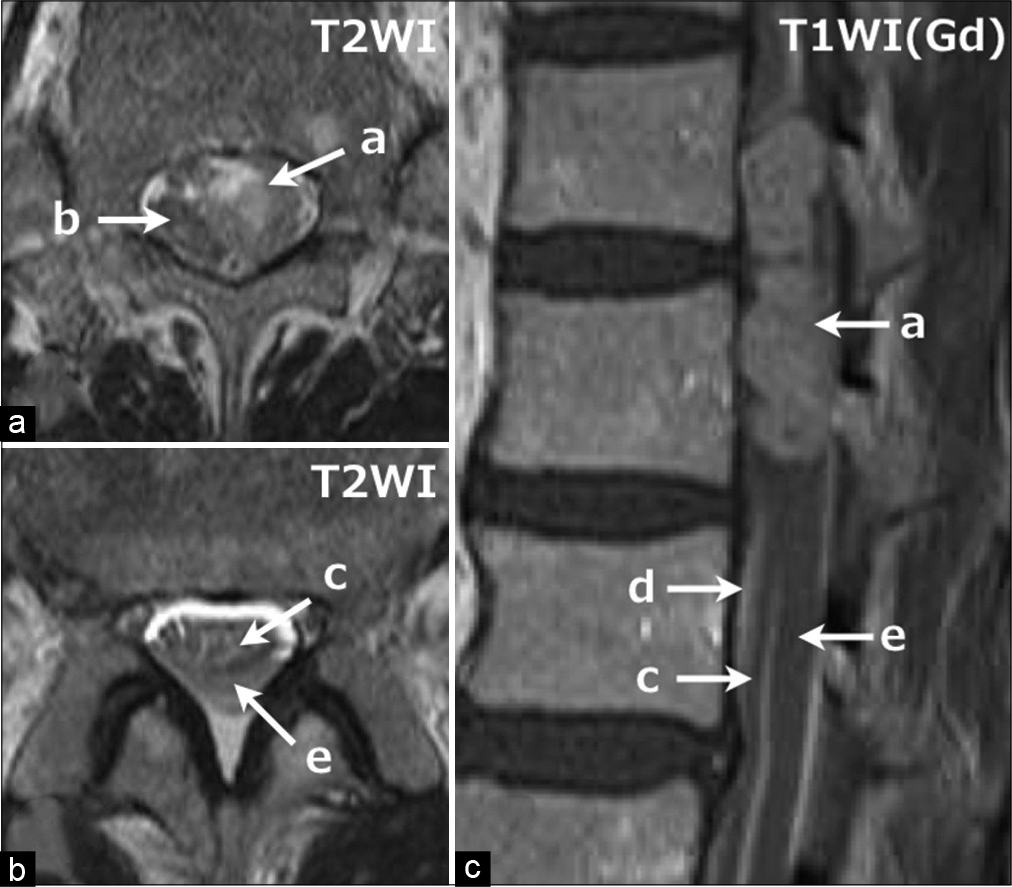
Figure 2:
Axial images of T2-weighted MRI at the level of L1 (a) and L2 (b), and sagittal image of Gd-enhanced T1-weighted MRI (c). The tumor mass (a) markedly compressed the conus medullaris (b) to the right side. The subarachnoid space around the cauda equina (c) just caudal to the tumor mass (a) is densely filled with clots (d), and there is a thick subdural hematoma (e) dorsal to the cauda equina.
Surgery
The patient underwent a T12-L2 laminectomy 3 weeks later using intraoperative sensory evoked potential (SEP) and motor evoked potential (MEP) [
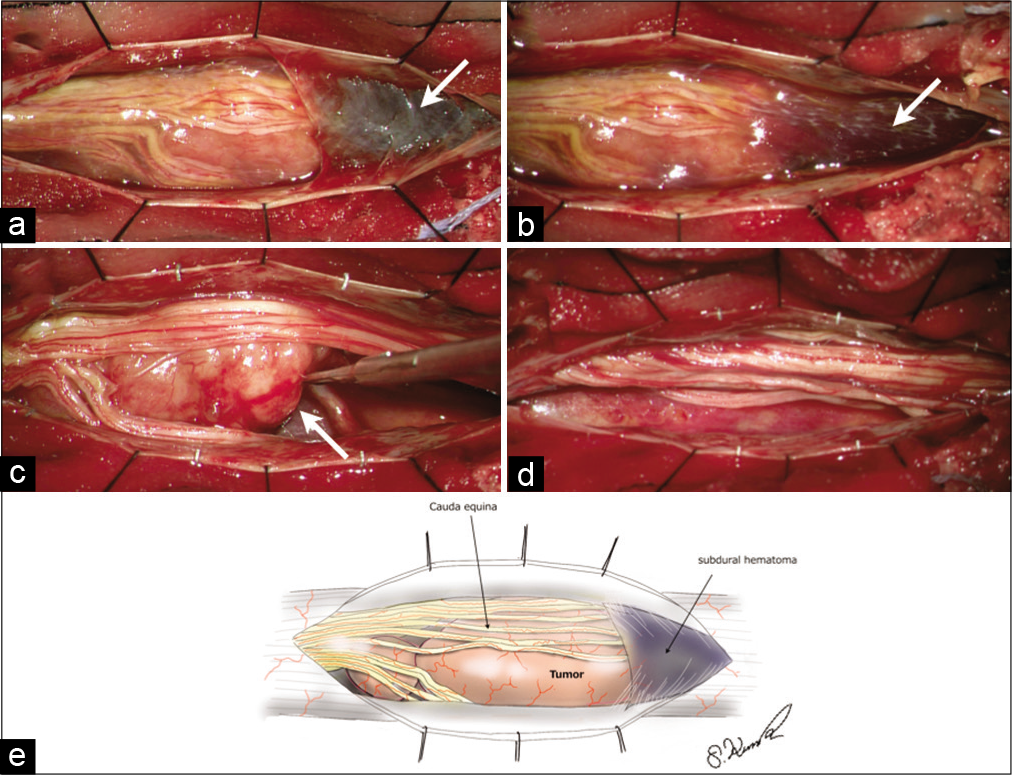
Figure 3:
Intraoperative findings (a-d) and illustration by the author (e). (a) When the dura was opened, the tumor was strongly compressing the surrounding cauda equina. Since 3 weeks had already passed since the onset, most of the clot in the subarachnoid space had been washed out. A thick subdural hematoma was present just caudal to the tumor (arrow). (b) When this subdural hematoma was removed, the arachnoid membrane, which had been compressed by the subdural hematoma, was found on its ventral side (arrow). (c) When the arachnoid was opened and the tumor was dissected from the surrounding cauda equina, bleeding from the lower pole of the tumor was found to have extended into the subarachnoid space (arrow). (d) The tumor was totally removed.
Pathology
The tumor was a typical schwannoma. It contained proliferating spindle cells arranged in short bundles or interlocking fascicles containing hypocellular and hypercellular area (Antoni A and B area, respectively). On immunohistochemistry, most of the tumor cells were positive for S-100 protein. Hyalinized and ectatic vessels were also found within the tumor close to the tumor capsule, with inflammatory cells clustered around them. Fresh hemorrhage associated with focal necrosis was also found within the tumor [
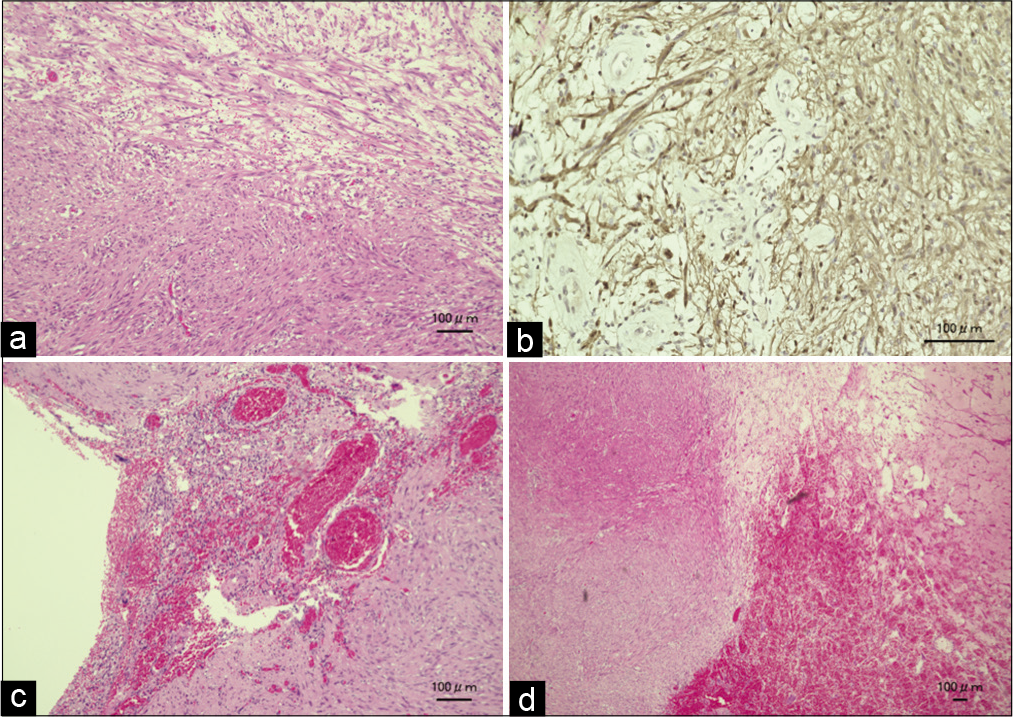
Figure 4:
Histopathological findings. (a) HE staining. Section of non-hemorrhagic lesion shows a cellular area consisting of elongated cells with Antoni A and B structures. (b) Immunohistochemistry reveals that most of tumor cells are positive for S-100. (c) HE staining. Section of hemorrhagic lesion demonstrates the enlarged, degenerated vessels in the tumor, which are surrounded by the inflammatory cells. (d) Section of hemorrhagic lesion shows fresh hemorrhage with typical Antoni A and B structures.
DISCUSSION
Spinal SAH occurs in only 0.05–1.5% of all spinal tumors. In addition to trauma, the most common causes of spinal SAH are spinal vascular lesions (i.e. saccular aneurysm of the spinal artery, spinal arteriovenous malformation, or fistula).[
As in the present case, SDHs often accompany SAH in patients with intratumoral hemorrhages into spinal schwannoma.[
The hyalinized enlarged vessels of spinal schwannomas may become occluded by thrombosis, resulting in intrinsic tumor necrosis and intratumoral hemorrhage. The histological examination also revealed the presence of numerous degenerated blood vessels in the tumor with inflammatory cells clustered around them, suggesting that disruption of the degenerated blood caused the intratumoral hemorrhage.
CONCLUSION
The present case demonstrates the rare acute presentation of a T12-L1 schwannoma with an accompanying intratumoral hemorrhage resulting in both a SDH/SAH.
Declaration of patient consent
Institutional Review Board (IRB) permission obtained for the study.
Financial support and sponsorship
None.
Conflicts of interest
There are no conflicts of interest.
Declaration of patient consent
Institutional Review Board (IRB) permission obtained for the study.
Financial support and sponsorship
None.
Conflicts of interest
There are no conflicts of interest.
References
1. Bennett SJ, Katzman GL, Mehta AS, Ali S. Hemorrhagic schwannoma presenting with subarachnoid hemorrhage and resulting cauda equina syndrome. Spine J. 2015. 15: e17-8
2. Cadieux M, Tso M, Fox S, Jacobs WB. Spontaneous spinal subarachnoid hemorrhage from a ruptured radiculopial artery aneurysm. World Neurosurg. 2021. 145: 114-8
3. Cervoni L, Franco C, Celli P, Fortuna A. Spinal tumors and subarachnoid hemorrhage: Pathogenetic and diagnostic aspects in 5 cases. Neurosurg Rev. 1995. 18: 159-62
4. Ciappetta P, D’Urso PI, Colamaria A. Giant craniovertebral junction hemorrhagic schwannoma: Case report. Neurosurgery. 2008. 62: E1166
5. Cordan T, Bekar A, Yaman O, Tolunay S. Spinal subarachnoid hemorrhage attributable to schwannoma of the cauda equina. Surg Neurol. 1999. 51: 373-5
6. de Divitiis E, Maiuri F, Corriero G, Donzelli R. Subarachnoid hemorrhage due to a spinal neurinoma. Surg Neurol. 1985. 24: 187-90
7. Kukreja S, Ambekar S, Sharma M, Nanda A. Cauda equina schwannoma presenting with intratumoral hemorrhage and intracranial subarachnoid hemorrhage. J Neurosurg Spine. 2014. 21: 357-60
8. Parmar H, Pang BC, Lim CC, Chng SM, Tan KK. Spinal schwannoma with acute subarachnoid hemorrhage: A diagnostic challenge. AJNR Am J Neuroradiol. 2004. 25: 846-50
9. van Gijn J, Kerr RS, Rinkel GJ. Subarachnoid haemorrhage. Lancet. 2007. 369: 306-18

