

- Department of Neurosurgery, All India Institute of Medical Sciences, Rishikesh, Uttarakhand, India,
- Department of Nursing, Akal College of Nursing, Eternal University, Baru Sahib, Himachal Pradesh, India,
- Department of Neuroanaesthesia, All India Institute of Medical Sciences, Rishikesh, Uttarakhand, India,
- Department of Anesthesia, All India Institute of Medical Sciences, Rishikesh, Uttarakhand, India,
- Department of Neurosurgery, All India Institute of Medical Sciences, Raipur, Chhattisgarh, India,
- Department of Nursing, All India Institute of Medical Sciences, Rishikesh, Uttarakhand, India,
- Department of Neurological Surgery, Mayo Clinic, Phoenix, Arizona, USA.
Correspondence Address:
Jitender Chaturvedi
Department of Neurological Surgery, Mayo Clinic, Phoenix, Arizona, USA.
DOI:10.25259/SNI_935_2020
Copyright: © 2021 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Jitender Chaturvedi1, Shiv Kumar Mudgal2, Tejas Venkataram1, Priyanka Gupta3, Nishant Goyal1, Gaurav Jain4, Anil Kumar Sharma5, Suresh Kumar Sharma6, Bernard R. Bendok7. Coma recovery scale: Key clinical tool ignored enough in disorders of consciousness. 08-Mar-2021;12:93
How to cite this URL: Jitender Chaturvedi1, Shiv Kumar Mudgal2, Tejas Venkataram1, Priyanka Gupta3, Nishant Goyal1, Gaurav Jain4, Anil Kumar Sharma5, Suresh Kumar Sharma6, Bernard R. Bendok7. Coma recovery scale: Key clinical tool ignored enough in disorders of consciousness. 08-Mar-2021;12:93. Available from: https://surgicalneurologyint.com/surgicalint-articles/10630/
Date of Submission
22-Dec-2020
Date of Acceptance
06-Feb-2021
Date of Web Publication
08-Mar-2021
Abstract
Background: Disorders of consciousness (DoC) includes coma, vegetative state (VS), minimally conscious state (MCS), and emergence from the MCS. Aneurysmal rupture with high-grade SAH, traumatic brain injury, and neoplastic brain lesions are some of the frequent pathologies leading to DoC. The diagnostic errors among these DoC are as high as ranging from 25% to 45%, with a probable error in the conclusion of patients’ state, treatment choice, end-of-life decision-making, and prognosis. Some studies also reported that 37–43% of patients were misdiagnosed in VS while demonstrating signs of awareness. Despite its wide acceptance, Coma Recovery Scale-Revised (CRS-r) remained underused or inappropriately utilized, which may lead to substandard or unprofessional patient care. Literature is rare on the knowledge of CRS-r among physicians published from India and across the globe. Therefore, we carried out the present study to ascertain physicians’ knowledge on CRS-r and raise awareness about its justifiable clinical utilization. We also explored the factors associated with this perceived level of experience among participants and recommend frequent physicians’ training for care of patients with DoC.
Methods: An institution-based cross-sectional online survey was conducted from June 8 to July 7, 2020, among Ninety-six physicians recruited using a convenient sampling technique. Twenty-item, validated, reliable, and a pilot-tested questionnaire was used to assess the knowledge regarding CRS-r and collect socio-demographic variables. The analysis was performed using the Statistical Package for the Social Sciences version 23. Bivariate and multivariate logistic regression analyses were employed to assess the association of participants’ socio-demographic variables and their parent department of work with the knowledge. P
Results: A total of Ninety-six participants were included in the analysis, and only 33.3% of them were found to have adequate knowledge of CRS-r. Multivariate analysis revealed that age (adjusted odds ratio [AOR] = 31.66; 95% CI: 6.25–160.36), gender (AOR = 44.16; 95% CI: 7.43–268.23), and parent department of working (AOR = 0.148; 95% CI: 0.06–0.39) were significantly associated with the knowledge.
Conclusion: Knowledge of the physicians on CRS-r is found to be exceptionally low. It has a strong tendency to adversely affect patients’ optimal care with disorders of consciousness (DoC). Therefore, it is crucial to expand physicians’ knowledge and awareness regarding CRS-r to adequately screen patients with DoC.
Keywords: Coma recovery scale-revised, Disorders of consciousness, Knowledge, Neurosurgery
INTRODUCTION
After severe craniocerebral insult secondary to various pathologies such as traumatic, vascular, or anoxic, a person may show a transformation through different phases of disorder of consciousness (DoC). These DoC include coma, vegetative state (VS), minimally conscious state (MCS), and emergence from the MCS (EMCS).[
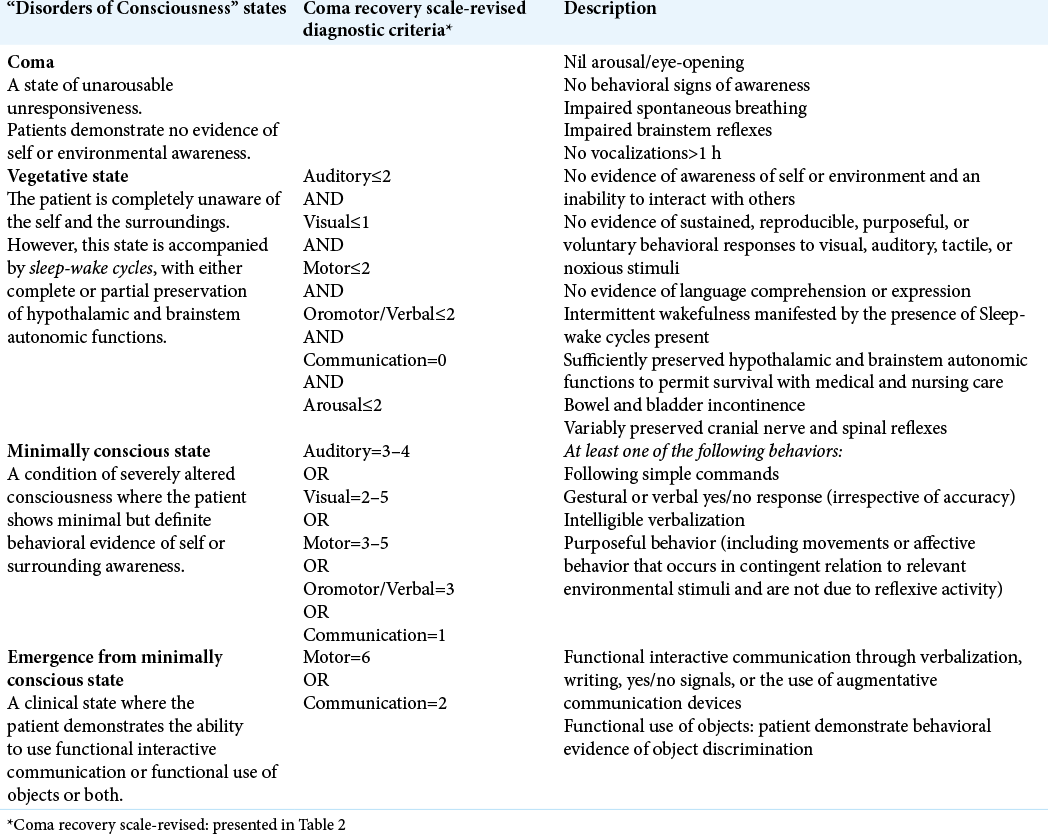
Survivors of craniocerebral insult may remain in coma for an uncertain period before progression into either VS or MCS. Promptly recognizing behavioral signs of awareness and making differentiation between coma, VS, and MCS is one of the most crucial and challenging work for physicians.[
Although essential, this task is either neglected in daily busy work in step-down wards, intensive care units (ICU), or physicians are often ignorant of differentiating these clinical responses. Differentiating between VS and MCS depends on the clinical assessment of patients’ responsiveness and the examiner’s knowledge and expertise. Most importantly, physicians and nurses taking care of the patient should know that such a system exists for their evaluation.[
Differentiating VS from MCS, neurobehavioral evaluation remains the gold standard and reliable for making a diagnosis. However, a neurobehavioral examination is critical due to the examiner, patient, and environmental biases presented in [
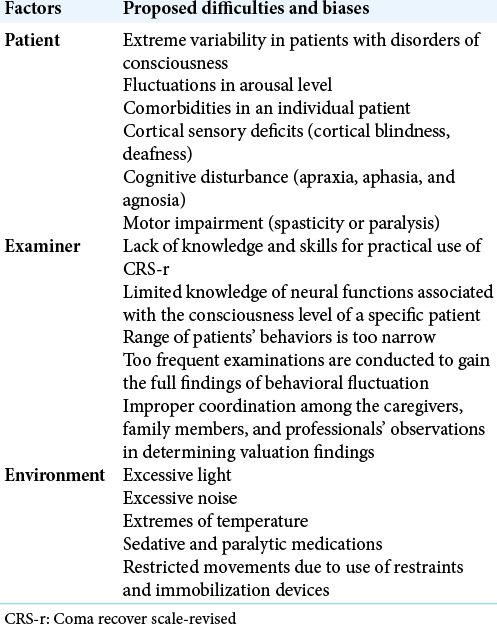
Moreover, it requires the clinical knowledge and expertise of physicians to use CSR-r effectively. Unfortunately, a high number of physicians steadily lose expertise with this scale after their professional training is over. The inadequate knowledge about this scale’s clinical application could negatively impact the optimal care of patients with DoC.[
Despite its wide acceptance, it remained underused or inappropriately utilized, leading to substandard or unprofessional patient care. Literature is rare on the knowledge of CRS-r among physicians published from India, and indeed South-East Asia or any other Low and Middle-Income Countries (LMIC). Therefore, we carried out the present study to ascertain the level of physicians’ knowledge of CRS-r. We also explored the factors associated with this perceived level of experience among participants.
MATERIALS AND METHODS
Setting and period
This institution-based, single-centric cross-sectional online survey was conducted from June to July 2020 at a tertiary care teaching hospital in North India to ascertain physicians’ knowledge on CSR-r and factors associated with this level of expertise among participants. This online survey was carried out using Google forms, and the first phase of this online survey was from June 8 to June 18, 2020, while follow-up was done from June 28 to July 7, 2020. The survey required nearly 12–15 min for completion.
Study population
A total of 96 physicians in the Department of General Medicine, Neurology or Neurosurgery (Neurosciences as a combined specialty), Emergency Medicine, and ICU/Critical care were recruited. All physicians who were willing to participate were included in the present study.
Sampling procedure
We could not find any study, previously published from any center in our country. The sample size was determined using the formula n/1 + ne2, where the total population of physicians in these departments was 110, assuming a 5% margin of error, and 95% confidence level.[
Ethical considerations
Ethical approval was obtained from the Institutional Ethical Committee (IEC: AIIMS/IEC/20/216 April 20, 2020). We obtained electronic informed written consent from each study participant. Confidentiality was assured by anonymized their name and department. The purpose of this study was well informed to all participants.
Data collection and instruments
Data were collected using an online structured questionnaire with two sections, Section A consisted of seven items related to socio-demographic inclusion regarding study and use of CRS-r information, while section B consisted of twenty items related to exact knowledge on CRS-r. The correct response was assigned a score of one, and the wrong one, zero. The questionnaire had a maximum score of twenty, and participants who earned a cutoff point of ten and above were considered to have adequate knowledge. The reliability of the questionnaire was estimated among twenty participants. The internal consistency of the tool was demonstrated during this study by Cronbach’s alpha (α = 0.82).
Data analysis
We used Epi-data version 3.1 for data cleaning and coding, then transferred to Statistical Package for the Social Sciences version 23. Descriptive statistics (frequencies, percentages, means, and standard deviations) were used to explore the data. For the statistical analysis, the level of knowledge was categorized into “adequate” and “inadequate” based on 50% scores. We did a two-stage logistic regression analysis to identify the association of participants’ socio-demographic variables with their knowledge level. In the first step, the binary logistic regression was employed to identify independent variables for knowledge. We further included the variables associated with P ≤ 0.25 in bivariate analysis for multivariate analysis. Extraneous variables were explored by comparing the crude odds ratio and the Adjusted Odds Ratio (AOR). All significant tests were two-tailed, and variables with P < 0.05 at the multivariate analysis were considered statistically significant.
RESULTS
A total of hundred participants were recruited, and ninety-six participated with a response rate of 96%. Of the ninety-six physicians who participated in the study, fifty-six (58.3%) were <35-years-old, and forty (41.7%) were >35-years-old. A total of sixty (62.5%) were male, and forty-eight (50%) of the participants were postgraduate. The working department’s proportion was slightly different, forty-four (45.8%) and fifty-two (54.2%) worked in neurosciences and other departments, respectively. Approximately two-thirds, i.e. sixty-four (66.7%) of the participants had more than five years of experience working in their core department. Regarding knowledge acquired (studied) about CRS-r during their training, and subsequent clinical use of CSR-r during their practice, sixty-four (66.7%) and eighty (83.3%) of the participants responded “no,” respectively [

We found that thirty-two (33.3%) participants had adequate knowledge of CRS-r, and the total mean ± standard deviation of their knowledge score was 7.58 ± 5.25. Bivariate logistic regression analysis showed that age, gender, educational level, department of work, and entire years of experience were associated with their knowledge [
The study revealed that participants younger than 35 years had significantly higher odds of having adequate knowledge, approximately 32 times, when compared to those who were older than 35 years of age. Male participants were 44.16 times more likely to have sufficient expertise than female participants (95% confidence interval [CI] 7.43–268.23). Besides, compared to physicians working in the neuroscience departments, the odds of having adequate knowledge decreased among physicians working in other departments (AOR 0.148; 95% CI 0.06–0.39) [
DISCUSSION
The CRS-r is widely considered to be the most sensitive neurobehavioral scale to differentiate between disorders of consciousness.[
Despite the emergence of other advanced techniques to differentiate between states of consciousness, such as functional neuroimaging, event-related potentials, or electroencephalographic testing, their validity is not yet proven. Their feasibility in the clinical setting is questionable.[
The misdiagnosis rates of coma recovery are substantially high across numerous reports in the literature, ranging between 15% and 43%.[
CRS-r is recommended as a measure to decrease the chances of misdiagnosis, given its ability to differentiate between VS, MCS, and EMCS. Given the unacceptable costs of a misdiagnosis of DoCs, several recommendations exist to adapt the scale for the most significant reduction in misdiagnosis rates. Considering the fluctuations in consciousness levels,[
The importance of CRS-r cannot be understated – not only is it a valuable diagnostic tool to differentiate between VS, MCS, and EMCS, but it also determines the prognosis, subsequent rehabilitation, and end-of-life choices for patients and their families, thus bearing ethical implications.[
Thus, given the value, the scale adds to the clinical setting. It is required to be administered multiple times. It is understandable why the miscalculation of CRS-r can be a costly affair. In our study, analyzing the level of physicians’ knowledge of CRS-r in a tertiary care teaching hospital, we found that only a small proportion of respondents possessed an “adequate” understanding of the scale. This can have grave consequences for the patient and risks posing a burden on the already strained health-care system, more so in LMIC.
While there are no studies assessing physician familiarity with CRS-r for us to compare our findings with, studies on GCS knowledge among physicians exist, identifying a similar gap in awareness. A survey of 90 military physicians (nearly half of which were residents) by Riechers et al. found a somewhat disconcerting finding – of those physicians who had completed ATLS training (87% of the total respondents), only 15% were able to recall all aspects of the GCS correctly. None of the physicians who had not taken ATLS were able to describe the GCS accurately. Their results were also specialty-dependent, with those trained in neurosurgery and general surgery performing better than physicians from other specialties.[
We found that age was a significant determinant of CRS-r awareness, with younger age groups recording higher scores on the questionnaire, which can be explained by their training’s relative regency. Similarly, male respondents recorded higher scores on the questionnaire. While there is no sex-specific explanation for the difference in awareness levels, we believe this could be because of the skewed sex-ratios existent in different departments, with departments like neurosurgery, which fared better, being predominantly male.
Nearly two-thirds of participants had not acquired CRS-r knowledge in training, which necessitates more prominence for it. We also recommend frequent crash courses and refresher training programs, considering that older age groups did not fare as well and that 50% of those who reportedly used it in practice had inadequate knowledge, pointing to the volatility of the content. These training programs can also be catered to specific specialties depending on their baseline knowledge.
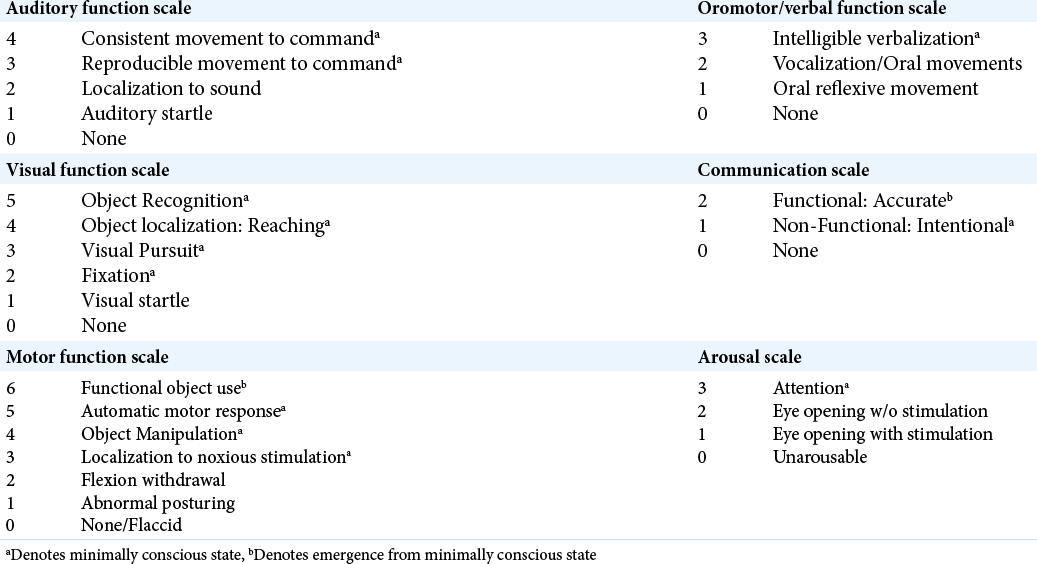
Further, more than 80% of participants reportedly did not use the scale in practice. However, they were not necessarily unaware of the scale’s use and adoption (24/32 patients who had adequate knowledge reported that they did not use it). This indicates barriers to usage other than a lack of awareness, such as scarcity of time and perhaps, a perceived lack of relevance. This needs to be tackled as well. A study by Wannez et al. demonstrated that limiting the CRS-r assessment to the five most frequently observed items (i.e., fixation, visual pursuit, a reproducible movement to command, automatic motor response, and localization to noxious stimulation) detected 99% of the patients in MCS.[
To the best of our knowledge, this is the first study to assess the levels of expertise of CRS-r among practicing doctors. Our analysis also had a few other strengths, such as using a well-validated and reliable questionnaire. We also incorporated a broad range of relevant specialties and anonymized our survey, which avoided response bias. The use of convenience sampling, we suspect, is a limitation because of generalizability.
The present study’s findings suggest that health-care professionals should be encouraged to use CRS-r for neurobehavioral assessment of patients with DoC. Regular re-learning and refresher lectures of this valuable clinical tool will go a long way in ensuring a reasonably correct evaluation of patients’ DoC status evaluated by the tool. Furthermore, regular CME programs beyond the medical school should be a compulsory prerequisite for renewing the health-care professionals’ practicing license. Senior professors and team leaders should encourage their teams to clinical usage of this scale in day-to-day bedside clinical rounds.
CONCLUSION
We found that only a small proportion of medical practitioners involved in the direct care of patients with DoC possessed adequate knowledge of the CRS-r. Close to one-third of physician participants had sufficient knowledge and skills for practical application of CRS-r. Participant’s age, gender, and parent department are directly and strongly correlated to the extent of knowledge and applicability of CRS-r. Given its vital importance in clinical practice, we propose that it is sensible to follow a two-pronged strategy, comprising “improved training” and “frequent incorporation into the daily routine” to avoid the perils of misdiagnosing DoC.
Declaration of patient consent
Institutional Review Board permission obtained for the study.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Adeleye AO, Owolabi MO, Rabiu TB, Orimadegun AE. Physicians’ knowledge of the Glasgow coma scale in a Nigerian University Hospital: Is the simple GCS still too complex?. Front Neurol. 2012. 3: 28
2. Seel RT, Sherer M, Whyte J. Assessment scales for disorders of consciousness: Evidence-based recommendations for clinical practice and research. Arch Phys Med Rehabil. 2010. 91: 1795-813
3. Andrews K, Murphy L, Munday R, Littlewood C. Misdiagnosis of the vegetative state: Retrospective study in a rehabilitation unit. BMJ. 1996. 313: 13-6
4. Annen J, Filippini MM, Bonin E, Cassol H, Aubinet C, Carrière M. Diagnostic accuracy of the CRS-R index in patients with disorders of consciousness. Brain Inj. 2019. 33: 1409-12
5. Bodien YG, Carlowicz CA, Chatelle C, Giacino JT. Sensitivity and specificity of the coma recovery scale-revised total score in detection of conscious awareness. Arch Phys Med Rehabil. 2016. 97: 490-2
6. Chatelle C, Bodien Y, Carlowicz C, Wannez S, CharlandVerville V, Gosseries O. Detection and interpretation of impossible and improbable coma recovery scale-revised scores. Arch Phys Med Rehabil. 2016. 97: 300-e4
7. Childs NL, Mercer WN, Childs HW. Accuracy of diagnosis of persistent vegetative state. Neurology. 1993. 43: 1465-7
8. Cortese M, Riganello F, Arcuri F, Pugliese M, Lucca L, Dolce G. Coma recovery scale-r: Variability in the disorder of consciousness. BMC Neurol. 2015. 15: 186
9. Gerrard P, Zafonte R, Giacino JT. Coma recovery scale-revised: Evidentiary support for hierarchical grading of level of consciousness. Arch Phys Med Rehabil. 2014. 95: 2335-41
10. Giacino J, Ashwal S, Childs N, Cranford R, Jennett B, Katz DI. The minimally conscious state: Definition and diagnostic criteria. Neurology. 2002. 58: 349-53
11. Giacino JT, Schnakers C, Rodriguez-Moreno D, Kalmar K, Schiff N, Hirsch J. Behavioral assessment in patients with disorders of consciousness: Gold standard or fool’s gold?. Prog Brain Res. 2009. 177: 33-48
12. Mudgal SK. Assess learning needs of nursing students and effectiveness of workshop on knowledge regarding extended and expanded role of nurses. Int J Nurs Educ. 2018. 10: 109-13
13. Pignat JM, Mauron E, Jöhr J, Gilart de Keranflec’h C, van de Ville D, Preti MG. Outcome prediction of consciousness disorders in the acute stage based on a complementary motor behavioural tool. PLoS One. 2016. 11: e0156882
14. Pistoia F, Carolei A, Bodien Y, Greenfield S, Kaplan S, Sacco S. The comorbidities coma scale (CoCoS): Psychometric properties and clinical usefulness in patients with disorders of consciousness. Front Neurol. 2019. 10: 1042
15. Portaccio E, Morrocchesi A, Romoli AM, Hakiki B, Taglioli MP, Lippi E. Score on coma recovery scale-revised at admission predicts outcome at discharge in intensive rehabilitation after severe brain injury. Brain Inj. 2018. 32: 730-4
16. Portaccio E, Morrocchesi A, Romoli AM, Hakiki B, Taglioli MP, Lippi E. Improvement on the coma recovery scale-revised during the first four weeks of hospital stay predicts outcome at discharge in intensive rehabilitation after severe brain injury. Arch Phys Med Rehabil. 2018. 99: 914-9
17. Riechers RG, Ramage A, Brown W, Kalehua A, Rhee P, Ecklund JM. Physician knowledge of the Glasgow coma scale. J Neurotrauma. 2005. 22: 1327-34
18. Schnakers C, Giacino J, Kalmar K, Piret S, Lopez E, Boly M. Does the FOUR score correctly diagnose the vegetative and minimally conscious states?. Ann Neurol. 2006. 60: 744-55
19. Schnakers C, Vanhaudenhuyse A, Giacino J, Ventura M, Boly M, Majerus S. Diagnostic accuracy of the vegetative and minimally conscious state: Clinical consensus versus standardized neurobehavioral assessment. BMC Neurol. 2009. 21: 35-42
20. Sharma SK, Mudgal SK, Thakur K, Gaur R. How to calculate sample size for observational and experimental nursing research studies?. Natl J Physiol Pharm Pharmacol. 2020. 10: 1-8
21. The Multi-Society Task Force on PVS. Medical aspects of the persistent vegetative state 1. N Engl J Med. 1994. 330: 1499-508
22. Wannez S, Gosseries O, Azzolini D, Martial C, Cassol H, Aubinet C. Prevalence of coma-recovery scale-revised signs of consciousness in patients in minimally conscious state. Neuropsychol Rehabil. 2018. 28: 1350-9
23. Wannez S, Heine L, Thonnard M, Gosseries O, Laureys S. Coma Science Group Collaborators. The repetition of behavioral assessments in diagnosis of disorders of consciousness. Ann Neurol. 2017. 81: 883-9

