

- Department of Neurosurgery, Osaka University Hospital, Suita, Japan.
- Department of Neurosurgery, Hanwa Memorial Hospital, Osaka, Japan.
Correspondence Address:
Koshi Ninomiya, Department of Neurosurgery, Osaka University Hospital, Suita, Japan.
DOI:10.25259/SNI_129_2024
Copyright: © 2024 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Kowashi Taki1, Koshi Ninomiya1, Akihiro Yamamoto1, Takuya Suematsu1, Manabu Sasaki2, Haruhiko Kishima1. Communicating hydrocephalus after resection of a meningioma ventral to the foramen magnum. 05-Jul-2024;15:231
How to cite this URL: Kowashi Taki1, Koshi Ninomiya1, Akihiro Yamamoto1, Takuya Suematsu1, Manabu Sasaki2, Haruhiko Kishima1. Communicating hydrocephalus after resection of a meningioma ventral to the foramen magnum. 05-Jul-2024;15:231. Available from: https://surgicalneurologyint.com/surgicalint-articles/12978/
Date of Submission
21-Feb-2024
Date of Acceptance
17-Jun-2024
Date of Web Publication
05-Jul-2024
Abstract
Background: Tumors in or near the foramen magnum may cause communicating or non-communicating hydrocephalus (HC), depending on their size and location. Here, an 81-year-old female developed communicating HC following the resection of a meningioma ventral to the foramen magnum.
Case Description: An 81-year-old female presented with numbness in the left neck and left hemiparesis. The magnetic resonance revealed an 18-mm tumor ventral to the foramen magnum that significantly enlarged over the past 6 months. She underwent total tumor resection but then presented with progressive HC both clinically (i.e., instability of gait with confusion) and radiographically (computed tomography). Following placement of a lumboperitoneal (LP) shunt, symptoms markedly improved. Further, the cerebrospinal fluid (CSF) analysis showed elevated cell counts and protein concentrations, indicating likely “leakage” of intratumoral contents postoperatively contributing to the progressive HC.
Conclusion: Patients presenting with acute meningiomas ventral to the foramen magnum may develop postoperative communicating HC attributed to tumor-related CSF leakage of necrotic intratumoral components that can be successfully treated with a LP shunt.
Keywords: Cerebrospinal fluid malabsorption, Foramen magnum meningioma, Lumbar peritoneal shunt, Postoperative hydrocephalus, Tumor resection
INTRODUCTION
Depending on their size and location, tumors arising in/near the foramen magnum can cause communicating or non-communicating hydrocephalus (HC). This is largely attributed to tumoral leakage of necrotic components (i.e., elevated protein) into the cerebrospinal fluid (CSF). Here, an 81-year-old female, 2 weeks following gross total resection of a foramen magnum meningioma, developed acute communicating HC successfully treated with a lumboperitoneal (LP) shunt.
CASE DESCRIPTION
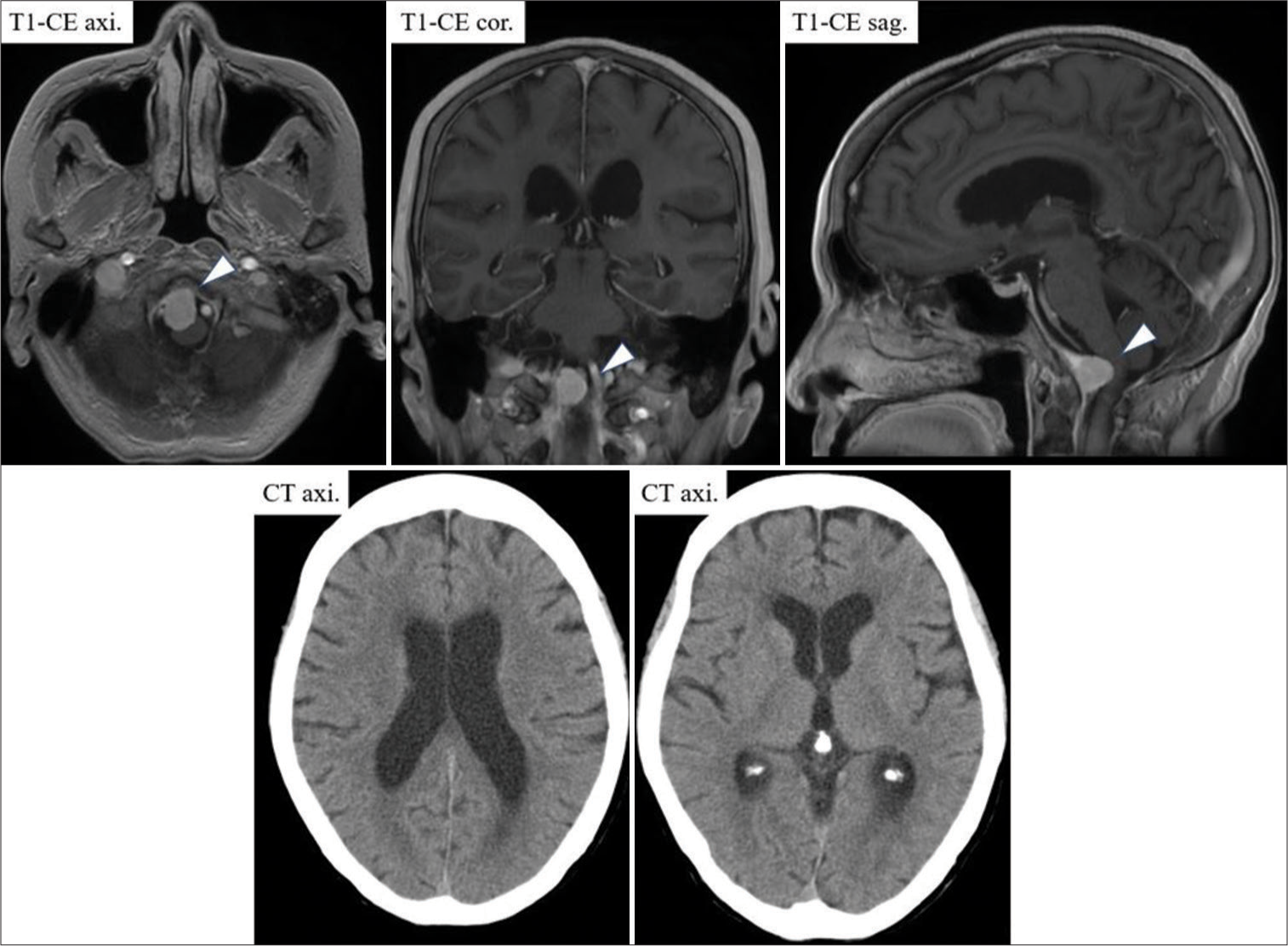
An 81-year-old female presented with 6 months of dizziness and numbness in the left neck/body and 2 weeks of acute left hemiparesis. The brain magnetic resonance (MR) showed an 18-mm tumor located anterolaterally to the right of the foramen magnum that had enlarged over the past 6 months; there was no accompanying HC [

Surgery
In the right park-bench position, hemisection of C1 and partial osteotomy of the right foramen magnum and right condylar fossa were performed. A dural entry point clearly separated from the right vertebral artery was identified. The tumor was exposed once the dura and dentate ligament were incised, along with retraction of the posterior root of C1 [
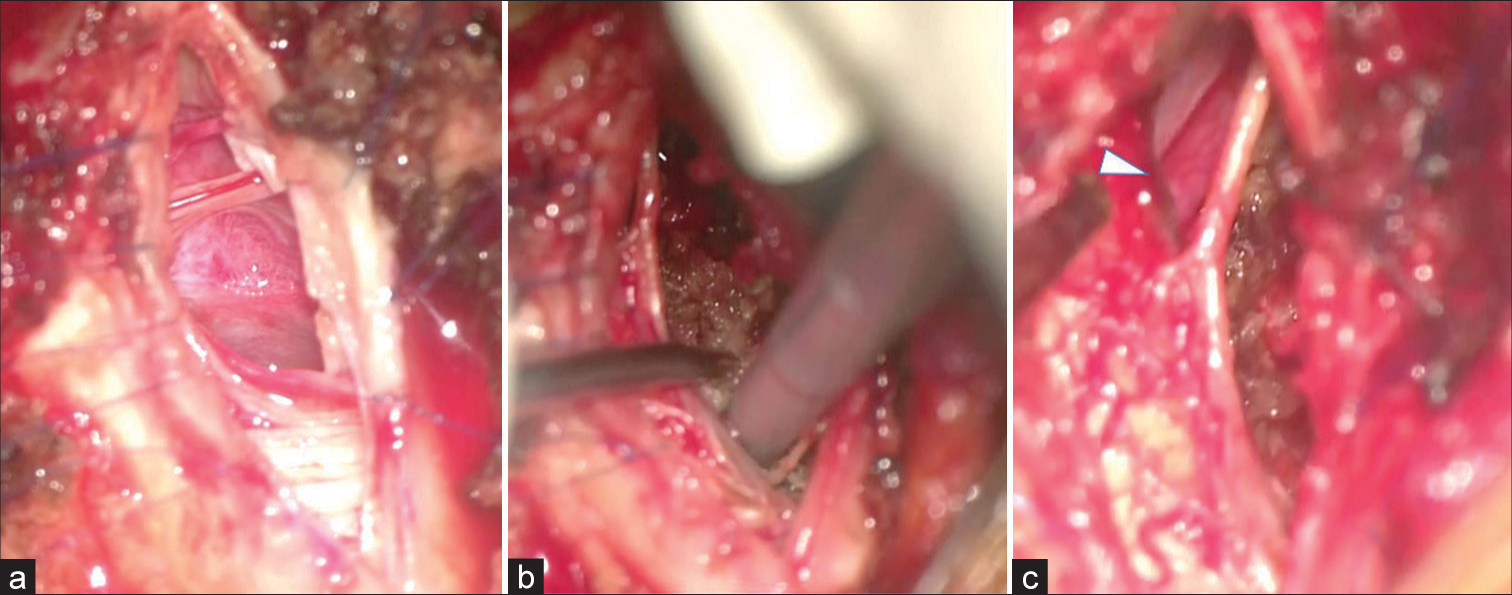
Figure 3:
(a) The right-sided dura was incised, the dentate ligament and the posterior root of C1 were cut, and the tumor was exposed. (b) The tumor was carefully fragmented and completely removed by ultrasonic aspiration. (c) The tumor was completely removed, and the contralateral vertebral artery was identified (arrowhead).
Postoperative course
Three days later, the patient only had a mild residual right lower extremity paresis and the repeat MR confirmed complete tumor removal [

Figure 4:
(a) Spinal magnetic resonance imaging showed complete tumor removal, and computed tomography (CT) showed no hydrocephalus (HC) (Evans index: 0.30). (b) CT showed the appearance of HC (Evans index: 0.36). (c) After lumboperitoneal shunt procedure, CT showed improvement in HC (Evans index: 0.32).
DISCUSSION
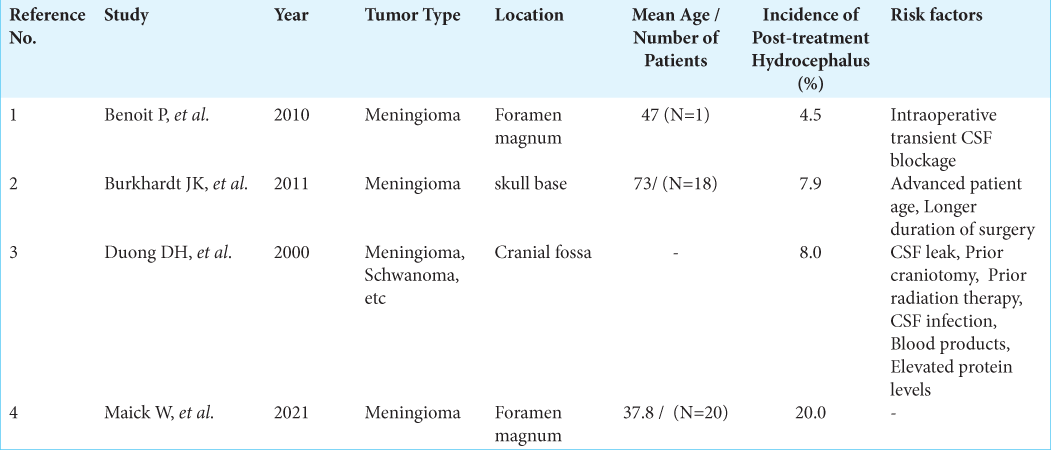
The incidence of HC following resection of foramen magnum meningiomas ranges from 4.5% to 20%.[
CONCLUSION
Following resection of a foramen magnum meningioma, patients may acutely develop communicating HC attributed to high CSF protein levels/tumor debris, subsequently requiring placement of LP shunts.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Journal or its management. The information contained in this article should not be considered to be medical advice; patients should consult their own physicians for advice as to their specific medical needs.
References
1. Benoit P, Jacques B, Olivier D. Management of anterolateral foramen magnum meningiomas: Surgical vs. conservative decision making. Oper Neurosurg. 2010. 67: ons58-70
2. Burkhardt JK, Zinn PO, Graenicher M, Santillan A, Bozinov O, Kasper EM. Predicting postoperative hydrocephalus in 227 patients with skull base meningioma. Neurosurg Focus. 2011. 30: E9
3. Duong DH, O’Malley S, Sekhar LN, Wright DG. Postoperative hydrocephalus in cranial base surgery. Skull Base Surg. 2000. 10: 197-200
4. Maick W, Paulo H, Giovanna Z, Pedro H, Paulo E, Marcos V. Foramen magnum meningioma: Series of 20 cases. Complications, risk factors for relapse, and follow-up. J Craniovertebler Junction Spine. 2021. 12: 406-11

