

- Department of Neurosurgery, University of Louisville, Louisville, Kentucky.
DOI:10.25259/SNI_599_2019
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Zaid Aljuboori, Mayur Sharma, Norberto Andaluz. Contemporaneous avulsion fractures of the inferior clivus and bilateral occipital condyles with injury of the tectorial membrane. 17-Jan-2020;11:11
How to cite this URL: Zaid Aljuboori, Mayur Sharma, Norberto Andaluz. Contemporaneous avulsion fractures of the inferior clivus and bilateral occipital condyles with injury of the tectorial membrane. 17-Jan-2020;11:11. Available from: https://surgicalneurologyint.com/surgicalint-articles/9841/
Date of Submission
27-Dec-2019
Date of Acceptance
07-Jan-2020
Date of Web Publication
17-Jan-2020
Abstract
Background: Craniocervical junction (CCJ) injuries are highly variable, and there are only limited data to suggest their optimal treatment. Here, we present a rare case of concomitant bilateral occipital condyle fractures with an inferior clival avulsion fracture with concomitant focal injury of the tectorial membrane.
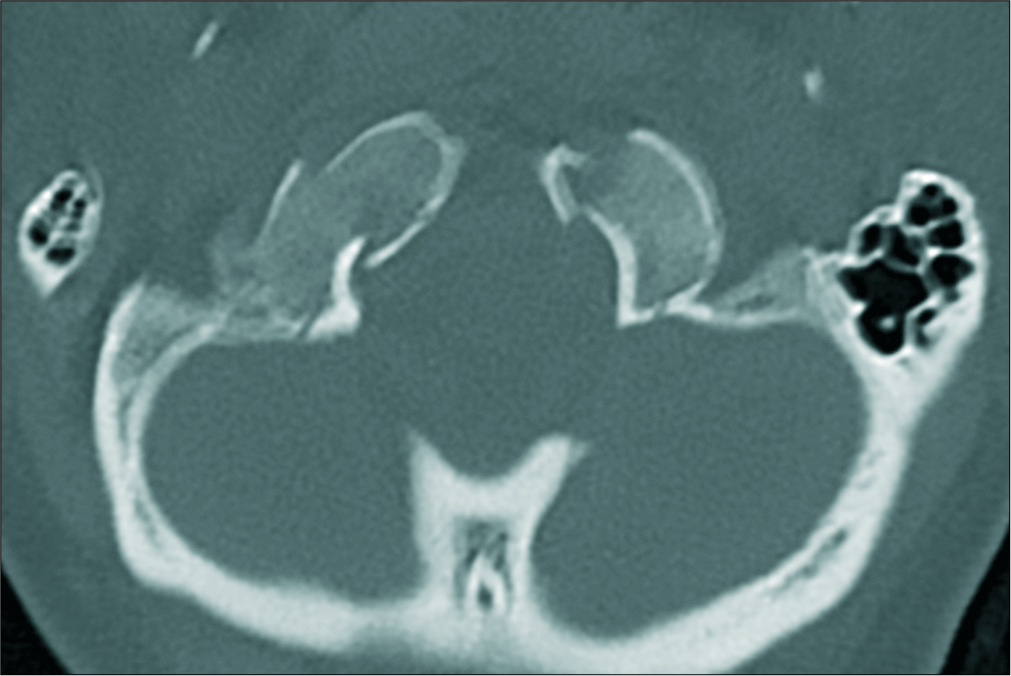
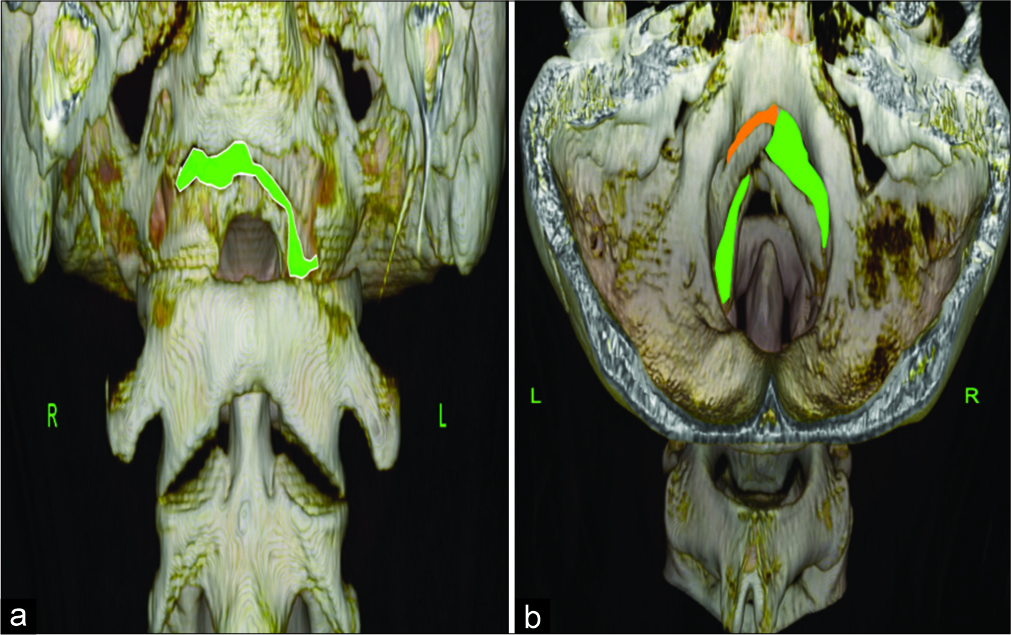
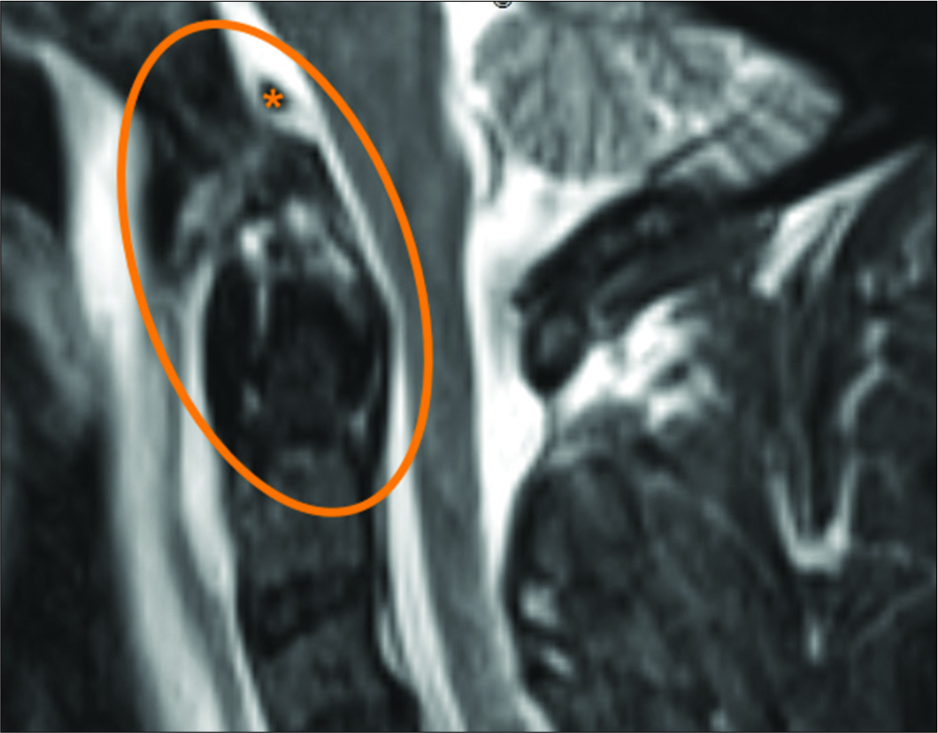
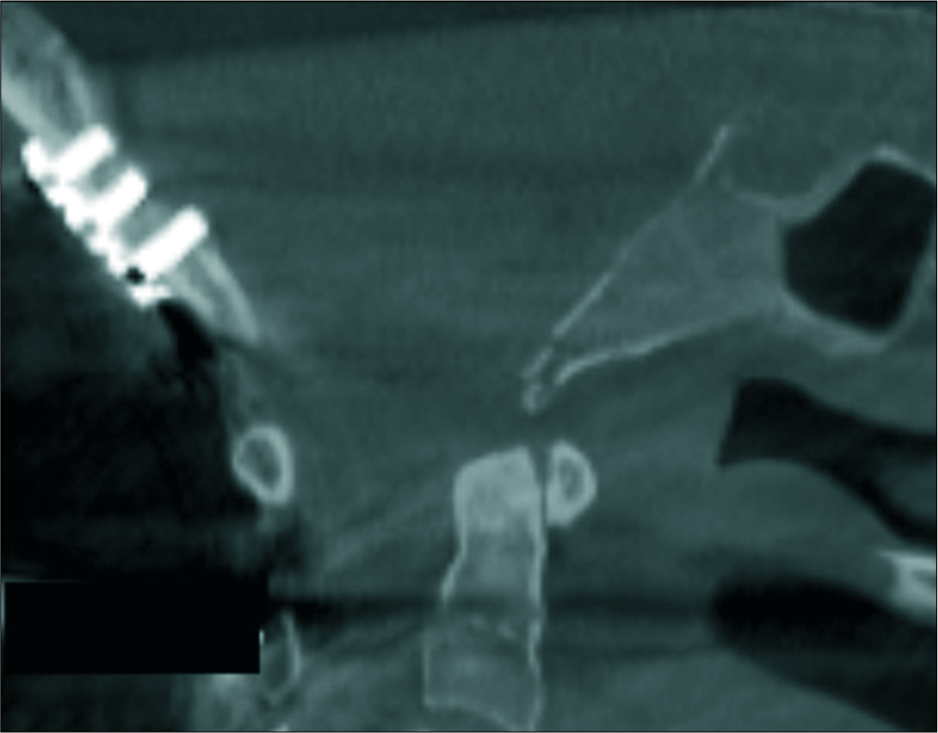
Case Description: Following a motor vehicle accident, a 51-year-old female sustained multiple orthopedic and soft tissue injuries. The cervical computed tomography (CT) showed a bilateral occipital condyle avulsion fractures with an avulsion of the inferior clivus. The cervical magnetic resonance imaging additionally demonstrated focal injury to the tectorial membrane with edema of both atlanto-occipital joints. Although the patient was neurologically intact, the CCJ instability warranted an emergent occiput-C2 (O-C2) posterior instrumented arthrodesis using the modular (multiple piece) occipitocervical (OC) plates/rods. The surgery was uneventful, and the patient remained neurologically intact. The 3-month follow-up cervical X-ray demonstrated continued stability/bony fusion.
Conclusion: Bilateral condyle fractures with a concomitant inferior clivus fracture are rare, and there is no known optimal strategy. Here, in an intact patient, instability of the CCJ warranted an O-C2 fusion.
Keywords: Clivus, Fracture, Fusion, Ligaments, Occipital condyle, Trauma
INTRODUCTION
Unilateral or bilateral fractures of the occipital condyles with or without the involvement of the inferior clivus are uncommon and are challenging to treat.[
Here, we present a case of contemporaneous avulsion fractures of the inferior clivus and bilateral occipital condyles with focal tectorial membrane injury successfully treated with occipitocervical occiput-C2 (O-C2) fusion.
CASE REPORT
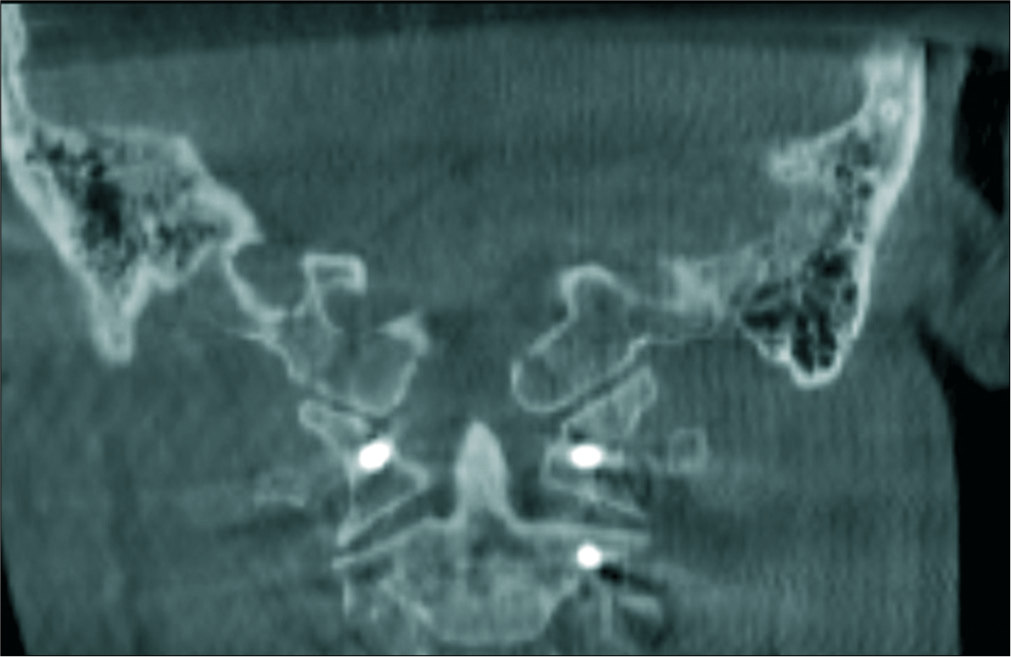
Following a motor vehicle accident, a 51-year-old female who presented neurologically intact with cervical magnetic resonance/computed tomography (CT) documented bilateral avulsion fractures of the occipital condyles (type III) and fracture of the inferior clivus [


DISCUSSION
The CCJ has multiple ligaments that provide support and stability.[
Radiological analysis
Isolated fractures with/without ligamentous injury can lead to instability of the CCJ and subsequently devastating vascular and/or neurologic complications. To assess both components, it is important to obtain an initial cervical CT and CT angiogram followed by a cervical MRI. Of note, 72 h after an injury, the tissue edema decreases, and ligamentous injury can be missed on MRI.[
Surgical considerations
There are not enough data to guide the selection between surgical and nonsurgical treatment for these injuries. Maughan et al.[
CONCLUSION
Bilateral occipital condyle fractures with inferior clivus fractures are rare, and there is no definitive treatment algorithm for these simultaneous lesions. Here, our patient with these multiple injuries and CCJ instability warranted an O-C2 fusion.
Declaration of patient consent
A patient consent was not obtained as this case report is retrospective in nature with no identifying information patient consent is not needed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Anderson PA, Montesano PX. Morphology and treatment of occipital condyle fractures. Spine (Phila Pa 1976). 1988. 13: 731-6
2. Dashti R, Ulu MO, Albayram S, Aydin S, Ulusoy L, Hanci M. Concomitant fracture of bilateral occipital condyle and inferior clivus: What is the mechanism of injury?. Eur Spine J. 2007. 16: 261-4
3. Evers JJ, Vieth VV, Hartensuer RR, Raschke MM, Vordemvenne TT. Management of an extended clivus fracture: A case report. BMC Res Notes. 2013. 6: 554-
4. Jones DN, Knox AM, Sage MR. Traumatic avulsion fracture of the occipital condyles and clivus with associated unilateral atlantooccipital distraction. AJNR Am J Neuroradiol. 1990. 11: 1181-3
5. Krüger A, Oberkircher L, Frangen T, Ruchholtz S, Kühne C, Junge A. Fractures of the occipital condyle clinical spectrum and course in eight patients. J Craniovertebr Junction Spine. 2013. 4: 49-55
6. Lopez AJ, Scheer JK, Leibl KE, Smith ZA, Dlouhy BJ, Dahdaleh NS. Anatomy and biomechanics of the craniovertebral junction. Neurosurg Focus. 2015. 38: E2-
7. Maughan PH, Horn EM, Theodore N, Feiz-Erfan I, Sonntag VK. Avulsion fracture of the foramen magnum treated with occiput-to-c1 fusion: Technical case report. Neurosurgery. 2005. 57: E600-
8. Steinmetz MP, Mroz TE, Benzel EC. Craniovertebral junction: Biomechanical considerations. Neurosurgery. 2010. 66: 7-12
9. Tanabe M, Watanabe T, Matsumoto S, Okamoto H, Shirakashi K. Avulsion fracture of the anterior half of the foramen magnum involving the bilateral occipital condyles and the inferior clivus--case report. Neurol Med Chir (Tokyo). 1999. 39: 358-61
10. Tubbs RS, Grabb P, Spooner A, Wilson W, Oakes WJ. The apical ligament: Anatomy and functional significance. J Neurosurg. 2000. 92: 197-200
11. Tubbs RS, Kelly DR, Humphrey ER, Chua GD, Shoja MM, Salter EG. The tectorial membrane: Anatomical, biomechanical, and histological analysis. Clin Anat. 2007. 20: 382-6
12. Vaicys C, Hunt CD. An unstable circumferential skull base fracture. J Trauma. 2001. 51: 577-8


