

- Department of Neurosurgery, Helsinki University Hospital, Helsinki, Finland, USA
- Department of Neurosurgery, Loyola University Medical Center, Maywood, IL, USA
- Department of Neuroradiology, Helsinki University Hospital, Helsinki, Finland, USA
Correspondence Address:
Tarik F. Ibrahim
Department of Neurosurgery, Helsinki University Hospital, Helsinki, Finland, USA
DOI:10.4103/2152-7806.168074
Copyright: © 2015 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Ibrahim TF, Hafez A, Andrade-Barazarte H, Raj R, Niemela M, Lehto H, Numminen J, Jarvelainen J, Hernesniemi J. De novo giant A2 aneurysm following anterior communicating artery occlusion. Surg Neurol Int 23-Oct-2015;6:
How to cite this URL: Ibrahim TF, Hafez A, Andrade-Barazarte H, Raj R, Niemela M, Lehto H, Numminen J, Jarvelainen J, Hernesniemi J. De novo giant A2 aneurysm following anterior communicating artery occlusion. Surg Neurol Int 23-Oct-2015;6:. Available from: http://surgicalneurologyint.com/surgicalint_articles/de-novo-giant-a2-aneurysm-following-anterior-communicating/
Abstract
Background:De novo intracranial aneurysms are reported to occur with varying incidence after intracranial aneurysm treatment. They are purported to be observed, however, with increased incidence after Hunterian ligation; particularly in cases of carotid artery occlusion for giant or complex aneurysms deemed unclippable.
Case Description:We report a case of right-sided de novo giant A2 aneurysm 6 years after an anterior communicating artery (ACoA) aneurysm clipping. We believe this de novo aneurysm developed in part due to patient-specific risk factors but also a significant change in cerebral hemodynamics. The ACoA became occluded after surgery that likely altered the cerebral hemodynamics and contributed to the de novo aneurysm. We believe this to be the first reported case of a giant de novo aneurysm in this location. Following parent vessel occlusion (mostly of the carotid artery), there are no reports of any de novo aneurysms in the pericallosal arteries let alone a giant one. The patient had a dominant right A1 and the sudden increase in A2 blood flow likely resulted in increased wall shear stress, particularly in the medial wall of the A2 where the aneurysm occurred 2 mm distal to the A1-2 junction.
Conclusion:ACoA preservation is a key element of aneurysm surgery in this location. Suspected occlusion of this vessel may warrant closer radiographic follow-up in patients with other risk factors for aneurysm development.
Keywords: A2, aneurysm, anterior communicating, de novo, giant, occlusion
INTRODUCTION
Since Graf and Hamby first coined the phrase “de novo” aneurysm, in 1964,[
Many postcarotid occlusion DNIAs are small when discovered and typically occur at the anterior communicating artery (ACoA), posterior communicating artery (PCoA), internal carotid artery (ICA)-bifurcation, and basilar bifurcation.[
CASE REPORT
Initial presentation and surgery
A 46-year-old female was incidentally found to have an ACoA aneurysm during screening conducted because her mother and maternal uncle both suffered subarachnoid hemorrhage (SAH). Of note, her mother's SAH was due to giant MCA aneurysm. The patient smoked tobacco daily and was normotensive. She had no other medical illnesses. A computed tomography angiogram (CTA) uncovered a 3 mm ACoA aneurysm facing posteriorly with the dome directed to the left [
Postoperative course and discovery of de novo intracranial aneurysms
The patient's last CTA prior to the discovery of her DNIA was 10 months after surgery at which time there was no new or recurrent aneurysm. She lost to follow-up after this, until 2014, when she presented to the neurosurgery clinic complaining of subjective memory issues. She was neurologically intact. The patient reported that she continued smoking following the initial surgery. A new CTA revealed a 2.5 cm × 3.7 cm × 3.0 cm largely thrombosed, partially calcified DNIA based off of the medial wall of the right pericallosal artery [
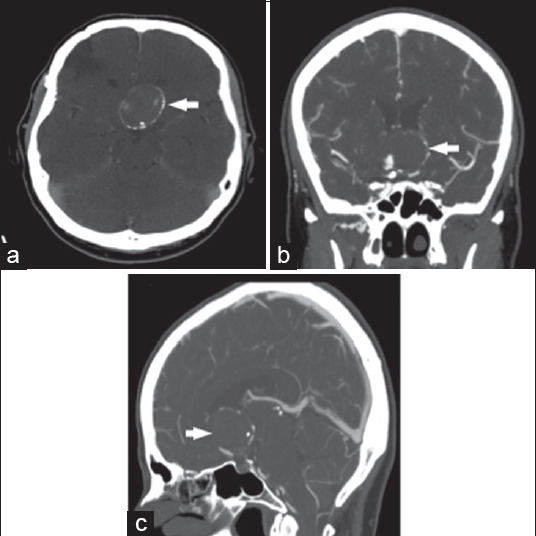
Figure 3
Computed tomography angiogram 6 years following the initial anterior communicating artery aneurysm clipping shows the 2.5 cm × 3.7 cm × 3.0 cm giant aneurysm (white arrows). There is calcification and thrombus evident on axial (a), coronal (b) and sagittal (c) cuts. There is some filling of the aneurysm from the right A2 seen on the coronal view

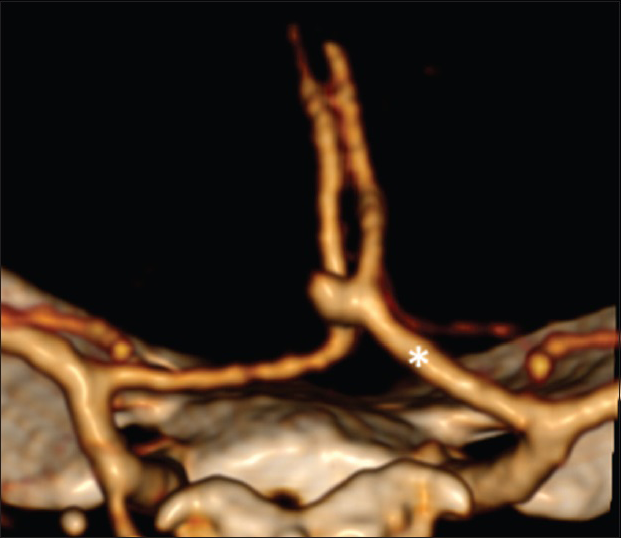
Figure 4
Digital subtraction angiogram viewed from an anterior-oblique angle. The aneurysm is based on the medial wall of the right A2 approximately 2 mm distal to the A1-A1 junction. The anterior communicating artery, patent at the initial surgery, does not fill at all now. The aneurysm clip (red arrow) is seen in the region the anterior communicating artery aneurysm and artery to be used
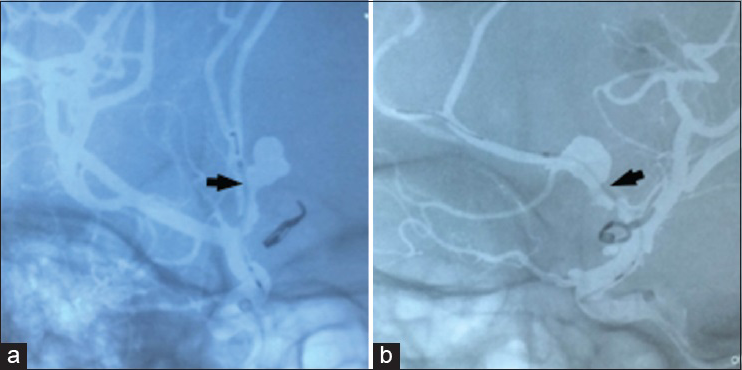
Figure 5
Digital subtraction angiogram (a and b) during Pipeline Embolization Device deployment. The microcatheter can be seen traversing the right internal carotid artery, right A1 and terminating in the distal right A2. Black arrows indicate where it crosses the aneurysm base. There was stagnation noted within the aneurysm immediately following Pipeline Embolization Device placement
The patient was neurologically intact after the procedure. There were no complications. She currently reports that her memory issues are unchanged. She was discharged home on Aspirin and Plavix.
DISCUSSION
We present the first case of a giant DACA DNIA. This aneurysm was felt to be de novo as opposed to recurrent or secondary to dissection for several reasons. The neck small remnant of the ACoA aneurysms (ACoAA) was based on the ACoA itself. It was coagulated with bipolar electrocautery as originally described by Yasargil[
All DACA aneurysms (distal to the ACoA) are rare and comprise only 2–9% of all -[
The development of DNIAs is thought to be multifactorial and include many of the risk factors that lead to the initial aneurysm. Women and smokers have been shown to be at increased risk.[
The interval between initial aneurysm treatment and DNIA development is also debatable. Some authors report DNIA detection over 18 years from the initial aneurysm treatment.[
We felt that this patient's ACoA aneurysm was appropriately excluded and did not require any further follow-up after her 1-year appointment. She may however, represent a small subset of high-risk patients that despite a low incidence of DNIAs in most aneurysm patients could be considered for close follow-up. This patient in particular was prone to DNIA formation as she is female, a smoker, and has a family history of SAH.
The location of this DNIA is unique. Increased hemodynamic stress within the cerebral circulation, particularly following Hunterian ligation, has been reportedly associated with a significant increase in the rate of DNIA formation.[

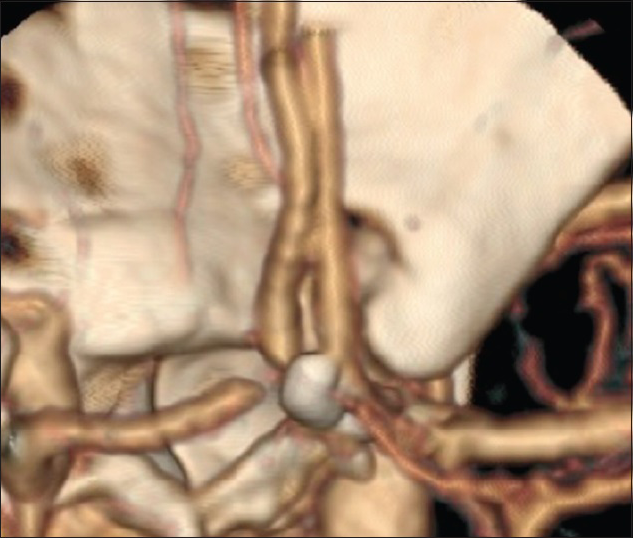
Figure 6
Digital subtraction angiogram showing the branching angle between the right A1 and A2 vessels. The anatomy within the red circle (a) is enlarged on the right (b). The observed angle as measured by Ingebrigtsen et al.[
Lending further to the impact of hemodynamics is the observed angle between the A1 and A2 arteries. Ingebrigtsen et al.[
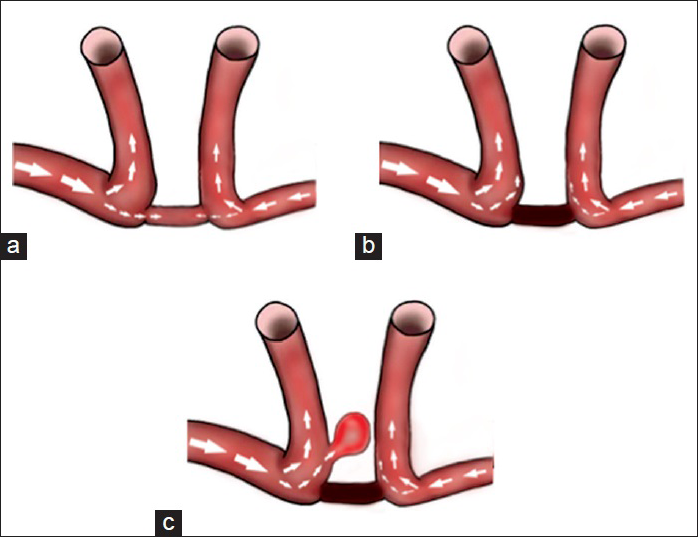
Figure 7
Characterization of blood flow patterns in the anterior cerebral artery/anterior communicating artery complex. The thickness of the arrows indicates amount of flow. A patent anterior communicating artery (a) would distribute the flow from the dominant right A1 such that some would flow into the anterior communicating artery (hence the leftward directed aneurysm) and some would flow into the A2. Once the anterior communicating artery is occluded (b), all of the flow from the A1 is directed into the A2. This eventually contributes to aneurysm formation (c)
The treatment of complex, giant aneurysms of the pericallosal region can be challenging. Open microsurgical techniques include direct clipping, trapping with bypass, or distal occlusion with bypass. A bypass for this type of aneurysm would likely be A3-to-A3. PEDs are typically used for complex and giant cavernous or intradural ICA aneurysms proximal to the PCoA but further indications are being explored. Puri et al. recently published a small experience using PEDs in distal aneurysms including 2 in the pericallosal region.[
CONCLUSION
We report a novel case of a giant A2 DNIA. While this patient had multiple risk factors for DNIA development, the location of her de novo aneurysm just distal to the occluded ACoA suggests that the altered hemodynamics played a significant role in development of her giant aneurysm. PED indications are expanding but they are associated with complications and their long-term outcomes are not known. ACoA preservation is a key element of microsurgical treatment of aneurysm in this location. The ACoA likely became occluded due to a combination of manipulation, clip application, and excessive bipolar cautery. Patients in whom the ACoA is suspected of occlusion after aneurysm surgery should be considered for closer radiographic follow-up; especially if they possess other risk factors for aneurysm development.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Arambepola PK, McEvoy SD, Bulsara KR. De novo aneurysm formation after carotid artery occlusion for cerebral aneurysms. Skull Base. 2010. 20: 405-8
2. Biondi A, Jean B, Vivas E, Le Jean L, Boch AL, Chiras J. Giant and large peripheral cerebral aneurysms: Etiopathologic considerations, endovascular treatment, and long-term follow-up. AJNR Am J Neuroradiol. 2006. 27: 1685-92
3. Bor AS, Rinkel GJ, Adami J, Koffijberg H, Ekbom A, Buskens E. Risk of subarachnoid haemorrhage according to number of affected relatives: A population based case-control study. Brain. 2008. 131: 2662-5
4. Bruneau M, Rynkowski M, Smida-Rynkowska K, Brotchi J, De Witte O, Lubicz B. Long-term follow-up survey reveals a high yield, up to 30% of patients presenting newly detected aneurysms more than 10 years after ruptured intracranial aneurysms clipping. Neurosurg Rev. 2011. 34: 485-96
5. Chalouhi N, Tjoumakaris SI, Gonzalez LF, Hasan D, Pema PJ, Gould G. Spontaneous delayed migration/shortening of the pipeline embolization device: Report of 5 cases. AJNR Am J Neuroradiol. 2013. 34: 2326-30
6. Crompton MR. Mechanism of growth and rupture in cerebral berry aneurysms. Br Med J. 1966. 1: 1138-42
7. Crompton MR. The pathogenesis of cerebral aneurysms. Brain. 1966. 89: 797-814
8. David CA, Vishteh AG, Spetzler RF, Lemole M, Lawton MT, Partovi S. Late angiographic follow-up review of surgically treated aneurysms. J Neurosurg. 1999. 91: 396-401
9. de Sousa AA, Dantas FL, de Cardoso GT, Costa BS. Distal anterior cerebral artery aneurysms. Surg Neurol. 1999. 52: 128-35
10. Dinc C, Iplikcioglu AC, Bikmaz K. Distal anterior cerebral artery aneurysms: Report of 26 cases. Neurol Med Chir (Tokyo). 2006. 46: 575-80
11. Doenitz C, Schebesch KM, Zoephel R, Brawanski A. A mechanism for the rapid development of intracranial aneurysms: A case study. Neurosurgery. 2010. 67: 1213-21
12. Fargen KM, Velat GJ, Lawson MF, Mocco J, Hoh BL. Review of reported complications associated with the pipeline embolization device. World Neurosurg. 2012. 77: 403-4
13. Farias JP, Trindade AM. Giant distal anterior cerebral artery aneurysm not visualized on angiography: Case report. Surg Neurol. 1997. 48: 348-51
14. Ferns SP, Sprengers ME, van Rooij WJ, van den Berg R, Velthuis BK, de Kort GA. De novo aneurysm formation and growth of untreated aneurysms: A 5-year MRA follow-up in a large cohort of patients with coiled aneurysms and review of the literature. Stroke. 2011. 42: 313-8
15. Fiorella D, Hsu D, Woo HH, Tarr RW, Nelson PK. Very late thrombosis of a pipeline embolization device construct: Case report. Neurosurgery. 2010. 67: onsE313-4
16. Gao L, Hoi Y, Swartz DD, Kolega J, Siddiqui A, Meng H. Nascent aneurysm formation at the basilar terminus induced by hemodynamics. Stroke. 2008. 39: 2085-90
17. Graf CJ, Hamby WB. Report of a case of cerebral aneurysm in an adult developing apparently de novo. J Neurol Neurosurg Psychiatry. 1964. 27: 153-6
18. Ha SK, Lim DJ, Kim SD, Kim SH. Rupture of de novo anterior communicating artery aneurysm 8 days after the clipping of ruptured middle cerebral artery aneurysm. J Korean Neurosurg Soc. 2013. 54: 236-8
19. Hampton T, Walsh D, Tolias C, Fiorella D. Mural destabilization after aneurysm treatment with a flow-diverting device: A report of two cases. J Neurointerv Surg. 2011. 3: 167-71
20. Hashizume K, Nukui H, Horikoshi T, Kaneko M, Fukamachi A. Giant aneurysm of the azygos anterior cerebral artery associated with acute subdural hematoma – Case report. Neurol Med Chir (Tokyo). 1992. 32: 693-7
21. Hayashi M, Kobayashi H, Kawano H, Handa Y, Kabuto M. Giant aneurysm of an azygos anterior cerebral artery: Report of two cases and review of the literature. Neurosurgery. 1985. 17: 341-4
22. Hernesniemi J, Tapaninaho A, Vapalahti M, Niskanen M, Kari A, Luukkonen M. Saccular aneurysms of the distal anterior cerebral artery and its branches. Neurosurgery. 1992. 31: 994-8
23. Inci S, Erbengi A, Ozgen T. Aneurysms of the distal anterior cerebral artery: Report of 14 cases and a review of the literature. Surg Neurol. 1998. 50: 130-9
24. Ingebrigtsen T, Morgan MK, Faulder K, Ingebrigtsen L, Sparr T, Schirmer H. Bifurcation geometry and the presence of cerebral artery aneurysms. J Neurosurg. 2004. 101: 108-13
25. Juvela S, Poussa K, Porras M. Factors affecting formation and growth of intracranial aneurysms: A long-term follow-up study. Stroke. 2001. 32: 485-91
26. Kanemoto Y, Tanaka Y, Nonaka M, Hironaka Y. Giant aneurysm of the azygos anterior cerebral artery – Case report. Neurol Med Chir (Tokyo). 2000. 40: 472-5
27. Kemp WJ, Fulkerson DH, Payner TD, Leipzig TJ, Horner TG, Palmer EL. Risk of hemorrhage from de novo cerebral aneurysms. J Neurosurg. 2013. 118: 58-62
28. Koyama S. Giant aneurysm of the pericallosal artery causing acute subdural hematoma – Case report. Neurol Med Chir (Tokyo). 2000. 40: 268-71
29. Lai LT, Morgan MK, Patel NJ. Smoking increases the risk of de novo intracranial aneurysms. World Neurosurg. 2014. 82: e195-201
30. Laitinen L, Snellman A. Aneurysms of the pericallosal artery: A study of 14 cases verified angiographically and treated mainly by direct surgical attack. J Neurosurg. 1960. 17: 447-58
31. Lehecka M, Porras M, Dashti R, Niemelä M, Hernesniemi JA. Anatomic features of distal anterior cerebral artery aneurysms: A detailed angiographic analysis of 101 patients. Neurosurgery. 2008. 63: 219-28
32. Maiuri F, Corriero G, D’Amico L, Simonetti L. Giant aneurysm of the pericallosal artery. Neurosurgery. 1990. 26: 703-6
33. McTaggart RA, Santarelli JG, Marcellus ML, Steinberg GK, Dodd RL, Do HM. Delayed retraction of the pipeline embolization device and corking failure: Pitfalls of pipeline embolization device placement in the setting of a ruptured aneurysm. Neurosurgery. 2013. 72: onsE245-50
34. Meng H, Wang Z, Hoi Y, Gao L, Metaxa E, Swartz DD. Complex hemodynamics at the apex of an arterial bifurcation induces vascular remodeling resembling cerebral aneurysm initiation. Stroke. 2007. 38: 1924-31
35. Miller CA, Hill SA, Hunt WE. “De novo” aneurysms. A clinical review. Surg Neurol. 1985. 24: 173-80
36. Mishima K, Watanabe T, Sasaki T, Saito I, Takakura K. An infected partially thrombosed giant aneurysm of the azygos anterior cerebral artery. No Shinkei Geka. 1990. 18: 475-81
37. Miyazawa N, Nukui H, Yagi S, Yamagata Z, Horikoshi T, Yagishita T. Statistical analysis of factors affecting the outcome of patients with ruptured distal anterior cerebral artery aneurysms. Acta Neurochir (Wien). 2000. 142: 1241-6
38. Niiro M, Shimozuru T, Nakamura K, Kadota K, Kuratsu J. Long-term follow-up study of patients with cavernous sinus aneurysm treated by proximal occlusion. Neurol Med Chir (Tokyo). 2000. 40: 88-96
39. Nitta T, Nakajima K, Maeda M, Ishii S. Completely thrombosed giant aneurysm of the pericallosal artery: Case report. J Comput Tomogr. 1987. 11: 140-3
40. Nussbaum ES, Erickson DL. The fate of intracranial microaneurysms treated with bipolar electrocoagulation and parent vessel reinforcement. Neurosurgery. 1999. 45: 1172-4
41. Ohno K, Monma S, Suzuki R, Masaoka H, Matsushima Y, Hirakawa K. Saccular aneurysms of the distal anterior cerebral artery. Neurosurgery. 1990. 27: 907-12
42. O’Neill M, Hope T, Thomson G. Giant intracranial aneurysms: Diagnosis with special reference to computerised tomography. Clin Radiol. 1980. 31: 27-39
43. Pia HW, Zierski J. Giant cerebral aneurysms. Neurosurg Rev. 1982. 5: 117-48
44. Pozzati E, Nuzzo G, Gaist G. Giant aneurysm of the pericallosal artery. Case report. J Neurosurg. 1982. 57: 566-9
45. Preul M, Tampieri D, Leblanc R. Giant aneurysm of the distal anterior cerebral artery: Associated with an anterior communicating artery aneurysm and a dural arteriovenous fistula. Surg Neurol. 1992. 38: 347-52
46. Proust F, Toussaint P, Hannequin D, Rabenenoïna C, Le Gars D, Fréger P. Outcome in 43 patients with distal anterior cerebral artery aneurysms. Stroke. 1997. 28: 2405-9
47. Puri A, Massari F, Hou S, Perras M, Brooks C, Stout C. E-042 use of flow diverters in vessels less than 2.5 mm during intracranial aneurym treatment. J Neurointerv Surg. 2014. 6: A1-78
48. Sakaki T, Tominaga M, Miyamoto K, Tsunoda S, Hiasa Y. Clinical studies of de novo aneurysms. Neurosurgery. 1993. 32: 512-6
49. Sekhar LN, Heros RC. Origin, growth, and rupture of saccular aneurysms: A review. Neurosurgery. 1981. 8: 248-60
50. Shiokawa K, Tanikawa T, Satoh K, Kawamata T, Kubo O, Kagawa M. Two cases of giant aneurysms arising from the distal segment of the anterior cerebral circulation. No Shinkei Geka. 1993. 21: 467-72
51. Sindou M, Pelissou-Guyotat I, Mertens P, Keravel Y, Athayde AA. Pericallosal aneurysms. Surg Neurol. 1988. 30: 434-40
52. Smith RR, Parent AD. End-to-end anastomosis of the anterior cerebral artery after excision of a giant aneurysm. Case report. J Neurosurg. 1982. 56: 577-80
53. Snyckers FD, Drake CG. Aneurysms of the distal anterior cerebral artery. A report on 24 verified cases. S Afr Med J. 1973. 47: 1787-91
54. Steven DA, Lownie SP, Ferguson GG. Aneurysms of the distal anterior cerebral artery: Results in 59 consecutively managed patients. Neurosurgery. 2007. 60: 227-33
55. Szikora I, Marosfoi M, Salomváry B, Berentei Z, Gubucz I. Resolution of mass effect and compression symptoms following endoluminal flow diversion for the treatment of intracranial aneurysms. AJNR Am J Neuroradiol. 2013. 34: 935-9
56. Timperman PE, Tomsick TA, Tew JM, van Loveren HR. Aneurysm formation after carotid occlusion. AJNR Am J Neuroradiol. 1995. 16: 329-31
57. Tomsick T. Long-term clinical follow-up of therapeutic internal carotid artery occlusion. AJNR Am J Neuroradiol. 2007. 28: 1626-
58. Tonn J, Hoffmann O, Hofmann E, Schlake HP, Sörensen N, Roosen K. “De novo” formation of intracranial aneurysms: Who is at risk?. Neuroradiology. 1999. 41: 674-9
59. Topsakal C, Ozveren MF, Erol FS, Cihangiroglu M, Cetin H. Giant aneurysm of the azygos pericallosal artery: Case report and review of the literature. Surg Neurol. 2003. 60: 524-33
60. Tsutsumi K, Ueki K, Morita A, Usui M, Kirino T. Risk of aneurysm recurrence in patients with clipped cerebral aneurysms: Results of long-term follow-up angiography. Stroke. 2001. 32: 1191-4
61. Türe U, Hiçdönmez T, Elmaci I, Peker S. Giant pericallosal artery aneurysm: Case report and review of the literature. Neurosurg Rev. 2001. 24: 151-5
62. Wang JY, Smith R, Ye X, Yang W, Caplan JM, Radvany MG. Serial imaging surveillance for patients with a history of intracranial aneurysm: Risk of de novo aneurysm formation. Neurosurgery. 2015. 77: 32-42
63. Wermer MJ, van der Schaaf IC, Velthuis BK, Algra A, Buskens E, Rinkel GJ. Follow-up screening after subarachnoid haemorrhage: Frequency and determinants of new aneurysms and enlargement of existing aneurysms. Brain. 2005. 128: 2421-9
64. Winn HR, Richardson AE, Jane JA. Late morbidity and mortality of common carotid ligation for posterior communicating aneurysms. A comparison to conservative treatment. J Neurosurg. 1977. 47: 727-36
65. Wisoff JH, Flamm ES. Aneurysms of the distal anterior cerebral artery and associated vascular anomalies. Neurosurgery. 1987. 20: 735-41
66. Yamagami T, Handa H, Hashimoto N, Nagata H, Watanabe H. Giant aneurysm of the azygos anterior cerebral artery. Nihon Geka Hokan. 1986. 55: 777-82
67. Yasargil M.editors. Aneurysm clipping. Microneurosurgery: Microsurgical Anatomy of the Basal Cisterns and Vessels of the Brain. Stuttgart: Georg Thieme; 1984. 1:
68. Yasargil MG, Carter LP. Saccular aneurysms of the distal anterior cerebral artery. J Neurosurg. 1974. 40: 218-23
69. Yoneoka Y, Takeda N, Akira I, Ibuchi Y, Kumagai T, Sugai T. Ruptured de novo intracranial aneurysms. Acta Neurochir (Wien). 2004. 146: 979-81
70. Yoshimoto T, Uchida K, Suzuki J. Surgical treatment of distal anterior cerebral artery aneurysms. J Neurosurg. 1979. 50: 40-4

