

- Department of Neurosurgery, National Hospital Organization Sendai Medical Center, Sendai, Miyagi, Japan.
- Department of Neurosurgery, Tohoku University Graduate School of Medicine, Sendai, Miyagi, Japan.
Correspondence Address:
Hiroyuki Sakata, Department of Neurosurgery, National Hospital Organization Sendai Medical Center, Sendai, Miyagi, Japan.
DOI:10.25259/SNI_1147_2021
Copyright: © 2022 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Takatsugu Abe1, Hiroyuki Sakata1, Masayuki Ezura1, Hidenori Endo1, Teiji Tominaga2. Direct carotid puncture for endovascular surgery of intracranial aneurysms: Technical note for avoiding complications. 25-Feb-2022;13:69
How to cite this URL: Takatsugu Abe1, Hiroyuki Sakata1, Masayuki Ezura1, Hidenori Endo1, Teiji Tominaga2. Direct carotid puncture for endovascular surgery of intracranial aneurysms: Technical note for avoiding complications. 25-Feb-2022;13:69. Available from: https://surgicalneurologyint.com/?post_type=surgicalint_articles&p=11412
Date of Submission
16-Nov-2021
Date of Acceptance
02-Feb-2022
Date of Web Publication
25-Feb-2022
Abstract
Background: While the most intracranial aneurysms are approachable by femoral or brachial artery puncture during endovascular surgery, in some cases, the lesion is difficult to reach due to complications such as the presence of winding pathways. Direct carotid puncture (DCP) is an alternative access approach, despite the potential risk of fatal neck hematoma. Herein, we describe the DCP technique in a series of five patients with intracranial aneurysms, together with its technical considerations.
Methods: Patients with intracranial aneurysms who underwent endovascular surgery using DCP were reviewed retrospectively. We selected the 3F to 6F systems for DCP depending on the necessity of adjunctive techniques. To prevent DCP-associated complications, we (1) conducted a micropuncture before introducing the short sheaths,
Results: Five out of 535 patients underwent DCP in our hospital between 2015 and 2019; successful vascular access was achieved in all cases. Although a minor neck hematoma occurred in one case, the patient did not require additional treatment. According to a literature review, severe neck hematoma requiring rescue therapy occurs in 5 out of 95 cases (5.3%).
Conclusion: Although the potential risk of neck hematoma is not negligible, the DCP technique appears to be a safe and effective approach in treating intracranial aneurysms with challenging access routes in cases where perioperative counter measurements are appropriately performed.
Keywords: Direct carotid puncture, Intracranial aneurysm, Neuroendovascular treatment
INTRODUCTION
Endovascular surgery is a minimally invasive method for the treatment of intracranial aneurysms.[
MATERIALS AND METHODS
Study population
Subjects were identified through an electronic medical record search for all patients with intracranial aneurysms who underwent endovascular surgery between 2015 and 2019 at our hospital. Patients who needed the DCP approach were included in the study. Approval to conduct, this study was received from the Institutional Review Board of our hospital. All medical records and information were anonymized and identified just before analysis.
DCP procedures
All procedures were performed under general anesthesia with the patient’s neck in an extended position. We first performed cerebral angiography through femoral approach in all cases and decided whether a guiding catheter could be placed through the femoral approach. If it seems difficult, we switched to DCP. The activated clotting time was maintained at 200–250 s during the procedure. For the DCP technique, the CCA was punctured percutaneously using a Metrik MAKTM Mini Access Kit (21-gauge needle and 0.018 guide wire) (Merit Medical, Utah, USA) for micropuncture followed by the insertion of a guidewire into the internal carotid artery (ICA) under radiographic guidance. We performed DCP by palpation-guided punctures. The following sheaths were then introduced into the ICA: (1) for coil embolization using a simple technique, we selected a 3F–4F system: SURFLO® IV Catheter 18-gauge (Terumo Corporation, Tokyo, Japan) (approximately 3F or 4F short sheath attached to an injector tube and a Y-connector). The inserted sheath was secured with sterile tape, which prevented it from coming out accidentally. (2) For coil embolization using an adjunctive technique, we chose a 5F system: a 5F short sheath attached to a two-way adapter (RS-VA284, Terumo Corporation, Tokyo, Japan) to secure the two-way route. (3) Finally, for flow diverter stenting, we selected a 6F system. While using the 3–4F system for coil embolization with the simple technique, we also performed common carotid angiograms with a 4F catheter placed at the origin of the CCA through the transfemoral approach. We reversed the effects of heparin with protamine sulfate immediately after surgery and proceeded with manual compression hemostasis. Protamine dosage was determined based on the heparin dosage received (10 mg/1000 units of heparin), not to exceed 50 mg. Finally, we provided perioperative intubation/sedation control to patients until the next day. The intubation tube was removed after confirming the complete hemostasis of the punctured CCA.
Literature review
To elucidate the potential risk of the DCP technique in patients with intracranial aneurysms, we performed a literature review, searching the publications on PubMed with the keywords “intracranial aneurysm” and “direct puncture” OR “DCP.” After the cases of cerebral aneurysms accessed by DCP were selected, we assessed the perioperative management as well as the complications due to DCP.
RESULTS
A total of 535 patients underwent endovascular surgery for intracranial aneurysms in our hospital between 2015 and 2019. Among them, 5 cases (0.93%) were treated using the DCP technique. [
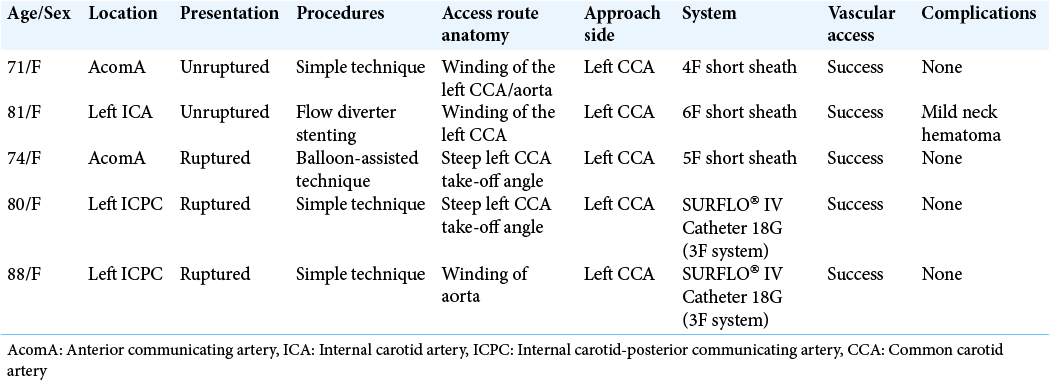
The patients’ ages ranged from 71 to 88 years. All the patients were women. There were two cases of anterior communicating artery aneurysm and three cases of internal carotid-posterior communicating artery aneurysm. We treated two cases of unruptured and three cases of ruptured aneurysms. All the punctures were performed on the left CCA due to the challenging access routes, such as the winding course of the CCA or aorta and the steep left CCA take-off angle. For coil embolization with the simple technique, the 4F system was used in one case and the 3F system (SURFLO® 18-gauge IV catheter) was chosen in two cases.
We achieved successful vascular access in all cases, which resulted in successful embolization. Computed tomography immediately after the procedure revealed no hemorrhagic complication in all cases. Magnetic resonance imaging was performed in all patients on postoperative days 2–4, revealing an asymptomatic small infarct in one case. Postoperative neurological deterioration was not observed in all cases. A direct DCP-related complication was observed in one case as mild neck hematoma postoperatively, which did not require additional treatment.
Results of the literature review
There were reports of 95 patients with intracranial aneurysms accessed by DCP, including our cases, as shown in [
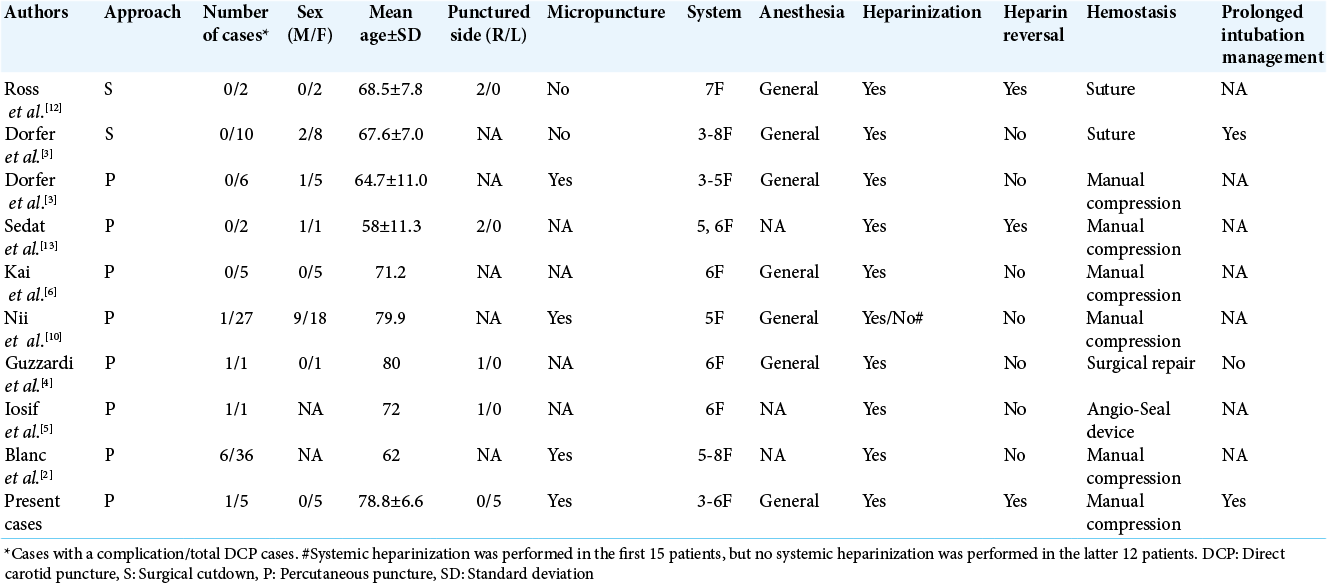
[
DISCUSSION
We attempted the DCP technique in patients in whom vascular access through the femoral or brachial approach was difficult. In the cases presented here, aortic arch anomalies, including the winding course of the CCA or aorta and the steep left CCA take-off angle, hampered access to the ICA through the conventional approach. According to other reports, aortic dissection and iliac occlusive disease could be other indications for using DCP.[
The appropriate choice of the system for the DCP technique is necessary to avoid complications. Blanc et al. previously reported the effectiveness of DCP for anterior circulation aneurysms when performing coil embolization.[
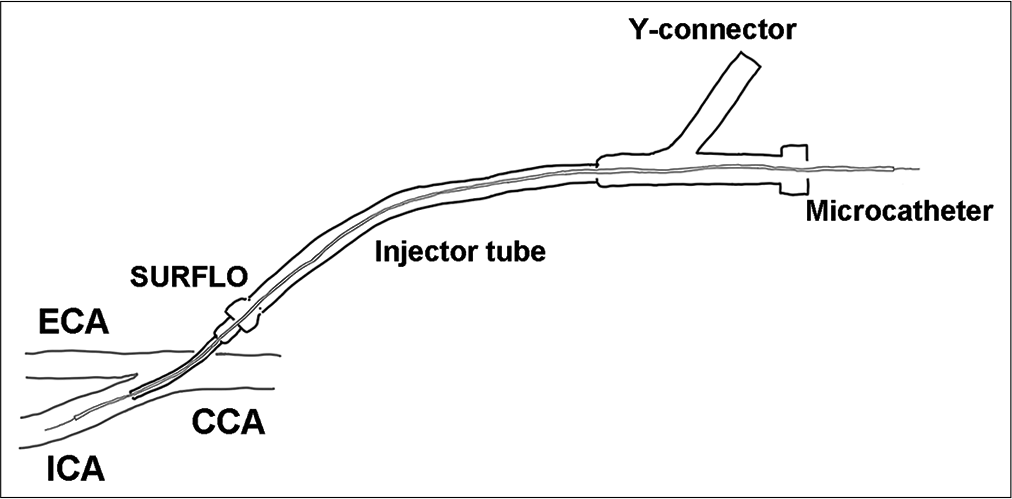
Figure 1:
The illustration shows a representative 3F direct carotid puncture system for coil embolization with the simple technique. The SURFLO® 18-gauge IV catheter (approximately of the 3F system) is inserted into the common carotid artery and then connected to the Y-connector attached injector tube.
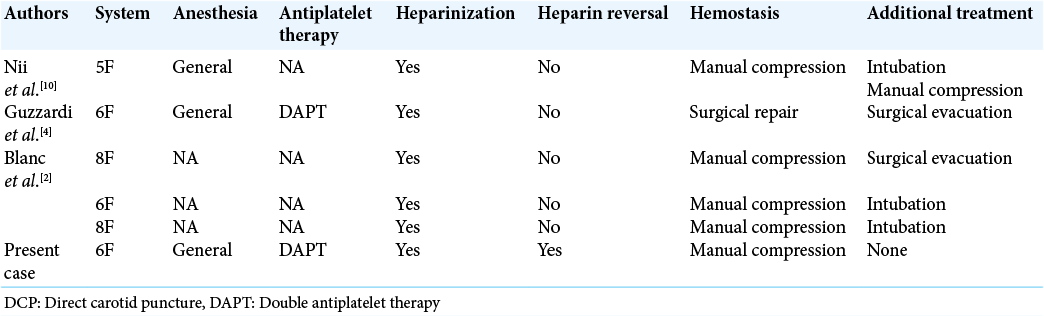
The most severe direct complication associated with the DCP technique is hemostasis failure, which might result in airway obstruction. Five out of six neck hematoma cases in the literature review needed additional treatment [
CONCLUSION
Based on our experience and previous reports, we consider that if appropriate countermeasures are taken, the DCP technique would be a safe and effective approach to treat intracranial aneurysms that are anatomically difficult to access. In particular, it is important to select a small-diameter system, perform heparin reversal, and manage prolonged intubation/sedation control.
Declaration of patient consent
Institutional Review Board (IRB) permission obtained for the study.
Financial support and sponsorship
JSPS KAKENHI (Grant Number JP19K18414).
Conflicts of interest
There are no conflicts of interest.
References
1. Akpinar CK, Gurkas E, Aykac O, Inanc Y, Giray S, Ozdemir AO. Direct common carotid artery puncture: Rescue mechanical thrombectomy strategy in acute ischemic stroke. Neurointervention. 2020. 15: 60-6
2. Blanc R, Piotin M, Mounayer C, Spelle L, Moret J. Direct cervical arterial access for intracranial endovascular treatment. Neuroradiology. 2006. 48: 925-9
3. Dorfer C, Standhardt H, Gruber A, Ferraz-Leite H, Knosp E, Bavinzski G. Direct percutaneous puncture approach versus surgical cutdown technique for intracranial neuroendovascular procedures: Technical aspects. World Neurosurg. 2012. 77: 192-200
4. Guzzardi G, Del Sette B, Stanca C, Paladini A, Galbiati A, Spinetta M. Intracranial carotid artery aneurysm treatment: First reported case of DERIVO ® flow-diverter placement by direct carotid artery puncture. Brain Sci. 2020. 10: 320
5. Iosif C, Clarençon F, di Maria F, Law-Ye B, le Jean L, Capelle L. Combined Angio-SealTM and stenting rescue treatment in a case of iatrogenic common carotid artery dissection during direct puncture for ruptured intracranial aneurysm embolization: A technical note. J Neurorad. 2013. 40: 130-3
6. Kai Y, Hamada J, Morioka M, Yano S, Mizuno T, Kuratsu J. Double microcatheter technique for endovascular coiling of wide-neck aneurysms using a new guiding device for the transcarotid approach: Technical note. Neuroradiology. 2005. 47: 73-7
7. Lam RC, Lin SC, DeRubertis B, Hynecek R, Kent KC, Faries PL. The impact of increasing age on anatomic factors affecting carotid angioplasty and stenting. J Vasc Surg. 2007. 45: 875-80
8. Miszczuk M, Bauknecht HC, Kleine JF, Liebig T, Bohner G, Siebert E. Direct puncture of the carotid artery as a bailout vascular access technique for mechanical thrombectomy in acute ischemic stroke-The revival of an old technique in a modern setting. Neuroradiology. 2021. 63: 275-83
9. Molyneux AJ, Birks J, Clarke A, Sneade M, Kerr RS. The durability of endovascular coiling versus neurosurgical clipping of ruptured cerebral aneurysms: 18 year follow-up of the UK cohort of the international subarachnoid aneurysm trial (ISAT). Lancet. 2015. 385: 691-7
10. Nii K, Kazekawa K, Onizuka M, Aikawa H, Tsutsumi M, Tomokiyo M. Direct carotid puncture for the endovascular treatment of anterior circulation aneurysms. AJNR Am J Neurorad. 2006. 27: 1502-4
11. Ribo M, Flores A, Rubiera M, Pagola J, Mendonca N, Rodriguez-Luna D. Difficult catheter access to the occluded vessel during endovascular treatment of acute ischemic stroke is associated with worse clinical outcome. J Neurointervent Surg. 2013. 5: i70-3
12. Ross IB, Luzardo GD. Direct access to the carotid circulation by cut down for endovascular neuro-interventions. Surg Neurol. 2006. 65: 207-11
13. Sedat J, Chau Y, Litrico S, Rasandrarijao D, Lonjon M, Paquis P. Stretched platinum coil during cerebral aneurysm embolization after direct carotid puncture: Two case reports. Cardiovasc Intervent Radiol. 2007. 30: 1248-51
14. Spetzler RF, McDougall CG, Zabramski JM, Albuquerque FC, Hills NK, Nakaji P. Ten-year analysis of saccular aneurysms in the Barrow Ruptured aneurysm trial. J Neurosurg. 2019. 132: 771-6
15. Styczen H, Behme D, Hesse AC, Psychogios MN. Alternative transcarotid approach for endovascular treatment of acute ischemic stroke patients: A case series. Neurointervention. 2019. 14: 131-6

